
Abstract
The bidirectional association between psychiatric conditions and medical illnesses has been studied for many different diseases. Unfortunately, prospective studies, which can address causation, are quite heterogeneous in terms of clinical populations, methods, and measures. One example, among many potential others, is the relationship between depression and type 2 diabetes mellitus (or its correlates), which has been studied extensively using longitudinal designs (Golden et al., 2008; Mezuk, Eaton, Albrecht, & Golden, 2008; Pan et al., 2010). The collective result generally confirms the suspected reciprocal nature of this specific association, despite the variation in the techniques, including populations (gender, ethnicity, location), methods (time of follow-up), and measures (symptom scales, self-report, clinical diagnosis) used to assess the magnitude and direction of the causal paths.
There exist other previously suggested correlations of psychiatric conditions with medical comorbidity diseases, including epilepsy (Adelöw, Andersson, Ahlbom, & Tomson, 2012; Hesdorffer et al., 2012; Thapar, Roland, & Harold, 2005), arthritis (El-Gabalawy, Mackenzie, Pietrzak, & Sareen, 2014; van’t Land et al., 2010), vascular conditions (Fiedorowicz, He, & Merikangas, 2011; Janszky, Ahnve, Lundberg, & Hemmingsson, 2010), cancer (Currier & Nemeroff, 2014), and pulmonary dysfunction (Jain & Lolak, 2009). However, the oversight present in many of these listed inquiries is the juxtaposition among diseases and conditions which are correlated with one or more psychiatric disorders. Three established examples include pulmonary diseases co-existing with vascular conditions (Chatila, Thomashow, Minai, Criner, & Make, 2008), some cancers correlating with an arthritic diagnosis (Chen, Chang, Wang, & Wu, 2011), and undiagnosed diabetes mellitus among individuals with an identified vascular disease (Bartnik et al., 2004). Hence, it may be necessary to comprehensively control for the presence of non-psychiatric comorbidities when investigating the bidirectional role of psychiatric condition on the prevalence and incidence of these medical illnesses. The goal of the present work is to determine the risk of reporting a medical comorbidity in relation to incidence of psychiatric condition, controlling for the potential multimorbidity that may exist.
Figure 1 represents the base conceptual model for the inquiry. The model describes the bidirectional nature of the analysis. That is, the prevalence of any one or more medical comorbidities may predict incident psychiatric condition, which may also foretell subsequent burden of any one or more medical comorbidities. Specifically, the hypothesis which is tested is the following: controlling for the wave of assessment, mean age, gender and race of the survey participants, and the presence of medical multimorbidity ni (where i = 1, 2, . . . , 6 and represents comorbid medical condition), the risks of reporting comorbidity m (where m ≠ ni) increases with each passing wave both before and after first reporting a psychiatric condition. Note that I use the terms comorbidity and multimorbidity differently. Comorbidity refers to a medical condition whose association with an incident psychiatric condition is of interest. Multimorbidity refers to medical conditions whose presence might represent confounders. Empirically, comorbidities are the dependent variables and multimorbidities are covariates.

Conceptual model.
The contributions of this work inform the literature in several ways. First, I am able to robustly test the bidirectional association of psychiatric conditions and medical illnesses by controlling for the presence of non-psychiatric multimorbidity. Second, the longitudinal design incorporates observations spanning two decades (1992-2012), which is among the longest time horizons in the extant literature investigating comorbidities among individuals with psychiatric condition. Third, although the Health and Retirement Study (HRS) data I use are based on self-report, there are a number of attributes that may minimize, although not completely eliminate, the recall and disease severity biases associated with such data collection: (a) Survey participants were asked to recall new diagnoses since the previous wave, which is generally limited to a 2-year recall span, and (b) data were accumulated based on participants’ recollection of a doctor’s diagnosis instead of reliance on scales measuring disease symptoms or self-report in the absence of medical confirmation. Although these factors still represent limitations, their impact should be viewed in light of the comprehensiveness of the proposed inquiry, including its long duration of follow-up and multimorbidity angle encompassing eight total disease classifications.
Method
I used the publicly available RAND data (Version N) for all 11 available waves of the HRS, spanning the years 1992 to 2012. The HRS is a national panel study with the initial respondents in 1992 being persons born during 1931 to 1941. The HRS over-samples Blacks, Hispanics, and Florida residents, but otherwise is representative of the U.S. population of this age. It contains measures of preferences and detailed financial, demographic, and health data, including data on health conditions existing at study entry and incident health conditions (Juster & Suzman, 1995).
First, I identified the wave in which the participants first reported a psychiatric condition as the index wave. The self-report was based on whether a doctor had ever told the respondent that he or she has ever had a particular disease. An incident case of a psychiatric condition was defined as responding “yes” to whether a doctor had ever told them they had emotional, nervous, or psychiatric problems and not previously reporting a psychiatric condition during participation in the HRS and not entering HRS with a reported psychiatric condition. I refer to this as incident psychiatric condition, with the important caveat that condition, as defined here, likely includes subclinical psychiatric impairments. Second, for each index cohort (based on wave of incident psychiatric condition), I collected comorbidity data from each non-index wave for each participant. Medical comorbidities assessed included high blood pressure (HBP), diabetes mellitus, cancer, lung disease, heart disease, stroke, and arthritis, a disease grouping within the HRS that has been used before (Weston, Hill, & Jackson, 2014). Individuals with contradictory or disputed disease outcomes were excluded from the analyses.
Log-binomial models were used to estimate relative risks (RRs) and confidence intervals (CIs; Skov, Deddens, Petersen, & Endahl, 1998; Wacholder, 1986). In a few instances, it is possible that these models may not converge. In those cases, log-Poisson models, which provide consistent but not fully efficient estimates of the RR and its CIs, are used (Zou, 2004) to estimate RRs of reporting a comorbidity preceding and following the incident wave. The main effect of interest was time before or after the wave in which incident psychiatric condition was reported. The models may be written as

where
The analysis was performed using SAS Software, Version 9.4. In all regressions, a multiple testing correction was used to assess the significance of the time covariate, the variable of most interest. Given seven total medical comorbidities, a p value of .05/7 = .007 is the cutoff to determine statistical significance of the estimated coefficients.
Results
Figure 2 presents the data in terms of incident psychiatric condition. Over the 10 waves, there were 4,358 individuals reporting incident psychiatric condition, with an average of 436 individuals per wave. All individuals reporting prevalent psychiatric condition were removed from the analysis. This included 100% of the individuals reporting psychiatric condition in the first wave. Among subsequent waves, the proportion of individuals reporting psychiatric condition who were also categorized as incident cases ranged from a high of 30% in Wave 2 to 8% in Wave 10. A trend analysis for proportions on wave revealed a significantly negative trend (slope = −0.02, SE = 0.0007, Z = 21.49).
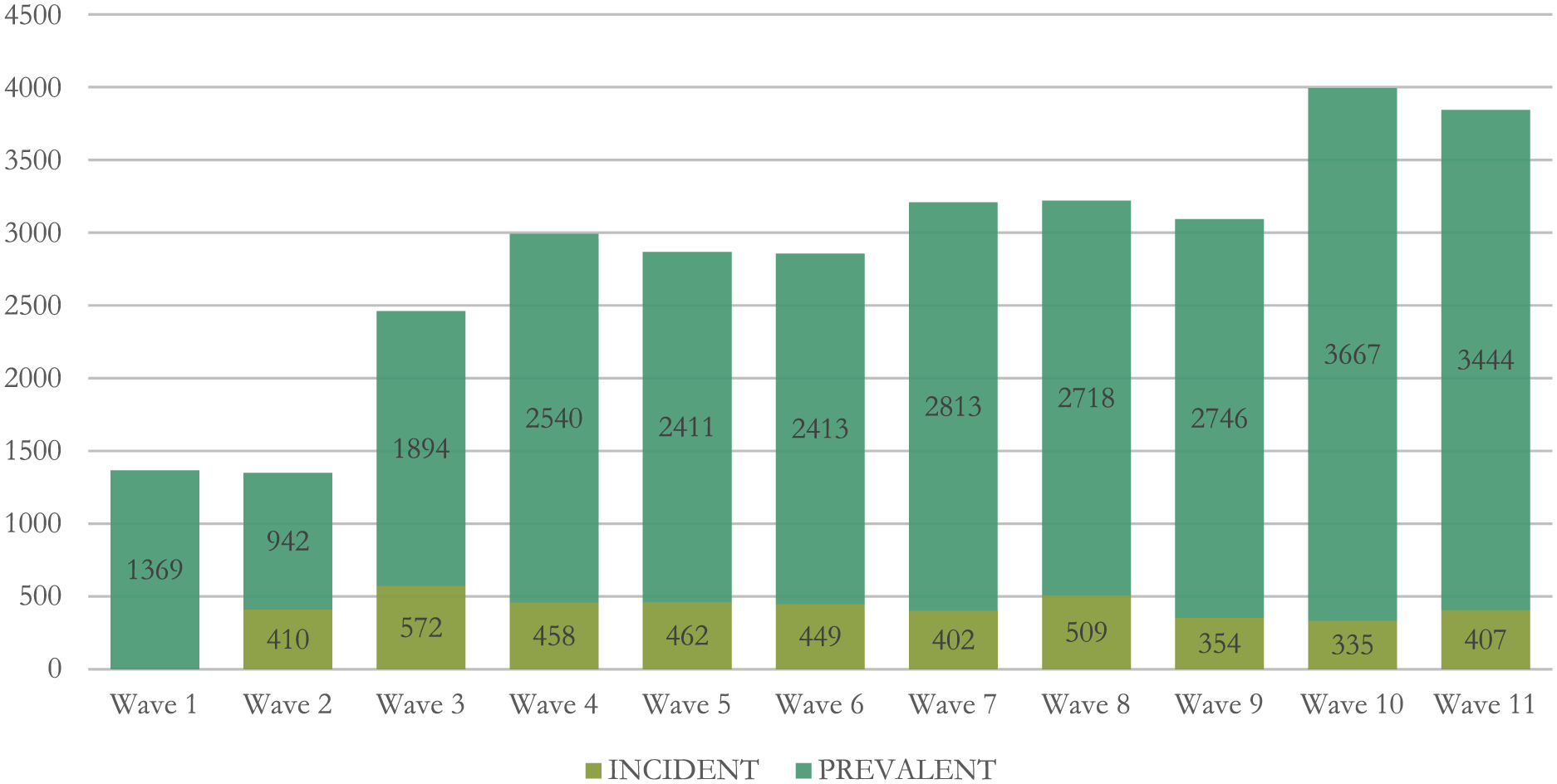
Number of incident versus prevalent cases of psychiatric illness by HRS wave.
Table 1 gives the comorbidity frequencies and their percentages relative to incident psychiatric condition. In the pre-incident period, there were 4,358 individuals with 24,345 self-reports available regarding comorbidities. In the post-incident period, there were 3,952 unique individuals with 31,306 reports available regarding comorbidities. For both periods, reports of HBP and arthritis were common (> 50% of total reports), whereas stroke was the least frequently reported comorbidity (6.2% and 11.5% in the pre- and post-incident periods). The numbers in parentheses reflect the reports and percentages of each outcome with full information known. For example, there were 6,787 self-reports of HBP in the pre-incident period for which data on all other comorbidities and demographics were also known. Therefore, these numbers reflect the analyzable data. In most cases (except HBP), the analyzable sample of reports did not differ from the available reports by more than 1 percentage point in either the pre- or post-incident periods. Of particular concern is the proportional increase in the numbers of participants reporting any outcome from the pre- to post-incident periods: a roughly 10-point increase for all but two comorbidities (cancer and stroke).
Comorbidity Self-Reports Relative to Incident Psychiatric Condition.

Note. Comorbidities reported at the incident wave (time = 0) are not included in these frequencies. Numbers in parentheses represent the numbers and percentage of total self-reports for each comorbidity that were retained in the regression models.
Table 2 displays the demographic characteristics of HRS respondents’ comorbidity reports, segmented by age, race, and gender. In the pre-incident period, White participants comprise 86.3% of all self-reports of lung cancer, the highest among any comorbidity, whereas in the post-incident period, White respondents constitute 87.9% of all cancer self-reports. Males self-report stroke as the most frequent comorbidity in both periods, whereas females identify arthritis and HBP most often in the pre- and post-incident periods, respectively. The difference in mean ages of all self-reports was most notable between White and non-White participants: non-Whites were roughly four years younger, on average, than Whites in self-reporting most comorbidities, a difference that dropped by more than half in the post-incident period.
Demographic Characteristics of Comorbidity Reports, by Age, Gender, and Race.

Note. HBP = high blood pressure.
Table 3 presents the main results using either the modified Poisson regression model or both the Poisson and log-linked binomial models. As noted in the table, convergence issues led to use of only the modified Poisson model for the outcomes of HBP, heart disease, and arthritis. For the pre-incident period (S = 1), five medical comorbidities were significantly and increasingly reported with each wave before incident psychiatric condition: diabetes (RR: 1.07, 95% CI: [1.04, 1.10]), lung disease (RR: 1.14, 95% CI: [1.10, 1.19]), heart disease (RR: 1.10, 95% CI: [1.07, 1.13]), stroke (RR: 1.18, 95% CI: [1.11, 1.25]), and arthritis (RR: 1.03, 95% CI: [1.01, 1.04]). In the post-incident period (S = 2), three medical comorbidities were significantly and increasingly reported with each wave after incident psychiatric condition: diabetes (RR: 1.05, 95% CI: [1.03, 1.08]), lung disease (RR: 1.07, 95% CI: [1.03, 1.10]), and heart disease (RR: 1.03, 95% CI: [1.01, 1.05]). The risk of self-reporting diabetes, lung disease, and heart disease increased with each wave in the pre- and post-incident periods. However, the risk for heart disease dropped significantly from the pre- to post-incident period.
Relative Risk Estimation by Modified Poisson & Binomial Regressions.

Note. Each outcome is modeled controlling for the other listed conditions as well as age, race, and gender. CI = confidence interval.
Binary response was fit using Poisson model only, as the log-linked binomial model failed to converge. For all other outcomes, the binary response was fit using Poisson model to obtain initial estimates for the log-linked binomial model (presented).
p < .007.
Post hoc sensitivity analyses were conducted on the three comorbidities with significant risks of being self-reported in the pre- and post-incident periods (diabetes, lung disease, and heart disease). To do so, I included two additional covariates with generally known behavioral associations to disease risk: body mass index (BMI) and smoking status (yes/no). Data on both behavioral phenotypes were collected in the HRS at each wave and therefore changed across the follow-up. For the pre-incident self-reports, mean values of BMI and smoking status were 27.4 (SD = 13.0) and 0.19 (SD = 0.23), respectively. For the post-incident self-reports, corresponding summary statistics were 28.1 (SD = 12.8) and 0.15 (SD = 0.20).
Table 4 presents the results of the sensitivity analyses. Including these variables made no appreciable impact on the original set of findings. However, with this further adjustment, the risk of self-reporting lung disease and heart disease significantly declined (although still positive) with each wave in the post-incident period as compared with the pre-incident period (RR: 1.15, 95% CI: [1.11,1.20] and RR: 1.06, 95% CI:[1.03,1.09] for lung disease; RR: 1.10, 95% CI: [1.07,1.13] and RR: 1.03, 95% CI:[1.01,1.05] for heart disease). The same was not observed with diabetes. Thus, overall, incident psychiatric condition made no difference in the risk of self-reporting diabetes in an aging cohort. The risk of reporting all other comorbidities was either not associated with incident psychiatric condition (e.g., HBP, cancer) or significantly reduced from the pre- to post-incident period (e.g., lung disease, heart disease, stroke, and arthritis).
Relative Risk Estimation by Modified Poisson and Binomial Regressions, Additionally Controlling for BMI and Smoking Status.

Note. BMI = body mass index; CI = confidence interval.
Binary response was fit using Poisson model only, as the log-linked binomial model failed to converge. For all other outcomes, the binary response was fit using Poisson model to obtain initial estimates for the log-linked binomial model (presented).
p < .007.
Discussion
The purpose of the present article is to comprehensively assess the bidirectional association between various medical comorbidities and incident psychiatric condition using the HRS. I showed using log-linked binomial regression analysis that lung disease, diabetes, and heart disease (with the modified Poisson approximation) 1 are the only medical comorbidities (among a list also including HBP, cancer, stroke, and arthritis) whose risk of self-report increases both before and after incident psychiatric condition. This association is robust to (a) the waves analyzed (which covers the period 1992 to 2012), (b) multimorbidity and age, gender, and race, and (c) a multiple testing correction.
The study of health care utilization among individuals with multiple chronic conditions has skyrocketed in the last decade (Glynn et al., 2011; Lehnert et al., 2011). This multimorbidity—the existence of several chronic health disorders in one individual—has essentially become the new norm (Marengoni et al., 2011), especially among older individuals (G. Anderson, 2010; Salive, 2013). Multimorbidity predicts greater health care use, especially in the presence of a mental health condition (Bähler, Huber, Brüngger, & Reich, 2015; Harlow, 1997; Harlow, Johnson, & Callen, 1993; Hodgkins, Montejano, Sasané, & Huse, 2011; Lacruz et al., 2012). Multimorbidity also increases the likelihood that an individual has or develops a mental health illness (Barnett et al., 2012; Neeleman, Ormel, & Bijl, 2001). This work isolates those comorbidities bidirectionally associated with a psychiatric condition in the aim of further examining health care utilization associated with treatment of these comorbidities over time and controlling for multimorbidity to more accurately assess the impact of a psychiatric condition on use.
The potential explanations for the association between diabetes, lung disease, and incident psychiatric condition are numerous. Recent research has uncovered a link between diabetes and statin use (Cederberg et al., 2015; Culver et al., 2012; Sattar et al., 2010), which has been increasing in recent years (Mann, Reynolds, Smith, & Muntner, 2008). Statin use has also been associated with reduced risk of psychiatric illness (Redlich et al., 2014; Young-Xu, Chan, Liao, Ravid, & Blatt, 2003). A post hoc trend analysis of the diabetes proportion among individuals with incident psychiatric condition revealed a significantly positive trend (slope = 0.02, SE = 0.002, Z = 8.40). Thus, the collective trend analyses do comport with the use of statins in explaining the rise and fall in diabetes prevalence and incident psychiatric condition, respectively. The evidence of the influence of statin use on lung disease, specifically interstitial lung disease, has been mixed, however (Saad, Camus, Suissa, & Ernst, 2013; Xu et al., 2012).
Previous work has suggested a genetic correlate, a potentially pleiotropic effect, as one explanation for the comorbidity between diabetes mellitus and psychiatric illnesses (Cassidy, Ahearn, & Carroll, 1999). An example of such an effect is the link between insulin resistance and depression to a polymorphism in the tyrosine hydroxylase (TH) gene, specifically the TCAT tetranucleotide repeat microsatellite (HUMTH01; Chiba et al., 2000), which may regulate the gene’s transcription (Meloni, Albanèse, Ravassard, Treilhou, & Mallet, 1998). This polymorphism has also been inconsistently linked to psychiatric conditions (Burgert, Crocq, Bausch, Macher, & Morris-Rosendahl, 1998; Meloni, Laurent et al., 1995; Meloni, Leboyer et al., 1995). The putative transcription factor zinc finger protein 191 (ZNF 191) binds the TCAT motif in proportion to the number of repeats present and could interfere in transcription regulation of the TH gene (Albanèse et al., 2001).
This transcription interference may be particularly problematic for individuals with a lung disease. Hypoxia stimulates TH gene expression in the carotid body (Czyzyk-Krzeska, Bayliss, Lawson, & Millhorn, 1992; Gonzalez, Kwok, Gibb, & Fidone, 1979, 1981; Kato, Yamaguchi-Yamada, & Yamamoto, 2010). This stimulation produces carotid body innervation (McDonald, 1981), which may itself influence the progression of diabetes and other heart-related ailments (Ribeiro et al., 2013). Hypoxia also induces TH gene expression in the locus coeruleus (Schmitt, Pequignot, Garcia, Pujol, & Pequignot, 1993), which has been noted in patients with major depression (Zhu et al., 1999). Use of antidepressants decreased expression of the TH gene in the locus coeruleus (Nestler, McMahon, Sabban, Tallman, & Duman, 1990).
Li et al. (2009) described ZNF 191 as a pleiotropic transcription factor, possibly influencing up to 1456 candidate genes, one of which includes the CTNNB1 (β-catenin) gene, a gene which may explain the growth of diabetes as a comorbidity in cancer (Chocarro-Calvo, García-Martínez, Ardila-González, De la Vieja, & García-Jiménez, 2013). ZNF 191 may activate the expression of β-catenin and its downstream target genes (Liu et al., 2012). β-catenin has been implicated in depression (Dias et al., 2014), glucose metabolism (Elghazi et al., 2012), and idiopathic pulmonary fibrosis (Chilosi et al., 2003).
It may be a useful endeavor to investigate the drivers that mitigate or propagate upregulation of the ZNF 191 gene. For example, a diet high in omega-3 fatty acids has been shown to downregulate the zinc finger protein 24 (ZNF 191) gene (Vedin et al., 2012). However, meta-analyses examining the effects of consumption of omega-3 fatty acids on improvements in depressive symptoms (Martins, 2009) or incidence of type 2 diabetes (Wu et al., 2012) did not reveal robustly positive effects, although protective effects for lung diseases have been replicated (Matsuyama et al., 2005; Shahar et al., 1994). Thus, research efforts specifically examining the propagation of ZNF 191 and its subsequent genetic cascade may yield better data on how to further interpret incidence of psychiatric condition and its most significantly tracked comorbidities of lung disease, heart disease, and diabetes mellitus in this data set. Statins represent one exogenous factor that may explain, in part, this association; statins have been associated with regulation of zinc finger transcription factors (Parmar et al., 2005; Tuomisto et al., 2008).
It is also possible that the bidirectional associations between the comorbidities with psychiatric condition may not be attributable (solely) to genetics. Long-standing environmental insults may be driving these results, generating an epigenetic effect. For one example, community water fluoridation has been suggested to influence both diabetes prevalence and lung disease. In another article, I have shown a significant and positive relationship between added water fluoridation and diabetes prevalence in the United States (Fluegge, 2016). Other research has indicated damage to lung tissue from oral fluoride exposure (Abdel-Gawad, Ashmawy, Zaki, & Abdel-Fatah, 2014; Aydin, Çiçek, Akdoğan, & Gökalp, 2003; Purohit et al., 1998). It is possible that the increased risk of self-reporting lung disease and/or diabetes across the 20-year study period is, in fact, an artifact to incident psychiatric condition. This more expansive causal view may be particularly insightful for the diabetes outcome, whose risk of self-report did not wane at all in this analysis, regardless of the occurrence of an incident psychiatric condition, presence of medical multimorbidity, demographics or risky behaviors like smoking and obesity.
This analysis provides useful information to further advance the research and application of integrative physical and mental health care, particularly among older adults. The research findings highlight diabetes as perhaps the most problematic comorbidity. Although adults with psychiatric disorders are at high risk for diabetes (Engum, 2007; Knol et al., 2006), screening for the disease is less frequent than among adults without psychiatric impairment (Mangurian et al., 2015). The present longitudinal study shows that the risk of self-reporting diabetes after disclosing a psychiatric condition is essentially unchanged. This disparity from other research could be due to the older age of participants; Medicare Part B covers a screening blood sugar test to check for diabetes, whereas state Medicaid programs, for example, are more variable with respect to coverage for diabetes screening.
One of the obvious limitations with this study is the lack of specificity with respect to psychiatric condition. The public RAND data set was intentionally not inspected for specifics on this outcome. The goal at the beginning was only to distinguish medical comorbidities from psychiatric conditions. Nevertheless, it will be useful to isolate which psychiatric conditions specifically are tightly linked with the lung disease and/or diabetes mellitus comorbidities in relation to incidence of the psychiatric condition. Depression has been perhaps the most studied association (R. J. Anderson, Freedland, Clouse, & Lustman, 2001), due in part to the high costs of the comorbidity (Egede, Zheng, & Simpson, 2002; Park, Katon, & Wolf, 2013). The prevalence of depression may be largely driving the results seen here.
A second limitation is that these results may be an incorrect estimate of the true association between psychiatric condition and medical comorbidities. Given that my definition of psychiatric condition likely encompassed elements of both clinical psychiatric illness and subclinical psychiatric conditions, distinguishing between the two will be a useful exercise to replicate the findings presented here. However, psychological distress (not necessarily to the degree of a clinical disorder) has been associated with higher mortality from cardiovascular disease and cancer (Russ et al., 2012), lung disease (Pembroke, Rasul, Hart, Smith, & Stansfeld, 2006), and diabetes (Virtanen et al., 2014). Thus, it may be the case that these findings are impervious to the distinction between clinical psychiatric illness and subclinical psychiatric conditions.
Footnotes
Acknowledgements
The author wishes to thank Drs. Catherine Stein, Nicholas K. Schiltz and Mendel Singer for their insightful review and methodological contributions to this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH National Heart Lung and Blood Institute Grant T32HL007567.