
Abstract
We examined factors associated with incident (one) and recurrent (2+) falls among 7207 non-Hispanic White (NHW) (89.7%), non-Hispanic Black (NHB) (5.0%), and Hispanic (5.3%) men ages ≥60 years with ≥1 chronic conditions, enrolled in an evidence-based fall program. Multinomial and binary regression analyses were used to assess factors associated with incident and recurrent falls. Relative to zero falls, NHB and Hispanic men were less likely to report incident (OR = 0.55, p < .001 and OR = 0.70, p = .015, respectively) and recurrent (OR = 0.41, p < .001 and OR = 0.58, p < .001, respectively) falls. Men who reported fear of falling and restricting activities were more likely to report incident (OR = 1.16, p < .001 and OR = 1.32, p < .001, respectively) recurrent and (OR = 1.46, p < .001 and OR = 1.71, p < .001, respectively) falls. Men with more comorbidities were more likely to report recurrent falls (OR = 1.10, p < .001). Compared to those who experienced one fall, men who reported fear of falling (OR = 1.28, p < .001) and restricting activities (OR = 1.31, p < .001) were more likely to report recurrent falls. Findings highlight the importance of multi-component interventions to prevent falls.
• Identifies the prevalence of incident and recurrent falls among older males. • Compares falls prevalence and falls-related risk among three racial subgroups. • Highlights the effects of multimorbidity on recurrent fall risk.
• Informs researchers and practitioners about the associations between psychosocial factors and falls. • Suggests fall-related risk may be mitigated by chronic disease management and self-management interventions to manage disease symptomatology.What this paper adds
Applications of study findings
Background
Falls are a major public health issue and are the leading cause of unintentional injury, which is a major cause of mortality among older adults in the United States (Moreland & Lee, 2021). Out of the 2.4 million cases of unintentional injury that were seen in the emergency room (ER) in 2018, approximately 92% of them were due to falls (Moreland & Lee, 2021). Also, falls are the leading cause of death from unintentional injury among older adults (Kramarow et al., 2015). In 2018, out of a total of 57,213 deaths from unintentional injury among older adults, 32,522 deaths (56.8%) were attributed to falls (Centers for Disease Control and Prevention [CDC], 2021).
In 2018, roughly 28% of older adults in the United States reported at least one fall, and this rate followed a two-year decline (Moreland et al., 2020). Prior to the decline, between 2012 and 2016, significant increases in fall reporting in this population had been previously observed (Moreland et al., 2020). A 2014 estimate showed that approximately 29% of older adults reported at least a fall in that year (Bergen et al., 2016). Despite the slight decline in rates, healthcare costs from unintentional injuries due to falls are expected to increase, as the older adult population in the United States increases (Moreland et al., 2020). Recent findings also show that incidence has been increasing at the rate of 1.5% annually (Hoffman et al., 2022). Taking all these into account, the prevalence of falls among older adults has not significantly diminished (Bergen et al., 2016; Moreland et al., 2020).
The literature about falls consistently demonstrates that age/aging is a major risk factor for falls (Hartholt et al., 2019; Lohman et al., 2019). This is underscored by the fact that when compared to other common causes of injury, beyond ER visits, falls accounted for most of hospitalizations from unintentional injuries among older adults, and the frequency of visits among adults aged 85 years and older was approximately four times as high as those reported in the 65–74-year age group (Moreland & Lee, 2021). Chronic conditions, such as heart disease and cancer, are also factors that can complicate the risk of falls in older adults, especially among older adults with multiple comorbidities (Immonen et al., 2020; Kwon et al., 2018). In the presence of one or more chronic diseases, older adults tend to fall more frequently (Kwon et al., 2018), leading to increased recurrence. Other risk factors include, but are not limited to, behavioral, sociodemographic, social, and environmental factors.
Many studies reveal that fall-related risk is higher among women (Chang & Do, 2015; Moreland et al., 2020; Nicklett & Taylor, 2014; Sun et al., 2016; Verma et al., 2016); however, some studies have identified that rates of falls are increasing among men (Hartholt et al., 2012), men have higher fall-related risk (El Fakiri, 2015), and men have higher fall-related mortality rates (Ambrose et al., 2013; Burns & Kakara, 2018; Lohman et al., 2019; Orces, 2008). Additionally, falls risk profiles differ significantly between men and women (Chang & Do, 2014; Ek et al., 2019; El Fakiri, 2015; Yi et al., 2021), especially in that men who fall tend to have more comorbidities than women (Gale et al., 2018; Vu et al., 2011).
The current literature is mixed regarding the associations between race/ethnicity and falls among older adults. A systematic review and meta-analysis identified that Hispanic and non-Hispanic Black older adults reported fewer falls within a 12-month period (Wehner-Hewson, et al., 2021). Nicklett and Taylor (2014) identified no significant differences in falls prevalence between non-Hispanic White, African American, and Hispanic older adults; however, when examined longitudinally, African Americans had lower odds of experiencing a fall and fewer recurrent falls. Findings that Black older adults had lower odds of experiencing an incident and recurrent falls and fractures, relative to non-Hispanic Whites, were confirmed by other studies conducted in the United States (Sun et al., 2016) and Canada (Morin et al., 2022). In yet another study, the odds of falling among those with two or more chronic conditions did not differ between non-Hispanic White, African American, and Hispanic older adults (Kwon et al., 2018). As reported here, studies about falls prevalence and fall-related risk factors among older adults are available, but few studies examine risk factors associated with incident and recurrent falls, especially with specific attention to men and differences by race and ethnicity (Alamgir et al., 2012; Han et al., 2014; Murphy et al., 2014; Wendelboe & Landen, 2011).
To address this gap in the literature, the current study utilized a large sample of male participants with chronic conditions to advance the literature regarding incident and recurrent falls among men of different races and ethnicities. To investigate the extent of the problem and examine race- and ethnicity-based differences between non-Hispanic White (NHW), non-Hispanic Black (NHB), and Hispanic men, the primary aim of this study was to identify the prevalence of incident and recurrent falls within a national sample of men ages 60 and older, with at least one chronic condition, who enrolled in an evidence-based fall prevention program. The secondary aim of this study was to identify the risk factors associated with incident and recurrent falls among these men.
Methods
Study Participants and Procedures
The database used in this study was exported from a national repository of participants who enrolled in evidence-based fall prevention programming in the United States from August 2014 to February 2019. All grantees funded by the Administration for Community Living (ACL) to deliver fall prevention programs were required to enter workshop and participant data as well as information about workshop attendance and delivery sites. Additionally, grantees were required to collect and enter data at or before the first workshop session regarding participants’ sociodemographics, fall history, fear of falling, and other fall-related risk factors. This study utilized these baseline participant data to meet study aims. The intention of this paper was not to assess the effectiveness of any fall prevention program for which the participants enrolled. Grantees utilized different strategies to recruit participants and promote workshops including (but not limited to) in-person interactions, flyers, social media, word-of-mouth, and referrals from partnering clinical and community organizations. Institutional Review Board approval was granted from The University of Georgia (#00000249) for this non-human subject research of secondary, de-identified data.
Measures
Dependent Variables
The dependent variables were based on the number of times participants self-reported a fall in the previous three months. Participants were asked, “In the past three months, how many times have you fallen?” A fall was defined as unintentionally changing position to rest on the ground, floor, or any lower level. Responses were collected continuously but initially grouped into three distinct categories: 0 falls (i.e., non-faller); 1 fall (i.e., incident faller); and two or more falls (i.e., recurrent faller). This trichotomous dependent variable was used to assess characteristics of incident and recurrent fallers relative to those who did not fall in the past three months. Subsequently, to examine differences between incident and recurrent fallers, participants who reported 0 falls were omitted from analyses to create a dichotomized variable to directly compare incident and recurrent fallers (i.e., one fall vs. two or more falls).
Independent Variables
The primary independent variable of interest was race/ethnicity, which was a three-category variable (i.e., non-Hispanic White, non-Hispanic Black, and Hispanic). Additional sociodemographic variables were included to account for variance in the dependent variable. Age was collected as a continuous variable in years but collapsed into a four-category variable for analyses (i.e., 60–69, 70–79, 80–89, and 90+). Educational status was assessed on a scale ranging from “less than high school” to “college graduate or higher,” which was collapsed to create a 3-category variable (i.e., less than high school, high school/GED/vocational training, and college graduate or higher). Participants were also asked if they lived alone (i.e., yes or no). Using the ZIP code of the delivery location for the workshop, the ZIP Code Tabulation Area (ZCTA) was obtained and used to determine the median household income (2011-inflation-adjusted dollars), as a proxy indicator of affluence according to geographic location (Smith et al., 2018).
To better understand participants’ health status, they were asked to report if a healthcare provider ever told them that they had any of seven chronic conditions (i.e., arthritis/rheumatic disease, heart disease or blood circulation problem, diabetes, depression, cancer, breathing/lung disease, and glaucoma). Participants self-reported their conditions on a “check all that apply” list, and the number of endorsed conditions was summed to create a count variable, which was used continuously in analyses (ranging from 0 to 7). Participants were asked to rate their general health status on a 5-point Likert-type scale that ranged from “poor” (scored 1) to “excellent” (scored 5) (CDC, 2018), which was treated continuously in analyses.
Two fall-related risk factors were included in analyses based on their relevance to incident and recurrent falling. Participants were asked to rate their fear of falling using a 4-point Likert-type scale ranging from “not at all” (scored 1) to “a lot” (scored 4), which was treated continuously in analyses. They were also asked “During the last four weeks, to what extent has your concern about falling interfered with your normal social activities with family, friends, neighbors or groups?” Responses ranged from “not at all” (scored 1) to “extremely” (scored 5) and were treated continuously in analyses.
Statistical Analyses
All analyses were performed using SPSS version 28. Descriptive statistics were calculated for all variables of interest. Bivariate analyses were performed to compare sample characteristics by the three race/ethnicity categories of participants (i.e., NHW, NHB, and Hispanic). Pearson’s chi-square tests were used to assess the proportional differences across race/ethnicity for categorical variables. One-way Analysis of Variance (ANOVA) was used to assess mean differences for continuous variables. Bivariate analyses were also performed to estimate the prevalence of falls and recurrent falls among study participants and compare sample characteristics across three categories of fall status (no falls, one fall, and two or more falls). Pearson’s chi-square tests were used to assess the proportional differences across fall status categories for categorical variables. One-way ANOVA was used to assess mean differences for continuous variables. Statistical significance for this study was set a p < .05. Only variables with statistically significant bivariate associations with falls status were included in multivariable regression models.
A multinomial logistic regression model was fitted to identify factors associated with incident and recurrent falling relative to men who did not report a fall. Men who reported no falls in the past three months served as the referent category. Using the variance inflation factor, multicollinearity was assessed between the independent variables (Lee, 2021). The results of the multinomial regression model are presented as adjusted odds ratios, alongside their respective 95% confidence intervals (CIs) and p-values. Then, the same independent variables used in the multinomial logistic regression were included in a binomial logistic regression to assess factors associated with recurrent falls among men who had fallen. Men who reported no falls in the past three months were excluded from this model, and incident fallers (i.e., one fall in the past three months) served as the referent category. The results of the binary logistic regression model are presented as adjusted odds ratio, 95% CI, and p-values.
Results
Sample Characteristics
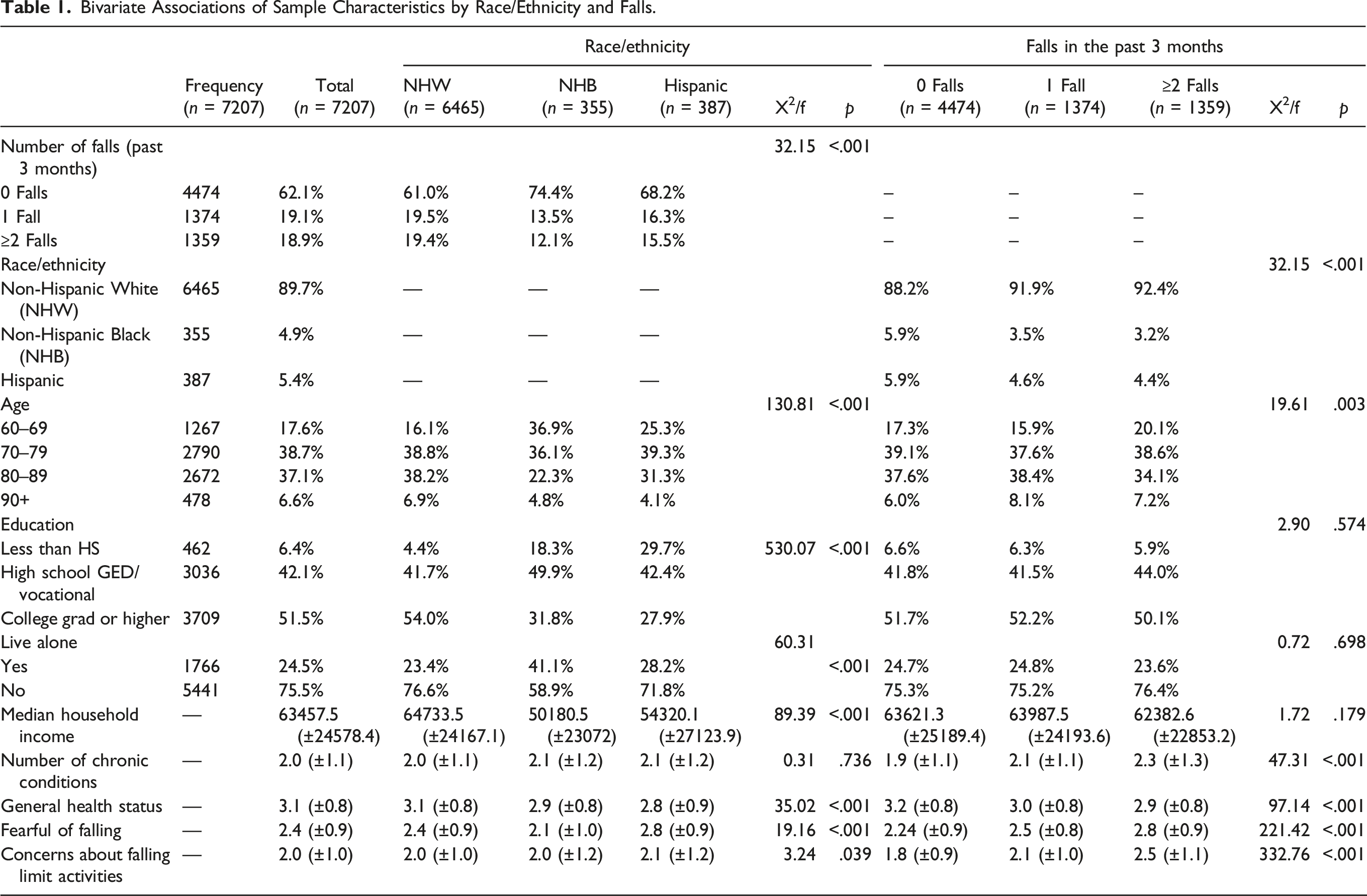
Bivariate Associations of Sample Characteristics by Race/Ethnicity and Falls.
Sample Characteristics by Race/Ethnicity
When comparing sample characteristics by race/ethnicity, a significantly larger proportion of NHW reported incident and recurring falls in the past three months (χ2 = 32.15, p < .001) relative to NHB and Hispanic participants. A larger proportion of NHW were in the older age groups relative to NHB and Hispanic participants (χ2 =
On average, NHW men enrolled in programs delivered in areas with higher median household incomes (f = 89.39, p < .001). On average, NHW participants reported significantly higher general health status (3.1 ± 0.8) than NHB (2.9 ± 0.8) and Hispanic (2.8 ± 0.9) participants, respectively (f = 35.02, p < .001). On average, Hispanic men reported higher fear of falling levels (f = 19.16, p < .001) and more activity limitations because of their concerns about falling (f = 3.24, p = .039) relative to their NHW and NHB counterparts, respectively.
Sample Characteristics by Fall Status
When comparing sample characteristics by fall status, a significantly larger proportion of men in the 70 to 79 age groups reported recurrent falls (i.e., 2 or more falls; χ2 = 32.15, p < .001). On average, men reporting recurrent falls reported significantly more chronic conditions (f = 47.31, p < .001), worse general health status (f = 97.14, p < .001), higher fear of falling (f = 221.42, p < .001), and more activity limitations because of their concerns about falling (f = 332.76, p < .001) relative to those reporting no falls or an incident fall only, respectively.
Factors Associated With Incident and Recurrent Falls Relative to No Falls
Factors Associated With Incident and Recurrent Falls.
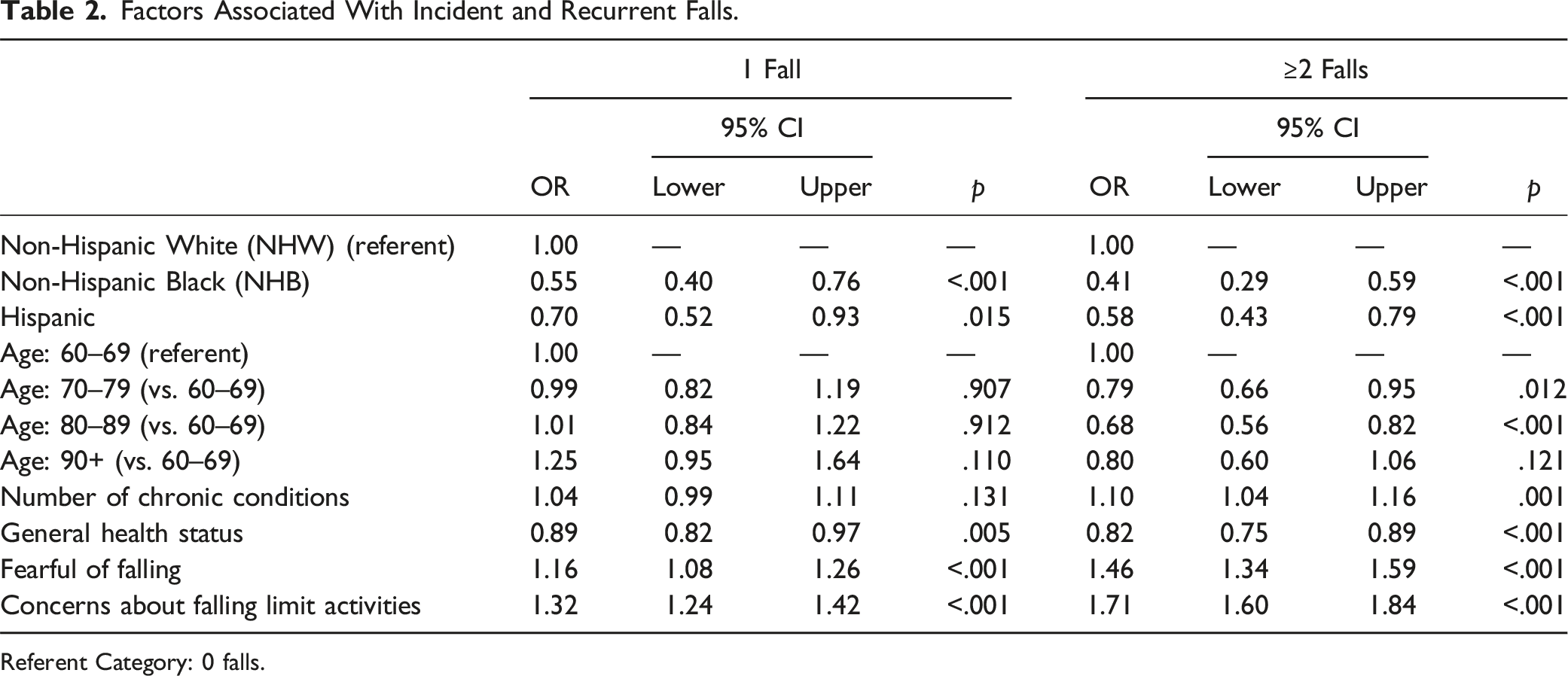
Referent Category: 0 falls.
Regarding recurrent falls, compared to NHW men, NHB (OR 0.41, 95% CI 0.29–0.59) and Hispanic (OR 0.58, 95% CI 0.43–0.79) men were significantly less likely to report recurrent falls. Relative to men ages 60–69 years, those in age groups 70 to 79 (OR 0.79, 95% CI 0.66–0.95) and 80–89 (OR 0.68, 95% CI 0.56–0.82) were less likely to report recurrent falls. Each additional chronic condition reported increased the likelihood of recurrent falls (OR 1.10, 95% CI 1.04–1.16). Men who perceived themselves to have better general health status were less likely to report recurrent falls (OR 0.82, 95% CI 0.75–0.89). Conversely, men who were more fearful of falling (OR 1.46, 95% CI 1.34–1.59) and reported more activity limitations because of concerns about falls (OR 1.71, 95% CI 1.60–1.84) were more likely to report recurrent falls.
Factors Associated With Recurrent Falls Relative to Incident Falls
Factors Associated With Recurrent Falls Relative to Incident Falls.
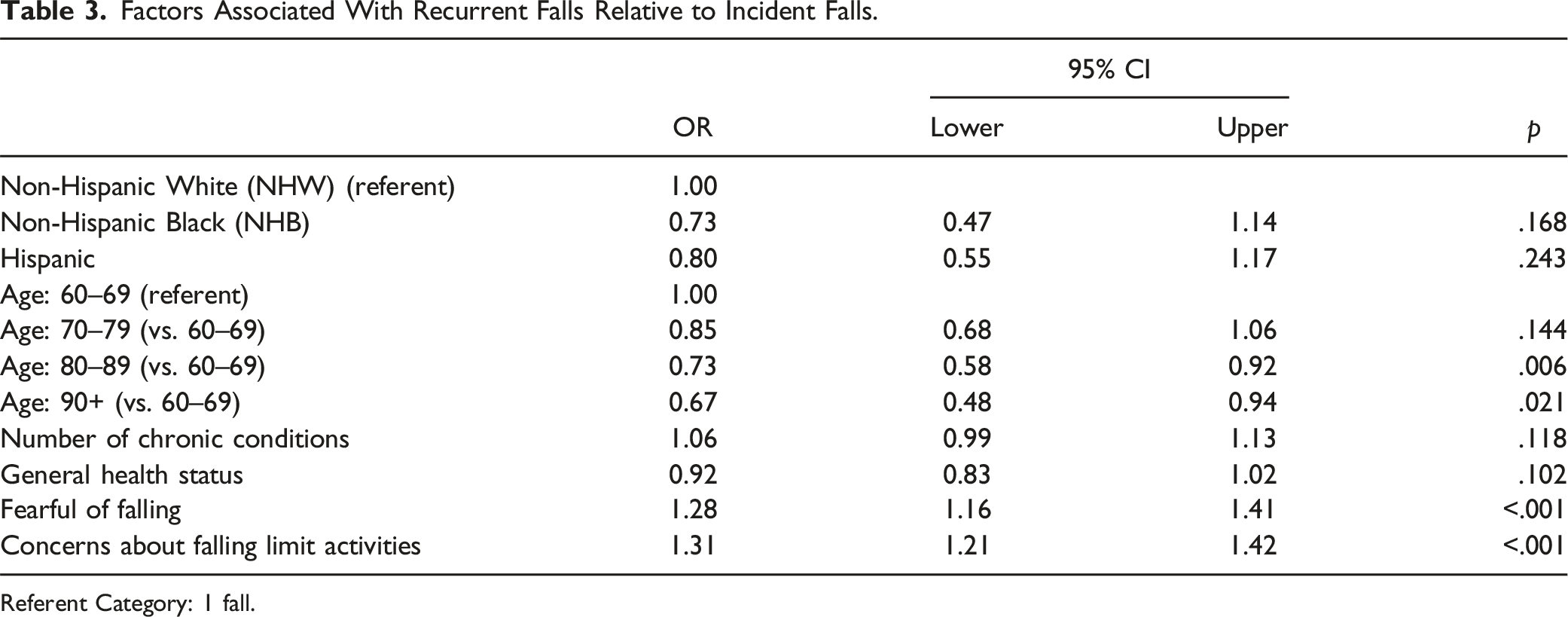
Referent Category: 1 fall.
Discussion
This study identified factors associated with incident and recurrent falls among older NHW, NHB, and Hispanic men with chronic conditions. With a mean age of 77.8 (±8.0) years, the proportion of men who reported at least one fall was approximately 38% (19.1% for incident fallers and 18.9% for recurrent fallers). This is much higher than the proportion of men who reported at least one fall in some previous studies; a study conducted in Canada reported a prevalence of 17.3% among men (Chang & Do, 2015), a Turkish study using four objective testing measures for falls, reported a 25.4% prevalence (Dokuzlar et al., 2020), and among community-dwelling men in the US, one study observed a 25% rate of reporting falls (Munch et al., 2015), while another showed a 26.5% prevalence among men (Paliwal et al., 2017).
The samples in many of these earlier studies had lower average ages than the current study and participants reported falls after 12 months (Chang & Do, 2015; Munch et al., 2015; Paliwal et al., 2017), as opposed to the current study’s past three months reporting period. In a prospective study in Australia focusing only on older men, with similar average age (77.3 years) but fall reporting during a mean follow-up period of 42.6 ± 8.7 months, recorded higher rates of fall reporting among men (47%) (Khalatbari-Soltani et al., 2021). The shorter reporting period in this study may have reduced fall underreporting related to recall bias, compared to other studies that relied on longer recall periods for reporting (Fujimoto et al., 2000; Karlsson et al., 2014). Higher reported falls rates may reflect the prevalence of multimorbidity among participants, thus potentially indicating higher fall-related risk within this sample relative to men in other studies. However, the most probable explanation for the higher rate of self-reported falls is that the men in the current study actively enrolled in a fall prevention program, which suggests that they recently experienced a fall or were more fearful of falling than other men not electing to enroll in such a program (i.e., possible self-selection bias).
When compared to their NHW counterparts, more predominant risk factors associated with falls were reported among NHB (e.g., lower education, lower median household income, living alone, and worse perceived health) and Hispanic (e.g., lower education, lower median household income, worse perceived health, more fear of falling, and restricting activities because of fall-related concerns) men, respectively. However, NHB and Hispanic men reported significantly fewer incident and recurrent falls than NHW men. This contradicts the findings of an international study, in which falls among US older adult males were compared across racial/ethnic groups, but there were no significant differences (Karlsson et al., 2014). In this current study’s sample, NHW men were generally older than NHB and Hispanic men and have longer life expectancies generally (Bond & Herman, 2016; Sun et al., 2016) which may explain the widened fall-related disparities between older men based on race/ethnicity. However, despite differences in prevalence, some authors found that fall-related mortality does not differ by race/ethnicity among older adult men and women combined (Nicklett & Taylor, 2014).
This study adds to the current literature by highlighting the fact that race/ethnicity may be a significant predictor of recurrent falls within the previous three months among older men. These findings support those from previous studies about race/ethnicity-based differences in fall prevalence (Nicklett & Taylor, 2014; Wehner-Hewson et al., 2021). The current study findings also contradict findings from earlier studies identifying no such differences (Karlsson et al., 2014; Kwon et al., 2018); however, these studies were not specific to older men living with chronic conditions.
Although cultural considerations suggest that older adults of color tend to live with caregiving relatives, which is sometimes supported by data (Okoye et al., 2021), the NHB men in the current study were significantly more likely to live alone, than NHW and Hispanic men (Verdery & Margolis, 2017). However, this is somewhat contradictory to another study reporting that both NHW and NHB men are equally likely to live alone (Sun et al., 2016). It appears that although living alone may independently increase the risk of falls among older adults (Ek et al., 2019; Zeytinoglu et al., 2021), the characteristics of the homes and neighborhoods in which older adults live are equally strong factors when considering living situations, and the homes of older adults who report recurrent falls tend to be characterized by disorderliness and disrepair (Okoye et al., 2021).
On average, participants reported having 2.0 (±1.1) chronic conditions, and the current study’s findings suggest that higher comorbidities were associated with incident and recurrent falls. For incident falls, contrary to what this current study found, one study showed that this relationship is either more pronounced or observed only in women (Chang & Do, 2015), while another study found that the dose–response relationship exists in older adults regardless of gender (Immonen et al., 2020). In a study conducted among community-dwelling older adults who had been previously hospitalized for a fall-related injury, comorbidity and higher multiples of comorbid conditions were found to be overwhelmingly higher among men than in women (Vu et al., 2011).
Comorbid diseases tend to have serious effects among older adults, especially for men of advanced ages (Ek et al., 2019), because they increase the recurrence of falls (Kwon et al., 2018; Okoye et al., 2021) and cause significant morbidity and disability among already severely sarcopenic men (Burns & Kakara, 2018; Yang et al., 2016). Sarcopenia, in and of itself, is a strong predictor of falls (Bischoff-Ferrari et al., 2015; Cruz-Jentoft et al., 2019; Schaap et al., 2018). Comorbidities can also directly cause sarcopenia by activating chronic inflammation, decreasing activity, and causing impairments in metabolism (Watson, 2012). The current study adds to the literature because it specifically identifies that having more comorbidities was associated with recurrent falls among older men with chronic conditions.
When looking at the full sample, participants perceived general health status, fear of falling, and activity limitations because of fall-related concerns were associated with incident or recurrent falls. More specifically, compared to men who did not fall, men reporting incident and recurrent falls reported worse health status, more fear of falling, and more activity limitations because of fall-related concerns. From this study, being fearful and being concerned about falling increased the likelihood of reporting a fall, and these two increased the risk of reporting recurrent falls. This is consistent with the findings of an earlier study, which compared the risk of falls from fear of falling across multiple racial/ethnic groups; NHW adults reported more fear of falling than NHB, which they suggested could explain the lower incidence of falls among NHB adults (Singh et al., 2020).
Individuals who have experienced a fall may develop fear of falling, which eventually modifies behavior toward further adopting sedentary lifestyle (Pellicer-García et al., 2020). Hence, as these older adults become frailer, they tend to become less active (Liu et al., 2021), likely for fear of suffering an injurious or fatal fall. As fear of falling and/or concern about falling reduce motivation or self-efficacy to adopt recommended health practices, or act as potential barriers to socializing or engaging in physical activity programs (Okoye et al., 2022), older adults continue to avoid physical activities, and a vicious cycle of disuse atrophy and sarcopenia of the lower limb muscles occurs, which, in an individual with multiple comorbid conditions, worsens the risk of more falls or recurrent falls (Jiang et al., 2022).
While fear of falling is more likely associated with females (Birhanie et al., 2021; Liu et al., 2021; Singh et al., 2020), a study among older adults with activity of daily living (ADL) impairments showed that fear of falling was more strongly associated with recurrent falls among men than women (O & El Fakiri, 2015). Thus, further investigation into the effects of fear of falling among men, especially older men of color, will contribute to our understanding of the gender-specific associations between fear of falling and falls.
An interesting finding from this study is that contrary to the previous literature, older men were less likely than younger men to report incident and recurrent falls, respectively. There are a few possible interpretations of these unique findings. Because these male participants self-selected to enroll in an evidence-based fall prevention program, it is possible that they may have experienced a recent fall, had more severe fall-related consequences, and/or been encouraged to enroll by a healthcare professional or family member. Having higher risk or more adverse events may be especially relevant for the younger men ages 60–69 years, who are well below the mean age for evidence-based fall prevention programs (Smith et al., 2018).
Another possibility is the presence of survivor bias, which suggests that the older men in this study, despite their age, were less at-risk for falls relative to their younger counterparts because of their lifestyle, living situation, and/or chronic disease status. For example, it may be that the older men in this study were not working or less mobile in the community, which may have been a protective factor in this study, despite sedentary behavior and immobility being known risk factors for falls (Bergen et al., 2019; Deandrea et al., 2010). More research is needed to better understand the relationship between age and falling among men enrolling in fall prevention programming.
Although the current study analyzed data from older men with chronic conditions who enrolled in evidence-based fall prevention programs (Smith et al., 2018), it did not evaluate the effectiveness of these programs to reduce falls or fall-related risk factors. Such evidence-based programs have demonstrated efficacy to reduce fear of falling (Yoshikawa et al., 2020), improve physical activity (Fernández-Argüelles et al., 2015; Sherrington et al., 2017), increase confidence to prevent and manage a fall (Arnold et al., 2011), and prevent falls (Guirguis-Blake et al., 2018). Aspects of effective multi-factorial fall prevention programming that reduce falls can include cognitive reframing (i.e., to reinforce that falling is preventable), lower limb exercises (i.e., to improve strength, balance, and flexibility), medication reconciliation (i.e., to reduce polypharmacy complications among those with multimorbidity), and home environment modification (e.g., grab bars, reduce clutter, and improve lighting) (Guirguis-Blake et al., 2018; Healy et al., 2008; Shubert et al., 2018; Stevens & Phelan, 2013; Szanton et al., 2016).
Additionally, findings from the current study suggest that efforts prioritizing chronic disease management among older adult males can potentially prevent incident and/or recurrent falls (Immonen et al., 2020; Paliwal et al., 2017) or reduce adverse ramifications occurring from a fall, if they occur (Ek et al., 2019). Chronic Disease Self-Management Education (CDSME) programs are widely available and effective interventions in the United States (Smith et al., 2017). CDSME programs have been shown to help individuals living with chronic conditions and multimorbidity improve healthy behaviors and prevent hospitalizations and emergency room visits (Lorig et al., 1999; Ory et al., 2013a, 2013b). These interventions focus on practical disease management strategies such as physical activity, nutrition, sleep, medication adherence, social support, and communication with healthcare providers. Given each of these disease self-management strategies addresses known risk and protective factors for falls (Smith & Ory, 2023), participation in disease self-management interventions may have direct and indirect benefits on fall prevention among older men. Although there were no differences in the number of chronic conditions by race/ethnicity in the current study, and since older adults of color tend to report more comorbidities and physical impairments (Kwon et al., 2018; Nicklett & Taylor, 2014; Sun et al., 2016), these contradictory findings with the literature warrant further investigation to assess the effects of chronic diseases on falls among older males of color. Additionally, studies are needed to determine if CDSME programs can serve as complementary strategies to effectively reduce falls risk among older males of color.
Strengths and Limitations
This study was not without limitations. First, it relied on self-reported data, which may have introduced recall bias and inaccurate reporting. Many falls among community-dwelling older adults are not witnessed by others, or not severe enough to cause injuries or require medical care, they often go unreported (Hoffman et al., 2018). Although older adults may be more likely to recall falls that result in injury or hospitalizations, the impacts of recall bias on the internal validity of measures such as non-injurious falls were minimized by the relatively short passage of time in the current study (i.e., past three months).
Second, the sample may have been biased because all participants in the dataset were enrolled to participate in an evidence-based fall prevention program. As such, this means that these men may not have been representative of the larger male population because they voluntarily elected to participate in a fall-related intervention. For example, relative to the average older adult male, it is possible that the men in this sample were more likely to have experienced a fall or been more fearful of falling. In addition, the proportions in this sample are not completely reflective of the racial proportions in the United States (United States Census Bureau, 2022), suggesting that the findings of this study may not be generalizable to the larger, national male population. This study had a substantially larger proportion of NHW than NHB and Hispanic men; hence, additional studies are needed that purposively examine incident and recurrent falls, and related risk factors, among older NHB and Hispanic men.
Third, because these data were used cross-sectionally (i.e., only using baseline measures), this study could not determine causality between reported falls and specific risk factors. However, this study provides direction for other studies that seek to investigate causality and the underlying mechanisms between some of these risk factors and falls.
Fourth, while this study had a large sample size and allowed for the control of a sufficient number of confounders in this ethnically diverse national sample, assessing gender-specific risk factors, the variables available in the baseline data were limited. There may have been many important factors contributing to incident and recurrent falls that were not measured in this dataset (e.g., social supports like marital status, household composition, household income, barriers to disease self-management, and details about disease history and treatment).
Conclusion
This descriptive study highlights the prevalence of risk factors for incident and recurring falls among older men with chronic conditions. Findings suggest that NHW men report more incident and recurrent falls, despite NHB and Hispanic men having more risk factors at younger ages. This study reinforces that known risk factors are associated with recurrent falls (i.e., older age, more comorbidities, worse general health, fear of falling, and limited activity because of fall concerns), but these findings are specific to a sample of older men with one or more chronic conditions. These findings may guide future research to identify risk for and prevent incident and recurrent falls among older men. Further, this study may help contextualize the men enrolling in fall prevention programming in their communities. Efforts to improve chronic disease management among these men may be particularly useful to alleviate physical and psychosocial issues brought about by their conditions, which in turn can reduce risk related to incident or recurrent falls.
Footnotes
Acknowledgments
The Administration for Community Living/Administration on Aging (ACL/AoA) is the primary funding source for this national study. The findings, conclusions, and opinions expressed do not necessarily represent official Administration for Community Living/Administration on Aging policy. The National Council on Aging (NCOA) served as the Technical Assistance Resource Center for this initiative and collected data on program participation from grantees.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National CDSME Resource Center - 90CSSG0048 and National Falls Prevention Resource Center - 90FPSG0051.
IRB Protocol Approval
Institutional Review Board approval was granted from The University of Georgia (#00000249) for this non-human subject research of secondary, de-identified data.