
Abstract
The purpose of this study was to explore the perceptions of disability among Saudi mothers and to understand the implication of the meaning for the mothers of children with disability. A critical ethnographic approach was employed using focus groups and follow-up interviews with the mothers. Three primary themes were identified that specifically influenced and affected the mothers’ experiences: (a) culture and religion, (b) motherhood and disability, and (c) community stigma and discrimination. The study reveals much-needed knowledge and sheds light on a topic, the details of which are rarely available in research literature from the Middle East. The findings further endorse the need for clinicians to listen to the mothers to consider their beliefs and the impact of these beliefs on their experiences. This, in turn, may provide a valuable conceptual lens for health care practitioners to use the family-centered model when working with cerebral palsy children.
Introduction
Cerebral palsy (CP) is the most common physical disability in childhood, the incidence of CP has been estimated to be 2 to 2.5 per 1,000 live births (Reddihough & Collins, 2003). In Saudi Arabia, however, agreement on incidence and prevalence levels has yet to be established, although a study conducted by Al Salloum, El Mouzan, Al Omar, Al Herbish, and Qurashi (2011) suggested that CP is the most common neurological disorder among Saudi children with a prevalence rate of 2.34 per 1,000. The complex and chronic nature of the multiple impairments that contribute to the diagnosis of CP has a substantial impact on the functional level and quality of life of the child, which, in turn, can result in a significant physical, financial, and psychological health burden on the family (Rosenbaum, 2003).
Recognizing the critical role that family plays in the integration and provision of care for children living with complex disabilities such as CP has resulted in shifting from focusing on the child to considering the needs of the whole family (Rosenbaum, King, Law, King, & Evans, 1998). Therefore, family-centered care has become a cornerstone of rehabilitation services (King, Teplicky, King, & Rosenbaum, 2004). Family-centered practice encompasses collaboration with families on child-related goals as well as the evaluation of family values, beliefs, and needs to design interventions targeted at positive family outcomes (Panzarella, 2009; Rosenbaum et al., 1998; Trute & Hiebert-Murphy, 2007). This means that each family can choose its own, optimal service delivery and should, for example, be given options with respect to their level of involvement (Law et al., 2003). Different families will have different preferences when it comes to their involvement in their child’s care. This may be influenced by culture, and how parents think about their children and different disability diagnoses is likely to have different meanings for parents from different cultural backgrounds (Hanson, Lynch, & Poulsen, 2013). Moreover, the concept of “disability,” and what it means to live with a disability, is multifaceted, including social and cultural influences, traditional practices, and personal experiences (Barnes, 2003; Bickenbach, 2009; Brown, 1997, 2002).
In the literature, numerous disability models are used to explore the disabilities from sociological, political, and medical perspectives. The term has been defined from sociological, political, and medical perspectives, and these varied descriptions have had an impact on disabled social support (Thomas, 2004). The social model of disability offers a paradigm for understanding disability by identifying the causes of disability within social and political domains (Smith, 2009). The social model of disability is important in understanding conceptions of and prejudices against people with disabilities and their carers by society (Barnes & Mercer, 2010; Shakespeare, 2006). The social model has been applied in this study to provide a framework for understanding how society perceives children with disabilities and their carers, and how mothers perceive themselves and their disabled children.
Mother’s Perception of Disability
Parents’ perceptions about the nature of their children’s disabilities have been a focal point among different cultural groups, including Mexican Americans, Chinese Americans, Africans, Turks, Iranians, Arabs, and Asians (Danseco, 1997; Daudji et al., 2011; Diken, 2006a; García, Pérez, & Ortiz, 2000; Kermanshahi et al., 2008; Masasa, Irwin-Carruthers, & Faure, 2005; Ryan & Smith, 1989). These studies have found that in every culture, disability is perceived differently. Moreover, these perceptions shaped parental attitudes toward their children with disabilities; the resources parents are willing to invest in the treatment, training, and education of these children; and parental expectations for the future of their children with disabilities. Parents from some cultural backgrounds have been found to hold dual biomedical and traditional beliefs regarding the nature, causation, and treatment of disability (Daudji et al., 2011; Diken, 2006b; Raman et al., 2010). Similarly, many mothers may not perceive biomedical interventions as effective or even necessary, or may not perceive their child as “disabled” (Diken, 2006b). Other mothers, especially those who believe in reincarnation, perceive their child’s condition as temporary (Danseco, 1997). Accordingly, these mothers may be less likely to seek treatment for their children (Danseco, 1997). Indeed, cultural understandings of disability are crucial. Groce (1999) argues that people with disabilities are limited not so much by impairments or activity limitations, but more by the cultural interpretations of disability. Therefore, understanding the cultural context and what is normative within a particular cultural group is essential to the practice, with different diagnoses of disability likely to have different meanings to parents from different cultural backgrounds (Santos & Mccollum, 2007).
Saudi Arabia is an Arab Islamic State, and Islam is the primary and state religion. The culture in Saudi Arabia is embedded in Islam; however, economic status, level of education, and environmental factors are also responsible for shaping the culture (Al-Shahri, 2002; Buckman, 2011). The traditional Saudi family is based on an extended family unit, which consists of the husband, wife, their children, and their married children with their spouses and grandchildren (Al-Saif, 1991). Family members in Saudi Arabia expect great loyalty from each other and accept familial obligations because this provides them with harmony and personal identity (Al-Saif, 1991). Therefore, a disabled person is cared for by his or her family, rather than by an institution. However, many family members do not have the knowledge or expertise to provide adequate or appropriate care to the disabled person, although this kind of responsibility is part of Islamic law and tradition. Saudi society has often marginalized disabled people for various reasons, including lack of awareness about disabilities in communities and shame associated with having a disability. Disabilities were thought to be hereditary, even if they were acquired during adulthood (Al-Jadid, 2014). The term “disability” is avoided by official associations as a protective strategy for the person and/or family. Instead, the term “people with special needs” is used. Furthermore, disabled girls were long hidden away in homes as they could be a reason for their sisters remaining unmarried, as people would avoid approaching the family (Al-Jadid, 2013).
Understanding cultural concepts and beliefs about disability in the Saudi cultural context is fundamental to assisting in planning and delivering family-centered rehabilitation services for children. However, little is known about the perceptions of disability in Middle Eastern countries, specifically the experiences of Saudi mothers with disabled children, nor is there much research on mothers’ experiences when that disability is CP. As mothers are the primary care providers often occupying traditional gender roles in Saudi Arabia, an understanding of mothers’ perceptions and beliefs about their children’s disabilities and what influences these beliefs is crucial. Developing an understanding of the impact of disability on mothers and the exposure to different values, influences, and mediating factors have not been explored. This study endeavors to bridge this gap by exploring the perceptions and experiences of mothers who have children with CP within the Saudi cultural context.
Method
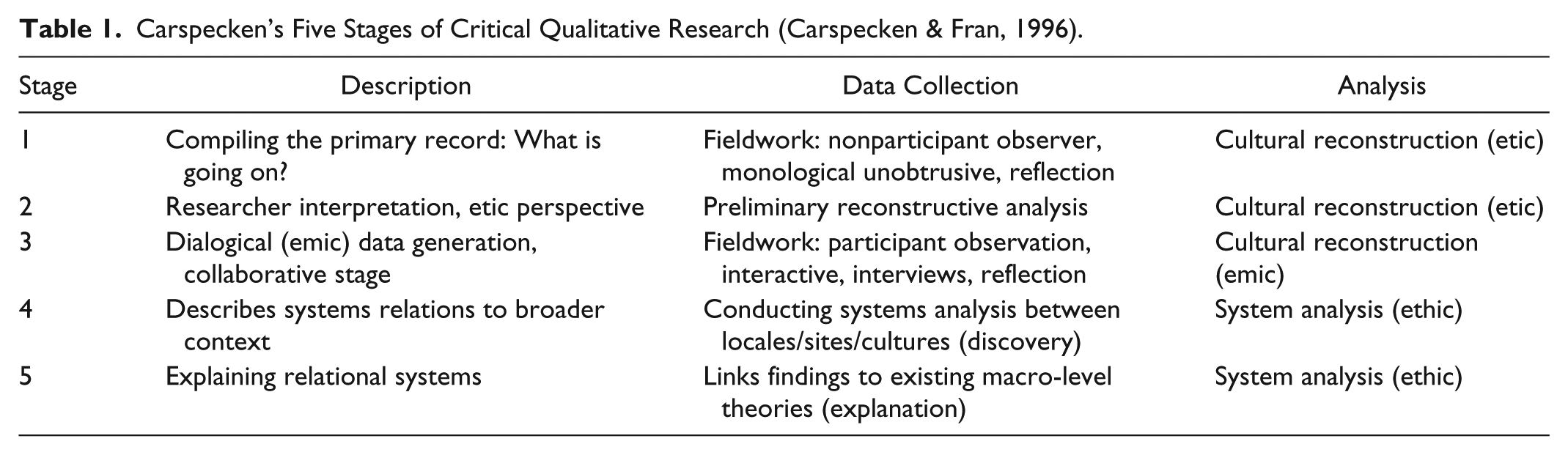
The aim of this study is to capture the experiences of the mothers conveyed in their own words and to use their viewpoints as the basis for discussion and analysis. J. Green and Thorogood (2014) suggest that when the researcher seeks in-depth understandings, qualitative methods are essential tools for exploring subjective accounts of peoples’ emotions, perceptions, and actions. A critical ethnographic approach proposed by Carspecken and Fran (1996) was employed here as this provides a detailed and critical exploration of the cultural aspects of the disability based on the knowledge of mothers and their interpretation of their perception and experiences. This framework comprises five stages (Table 1). The first three stages of Carspecken’s framework use critical analytical models to reconstruct cultural structures and themes, whereas the last two stages are designed to describe systemic relationships and articulate the findings in relation to broader sociocultural factors or existing theories (Carspecken & Fran, 1996).
Carspecken’s Five Stages of Critical Qualitative Research (Carspecken & Fran, 1996).
Study Setting
The study was conducted at the King Fahad Medical City (KFMC), which is located in the center of Riyadh, the capital city of Saudi Arabia, and is considered to be the largest and most advanced medical complex in the country, with a total capacity of 1,095 beds. KFMC comprises the following four hospitals and five centers: the Main Hospital, the Children’s Hospital, the Rehabilitation Hospital, the Women’s Specialist Hospital, the Neuroscience Centre, the Diabetic Centre, the Prince Salman Heart Centre, and the Prince Sultan Hematology and Oncology Centre.
The Rehabilitation Hospital, which is accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF), has 85 beds and offers inpatient care, day care, and outpatient services. The hospital receives patients who are referred from other KFMC hospitals and centers, as well as from district hospitals all over the country. Its physical therapy department provides both inpatient and outpatient services for adults and children. Pediatric physical therapy services are provided for children below 13 years of age; according to physical therapy records, more than 30 children with CP are seen daily in the pediatric physical therapy clinic.
Participants
Participants were recruited using convenience sampling. Mothers whose children had a diagnosis of CP and were registered at the KFMC for physical therapy were invited to participate in the study. Recruitment was undertaken using posters within the department. Six mothers self-selected themselves into the study. Specific demographic information is shown in Table 2.
The Study Questions and Issues.

Note. CP = cerebral palsy.
Data Collection
Data collection methods included participant observation, field notes, focus group, and semi-structured follow-up interviews. Prior to entering the field, researchers developed two lists of questions. The first list identified issues that can be investigated, whereas the second list outlines information required to address the questions as issues arise. The list of the questions and issues is presented in Table 3.
Profile of Mothers and Their Children With CP.

Note. CP = cerebral palsy.
This research is informed by the main researcher’s work experience as a pediatric physiotherapist, which gave the researcher the opportunity to observe the mothers’ reactions to the medical term CP during both clinic visits and interviews and focus group. Prior to the main data collection, a primary record was developed. Carspecken and Fran (1996) explained a primary record built up through note-taking, audio recordings, and if desired, videotaping. Observations and field notes were handwritten and then transcribed into a Word document. Two focus groups were conducted with six mothers. The focus group discussions were undertaken in Arabic and took place in the physical therapy department conference room that was suitable to ensure the confidentiality of the discussions. Sessions lasted between 60 and 90 minutes and were all audio-taped, with the participants’ agreement. Three follow-up interviews were conducted after the preliminary analysis of the data from the two focus group sessions. Three mothers were interviewed individually to highlight key aspects of their perceptions of CP and to explore specific areas that had been highlighted as significant during the focus group discussions. All follow-up interviews lasted from 30 to 60 minutes. The tone and body language were considered during focus group sessions and interviews. All the interviews were tape-recorded after securing participants’ consent. The researcher kept memos after each interview to record personal impressions related to the interview and to capture contextual information, and these memos were considered during the analysis.
Data Analysis
Focus groups and interviews were conducted and transcribed into Arabic and subsequently translated into English using the back-translated method to ensure accuracy in the meaning of the original language. The data were initially entered into a computerized database, coded, and categorized to identify the emerging patterns and themes as recommended by Carspecken and Fran (1996). A list of primary codes was derived, the relationships among the codes were identified, and categories and final assertions were thereby generated. Reflection was used to prevent probable biases. Then, the categories were brought together to generate the main themes and final assertions.
All sources of data, including signed consent forms, demographic information, interview audiotapes, field notes, written transcripts and their translations, and data analysis notes, were stored in a locked cabinet, whereas electronic data were stored in password-protected files accessible only to the researcher. Furthermore, the anonymity of the research participants was maintained by substituting anonymous codes for names, with only the researchers having knowledge of the original names of participants.
Trustworthiness was facilitated by conducting the focus groups and the interviews in an open manner and creating a space for personal reflections. Furthermore, all three of the mothers who participated in the follow-up interviews validated the initial interpretation of the data and confirmed that they accurately reflected their perspectives. Then, the researchers incorporated the data gathered from the follow-up interviews into the categorized themes and examined the analyzed data for linkages to existing literature that best explained the phenomenon.
Ethical Approval and Research Governance
Ethical approval for the study was gained from the University of Brighton’s Faculty of Health and Social Science Research Ethics and Governance Committee (FREGC) and from the institutional review board (IRB) of the KFMC, where the study was conducted.
Findings
In this article, we report on the qualitative findings based on the focus group and follow-up interviews with mothers, which are discussed under three main themes: culture and religion, motherhood and disability, and community stigma and discrimination. This, in turn, reveals rich new insights into mothers’ experiences of their children’s disability. Each theme is discussed separately, bringing in rich descriptions from the mother’s interview quotes (Figure 1).

Diagram showing the three main themes and subthemes, which emerged from the analysis.
Theme 1: Culture and Religion
Religious beliefs and cultural norms were major factors in the mothers’ perceptions of their children’s disability. The mothers native to Saudi Arabia accept all aspects of their life, whether good or bad, happy or tragic, as tests from the God, and how they respond to these tests reflects their faith and eventually their place in the life hereafter.
Subtheme 1: Evil eye and Jinn cause CP
All mothers made references to theologically based explanations to having a child with a disability; they believed that it was “God’s will” that they had given birth to a child with a disability. Some of the mothers explained that it was the role of the evil spirit (Jinn) that gave rise to them having a disabled child. Moreover, although medical specialists diagnosed their children’s condition, they still believed that their children’s disability resulted from someone casting an “evil eye” on them. In Saudi culture, certain beliefs are considered to have a cultural as well as a religious basis, as is evident in the shared belief of the evil eye, whereby an envious person might comment or compliment someone without saying “Masha’Allah” (God protect you from envy). One mother, of a 6-year-old boy, exemplifies this: I believe what happened to my son was a strong ayn (evil eye) that hit his health. I felt it one day when I had a large gathering in my house and one of the ladies without saying Masha’Allah (God protect you from envy), said, “You have a pretty child.” (M6)
Such beliefs about the cause of disability can hinder the management and treatment of a child. In this particular case, another mother refused to follow specific medical advice and became labeled as uncooperative. She did, however, continue with rehabilitation services but also employed a traditional healer who provided an alternative treatment option. She stated, Deep in my heart, I feel it is Jinni that caused my child’s disability. I went for traditional treatment, and they advised me to remove the pump, but his doctor refused to take it out, and I asked him to stop the medication under my responsibility. (M1)
Some mothers felt the need to exploit all treatment possibilities in the hope that they might find a cure for their child. Healing through the Qur’an is established and well known in Muslim culture. Verses of the Qur’an are used by Muslims to protect children from the harmful effects of the “evil eye” and “Jinni” that causes disability. Conversely, mothers also believed that having a disabled child was “fate” or “divine intervention” and that God (Allah) chose them to care for a child with CP. This belief emanated from a core tenet of Muslim faith, namely, that all that occurs in life is mandated by the divine will. They believed that having a child with CP was determined by God and that it could happen to anyone. Equally, they believed and appreciated that health was the greatest blessing from God. Mothers were thankful and recognized the importance of holding on tightly to Islamic principles, which involved suffering, patience, and reward. The repeated use of the expression “Thank God!” by mothers during the focus group interviews reaffirmed their faith in the actions of God. Consequently, this divine religious intervention or fate played an important role in helping mothers to cope, making them calmer and more resilient. One of the mothers with a severely disabled child demonstrated this: “God gave me strength and faith, which helped me handle my child’s disability and for also handling my other child with Down syndrome” (M5). Most mothers believed that God predetermines both the disease and the cure, which may be mediated by prayers, and prayer was constantly invoked as a core support by mothers throughout, regardless of the severity of their children’s disability.
Subtheme 2: Aspiration and optimizing the child’s future
Culturally, mothers’ aspirations for their children’s futures and their improvement indicated hope and a belief that their children might indeed be able to lead a healthy life like ordinary children. They compared their children’s abilities with those of their nondisabled peers and hoped that their children would be able to walk, take care of themselves, and have future occupations. They also expressed their interest in including their children in as many “normal” activities as possible and to integrate them in the society and community. A mother of a 13-year-old boy, for example, wished to see her disabled children have greater independence and greater social inclusion in future: “I want Ab to be independent and able to live like other normal children. I want the society to accept him and I wish that people would stop giving him strange and petty looks” (M1).
The severely disabled children, especially girls, were seen by mothers as frail, needing somebody to look after them even in adulthood, or were seen as vulnerable, finding it more difficult to live alone. Marriage proposals are not offered to individuals with disabilities for this reason; it is just not socially acceptable. In addition, there is also a cultural fear of disabled individuals passing on a genetic defect to their children. The mother of a 14-year-old girl shared her specific anxiety and feelings of worry about the future of her daughter: “It is challenging. I don’t want to think of the future. A lot of issues such as menstrual cycle, I don’t know how she will deal with it. No, I don’t want to think” (M4).
Theme 2: Motherhood and Disability
This theme focuses on how the term CP was perceived by the mothers and influenced their views and impact of the disability on themselves. Although all mothers referred to a religious explanation for the cause of their children’s disability, some also gave medical explanations such as “brain atrophy” and “lack of oxygen.” Such medical terms were more acceptable than the term CP, as one mother stated: “CP means paralysis of the brain. Some children will have problems with hearing, and vision. Others will have difficulty in movement and mobility” (M3).
One mother of twins preferred to believe that they were healthy and had only delayed motor development; she kept hoping they would “catch up to their age.” Furthermore, most of the mothers viewed their children as being healthy and focused on the normal aspects of their children’s development. They were also concerned about their children’s feelings, assuming others would be insensitive to or pity them, so in turn they sought to hide the diagnosis from their children: She asked many times. I always tell her that this is from her birth and that if God is willing, she will improve. I never told her that she has a disability. I also don’t like anyone to tell her about her disability. (M2)
Subtheme 1: Rejection of the term CP
Alternatively, some mothers sought to reject rather than normalize the term and condition, as culturally, the term CP is synonymous with notions of having an “incomplete child” or a child with severe mental retardation and complete paralysis throughout their whole life. One mother justified this by convincing herself that her child was improving. She believed that CP was a progressive disease resulting in deterioration over time; therefore, as her child was improving, he could not possibly have CP: “I know that my child is improving with time; now he has started to talk and express himself, and he had begun to walk too. CP children will not improve over time” (M6).
Rejecting the term CP also resulted in parents delaying seeking medical advice. A mother of a 13-year-old boy realized that her son was unable to move as quickly as the other healthy children. She remained optimistic, however, and hoped for a better future outcome but did not actively seek help from the medical system during that period.
Subtheme 2: The experience of diagnosis and its consequences
Mothers also spoke of their experiences surrounding the diagnosis and identification or labeling of their children’s impairment. Many were distressed by health care providers’ lack of sensitivity, the lack of a specific diagnosis and discussion of the risks attached to the impairment. They expressed their anger and loss of trust in the health care providers for the delay in diagnosis and for not taking their concerns seriously. Mothers spoke of their frustration and disappointment on learning of the initial diagnosis of their child. These feelings of shock, denial, grief, and frustration are evident in the mother of an 11-year-old boy. She had described the diagnosis of CP as being like “the end of the world” because by giving birth to a disabled child, she was unable to live up to social expectations of having a healthy baby. One mother felt that health care providers lacked knowledge of CP, which compromised her daughter receiving optimal medical assessment and diagnosis. The loss of trust and confidence resulted in her seeking a second opinion from outside the country: I took RG to the hospital, and the doctor gave us a paper to physical therapy without any explanation. We asked him what was wrong with her, but he did not answer. Doctors said she was normal. Then, we went abroad, and the doctor diagnosed her as CP. (M4)
Diagnosis and prognosis are vital to managing the impairment and to accessing specialist support services. Thus, the mothers in this study did not have a full picture about the likely prognosis of their children’s impairment. This could affect the mothers’ perceptions of their children’s disability as well as their expectation of their children’s futures. Interestingly, the mother of a 6-year-old boy said that the diagnosis had been given to her as brain atrophy, not CP. The picture was not always pessimistic, however, and some mothers found the attitudes of health services and professionals helpful. The mother of the twins had positive feelings about the health care profession in Saudi Arabia, as she was provided with satisfactory consultation and medical support for accurate diagnosis. She did not experience negative emotions or powerlessness when seeking help, but trusted the health professionals’ knowledge and skills. The standard of care provided enabled her to feel comfortable and confident with the medical system without doubting their competence: “After seeking several hospitals in the south region, we came here (RHD). My children recently were diagnosed with CP. The physician met with us—myself and their father—and explained to us that our sons had mild CP” (M3).
Theme 3: Community Stigma and Discrimination
Each of the mothers spent a great amount of time talking and discussing community attitudes that led to them feeling blamed, shamed, and stigmatized or experiencing overt discrimination and rejection. They all agreed that the most difficult thing was addressing other people’s reactions to their children. They described the social barriers they experienced themselves due to their child’s visible differences. These barriers included stigmatizing attitudes and actions that were directed at mothers during social interactions.
Subtheme 1: Blaming mothers
Mothers were commonly blamed for their children’s disability. One mother, for example, vented her frustration over her mother-in-law’s taunt that she was the cause of her child’s disability and was not a “good” daughter-in-law because she did not have a healthy baby: My mother-in-law blamed me for not having a healthy child. Society blames the mother. In the beginning, my mother and my aunts told me to admit him to disabled centers and to leave him till he became independent, but I refused. (M6)
Mothers also expressed feelings of shame and of receiving negative attitudes from their extended family. One mother of a child with spastic diplegia (wheelchair user) described stigmatizing attitudes and actions from her parents-in-law, who were unwilling to be seen with her child with CP. Such attitudes meant some mothers felt they did not belong and left them feeling hopeless and powerless in family relationships.
Subtheme 2: Stigmatization
Consistent with shame and stigma from the extended family were mothers’ experiences of negative perceptions from the larger society. They reported limited acceptance of their children by society. Here, the public generally excluded them because of a lack of familiarity and knowledge about the child’s disability. Staring and gazing were the most common forms of stigmatization that they experienced, although sometimes oversympathizing also made them feel that their child was not normal. For example, the mother of an 11-year-old boy reported that words such as pity and sympathy were often used to describe the general community’s perception of her child, which was not helpful for feeling and being included. Moreover, the mothers articulated concerns over how stigma could affect their children’s self-esteem and result in psychological damage. This powerlessness or lack of control over public attitudes meant that the mother of a 14-year-old girl felt helpless in protecting her child from others’ attitudes: To tell you the truth, I don’t accept society’s attitude toward my daughter. Their attitude makes my daughter feel bad. At the same time, I can’t control people’s attitudes, and I feel powerless. The word “handicapped” hurts my feelings. It hurts me a lot. (M2)
Reinforcing this level of stigma was the mother of a 14-year-old girl, who believed that disabled children were more openly stigmatized in Saudi Arabia compared with other Middle Eastern countries that she had visited. She felt her daughter was treated as an alien, especially when out at the shopping mall or at the school. “I don’t like Saudis’ attitude toward the disabled. We went to Jordan and Kuwait, but I did not see this attitude, it was only in Saudi Arabia” (M4).
Subtheme 3: Social isolation
Mothers believe that disabled children are an invisible group in society and draw attention and curiosity from other people. This stigma inevitably leads to social exclusion and isolation from society, as well as within their local networks. The mother of a 13-year-old boy stated that she isolated herself and stopped going outside because of the public attitudes: I stopped taking my children out to the shopping mall. Before I used to take them out, but I stopped because of people’s attitudes toward AD. I found it very difficult . . . Very difficult. I don’t know why they behave like this. (M1)
Many mothers purposely avoid social gatherings, preferring to remain at home, where they or their children were less likely to face discrimination. Furthermore, mothers believed inaccessibility, in both environmental and structural terms, was a key issue creating isolation and segregation, as described by this mother: “I have difficulty going for outings, such as going shopping or dining, because of inaccessibility of the community. Able people don’t consider the disabled in the building structures” (M5).
Significantly, despite these overt experiences of stigma and discrimination, mothers still wanted their children included in this society that appeared to reject them and their children. What they wanted and insisted on was increased public awareness about disability, as this was one of the main reasons for the stigma and discriminatory attitudes expressed toward their children.
Discussion
The findings of this study suggest that mothers had various cultural and religious explanations for the cause of their children’s disabilities, with some placing great emphasis on the role of the evil spirit (Jinn). This finding is congruent with religious and cultural beliefs reported by Muslim scholars (Croot, Grant, Cooper, & Mathers, 2008; Diken, 2006b), who reported that within the Pakistani and Turkish cultures, the evil eye and Jinn were highlighted as the most common cultural source of disability. The notion of “God’s will” emerged prominently in other studies of cultural perceptions of disability within Muslim communities (Croot et al., 2008; Daudji et al., 2011; Diken, 2006a, 2006b; Raman et al., 2010). Nevertheless, some important differences exist. Although disability is traditionally seen as a result of punishment from God or as a gift from God (Croot et al., 2008; Daudji et al., 2011; Diken, 2006b), with studies from South Asia showing that most mothers believe that their child’s condition was a punishment of their sins from God, the majority of this study’s participants attributed CP to an evil eye or evil spirit instead. Similarly to our study, a study exploring Iranian mothers’ lived experiences of having a child with cognitive disabilities revealed that accepting “God’s will” was the most important source of comfort for the mothers and created a positive outlook (Kermanshahi et al., 2008). This was further endorsed by Raman et al. (2010), who recognized that the strong religious beliefs held by Kuwaiti mothers provided them with a strategy to cope with their personal perspectives on disability and their extended caregiving role. Our findings also support recent research (Croot et al., 2008; Daudji et al., 2011) that shows that hope for the future among Pakistani and South Asian cultures is often faith-based. Similarly, parents’ beliefs about disability’s causes have been shown to have a significant impact on the perception and understanding of their children’s disability and expectations for their children’s future (Mandell & Novak, 2005).
Although some studies have found that religious beliefs might mean refusing treatment or early intervention services (Mirza, Tareen, Davidson, & Rahman, 2009), this was not an issue with the Saudi mothers interviewed here, with some seeking modern medical treatment. This is also consistent with the study by Diken (2006b), which revealed that mothers in Turkey use modern treatment methods by taking their children to medical professionals, although they also gave more emphasis to traditional treatment practices.
Although most mothers use religious and cultural causes as explanations for the CP, the medical terminology was also considered helpful. For example, two mothers used the baby’s lack of oxygen right after birth as a cause of the condition. This is consistent with previous research that has shown that mothers had adopted both “biomedical” and “traditional” explanations (Croot et al., 2008; Diken, 2006b; Raman et al., 2010). Cultural perspectives, mixed with religious values, often led to several courses of action. It was evident that the mothers generally rejected the diagnosis of CP and either justified their response by labeling their children as “normal” or identified their children’s condition as delayed motor development. This was considered as standing up for their children against social stigmatization. This finding is reinforced by McKeever and Miller (2004), who found that mothers would allow others to see their children’s worth in society by emphasizing the child’s “normal” development and not their disabilities. Therefore, to maintain hope, the mothers denied the diagnosis because it contradicted their image of having a healthy child, and they found it difficult to connect this image with a disability such as CP (Huang, Kellett, & St. John, 2010).
We would argue that a more nuanced understanding of how culture, disability, and motherhood interact, avoiding stereotypes and generalizations, is required to fully understand the beliefs and practices adopted by the mothers. The relationship between families and medical professionals is significant because in many cases, getting a correct diagnosis, as well as gaining the desired treatment, depends on the quality of the communication between parents and medical professionals (Kaba & Sooriakumaran, 2007). This is particularly evident in Western literature that suggests that parents in the United States often complain that professionals do not listen to them or take their views seriously (Ahern, 2000), and they sometimes respond by seeking another doctor or by searching for treatments on their own (Christon, Mackintosh, & Myers, 2010). Similarly, our study findings showed mothers claimed that the health care professionals did not listen to them and did not give them any information about their children’s condition. Until diagnosis, the perception of the child by the parents is changeable, often dominated by “but he looks so normal” and “positive visualizations” about the future. The experience and satisfaction with the diagnostic process at the hospital also depends on the setting, timing, and level of information, as well as the parents’ readiness for the information (Graungaard & Skov, 2006).
Wider social support and acceptance from members of the extended family has been found to influence parents’ views of their children’s disability (Ravindran & Myers, 2012). Kermanshahi et al. (2008) noted that some grandparents blamed parents, especially mothers, for a child’s disability, and so did not accept the grandchild. Similarly, our study showed that the extended family, and in particular the mothers-in-law, rejected children with CP, which reinforced negative social attitudes. Jackson and Mannix (2004) revealed that mother blaming was a burden for women because they internalized this concept in their lives and experienced distress due to their children’s misbehavior or disease.
Importantly, mothers reported stigma and a lack of support from their extended families and community. This finding is consistent with numerous other studies that have suggested that disabled children and their families are subjected to discrimination and stigmatization and that the discrimination experienced by disabled children and their families is persistent (Davis & Manago, 2016; Gray, 2002; S. E. Green, 2003). This may tend to have an isolating effect on the mother and child. This finding is reinforced by Azar and Badr (2006), who noted that extreme social isolation experienced by families with children with disabilities in Lebanon was due to the social stigma surrounding disability. It is also consistent with S. E. Green (2003), who reported that mothers who experienced a great deal of stigma related to their children’s disability reported higher maternal distress, which, in turn, decreased the frequency with which those children interacted with same-age peers. This was further supported by Al-Jadid (2013) and Hemdi (2010), who showed the need for accessible facilities and medical rehabilitation hospitals in the Kingdom of Saudi Arabia, not only in big cities but also in the peripheral areas. The findings of this study also support arguments for family-centered approaches, aiming to create a partnership-based approach between parents and medical professionals.
Limitations and Future Directions
This study was part of a larger study exploring mothers and children’s views. Due to time constraints, the sample size was restricted to six mothers; however, the sample size was adequate for data saturation, whereby discovered information was repeated, and the phenomenon became stronger and more evident (Morse, 2000, 2015). The homogeneity of the sample allowed for saturation to be reached with a smaller sample size (Boddy, 2016). A study on a larger sample would provide more information and a better understanding of the phenomenon. Another limitation was that the study focused on the experiences of mothers only, although CP has an impact not only on mothers and children but also on other family members. Future research should be directed toward other family members to create a genuine family context for understanding this disability in Saudi culture. It will also be useful to investigate the experiences of other people who work with “CP children,” such as health care providers and teachers.
Conclusions and Implications
This study provides a detailed account of a small number of Saudi mothers’ beliefs about the perception of the term CP through focused group discussion and follow-up interviews. It demonstrates how mothers hold multiple and apparently contradictory beliefs and explores how their children’s disability affected the daily lives of both mothers and their families. We explore how mothers created their coping strategies and, in some instances, resisted and even challenged the dominant culture of shame and blame. Our study will contribute to a theoretical base for health and social care practitioners to take into account mothers’ knowledge and experiences of living with a child with CP. It also highlights the importance of developing support or self-advocacy groups for mothers of CP children in Saudi Arabia, to empower them to be more involved and more aware of their children’s rights and reinforce their ability to cope with the challenging and demanding role of raising a child with CP.
Footnotes
Acknowledgements
The authors would like to thank all mothers who gave their time to take part in this study and openly shared their experiences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.