
Abstract
Background
The aim of this study was to assess practicing dentists’ characteristics and professional aspects that influence users to adopt Digital Technologies in Dentistry (DTD) in Saudi Arabia (SA). Moreover, we aimed to identify dentists’ perceived barriers and challenges and to anticipate future potential developments towards implementing DTDs in their practices in SA.
Methods
This analytical cross-sectional study based on a validated questionnaire was conducted using a snowball sampling technique to include a conveniently selected sample of dentists from all dental specialties currently working in SA.
Results
The response rate was 64% completed and returned. A statistically significantly large share of Gen X (10.1%) used digital technologies (DTs) in dental practice compared with non-digital users. 40% received sufficient postgraduate education on DT, 92% agreed that DT should be included in the undergraduate dental curriculum. However, 79% actually gained skills or knowledge on DT through workshops and formal courses. ‘Lack of practitioners’ awareness’, ‘lack of education and pioneers’ and ‘lack of clinical evidence’ were highlighted as the foremost barriers. Lower-frequency DT users believed that treating patients with DT makes treatment more predictable. Together, clinical trials and hands-on training courses can help overcome the barriers to the adoption of new dental technologies.
Conclusions
Exploring technology adoption and usage amongst practicing dentists allows healthcare stakeholders and policymakers to set a clear direction towards the digitalisation of the healthcare system and within healthcare organisations. The study also highlighted the foremost barriers, challenges and actions towards the adoption of DTDs.
Background
Modern dentistry relies heavily on the digital revolution, which now plays a pivotal role in the future of dentistry.1,2 The emergence of digital dental devices not only constitutes a technological transformation but also fundamentally reshapes the structure of healthcare systems, from the doctor–patient relationship to treatment processes. In addition, they have been increasingly incorporated into research, education and training. As a result of this paradigm shift in dentistry, patient records, data acquisition, clinical decisions and treatment options have improved.3,4 As an additional benefit, digital dental radiography reduces radiation exposure, improves imaging quality and requires fewer resources in the dental workplace. The use of intraoral scanning device (computer-aided design and manufacturing) technologies, three-dimensional (3-D) printing and new-generation materials has replaced traditional multistep procedures in chairside restorative and prosthetic procedures owing to the reduced working time and improved treatment outcomes of these technologies.3–6 Dental implants, 7 restorative, 8 orthodontics, 9 oral surgery and oral rehabilitation 10 have all explored the potential of digital dentistry in clinical procedures.
The rapid influx of digital dentistry has brought new horizons to daily clinical practice, but the extent and adaptation of its use vary significantly amongst dental practitioners. 11 Adapting new innovations is a complex and dynamic process heavily influenced by several variables, including but not limited to the technology itself, potential user, organisational setting and wider socio-political context.12,13 Several studies have investigated dentists’ adoption of digital technology (DT), providing valuable insights into their motivations. However, these studies have been limited to a particular type of DT. Challenges and barriers such as high initial costs, resistance to change, interoperability issues and data security concerns need to be addressed to facilitate the wider adoption of DT.11,13 Identifying and overcoming these challenges requires a deeper understanding of context-specific differences.
Whilst perception studies amongst dentists were highlighted elsewhere to investigate dental practitioners’ opinions on digital technologies in dentistry (DTD) and the relationships of these opinions with practitioners’ level of technology use, 14 a knowledge gap still exists in Saudi Arabia (SA) with respect to studies that assess dentists’ perceptions of and willingness to use DTs that await testing, despite the barriers and challenges that hinder their implementation in dental practice. Furthermore, a broader explanation of other determinants contributing to DTD use, such as generational differences, has not been explored. Whilst it adds to the literature on the findings of dentists in SA, it may also enable understanding of barriers and facilitators to implement improvement strategies that are conducive to both medical and dental practices and to subsequently initiate changes to the profession itself and the delivery of high-quality care to patients. The findings of this study may influence the guidelines of the Saudi Commission of Health Specialties, dental educational institutions and dental practices with respect to implementing relevant DTDs in dental practices. Therefore, an exploratory study to assess the feasibility of the study protocol, amongst other purposes, is needed to set the foundation for conducting a larger multi-lenses study.
Aim
The aim of this study was to assess practicing dentists’ characteristics and professional aspects that influence users to adapt DTDs in SA. Moreover, we aimed to identify dentists’ perceived barriers and challenges and to anticipate future potential developments towards implementing DTDs in their practices in SA.
Materials and methods
Study design and setting
This analytical cross-sectional study was conducted from February to April 2021 and included a conveniently selected sample of dentists from all dental specialities who were currently working in the 13 administrative regions of SA. The study categorised the regions into central, western, eastern, northern and southern.
Recruitment of participants, data collection method and variables
The sample size was estimated using Epi Info StatCalc at a confidence level of 95%, with an alpha error of 5% and a beta error of 20%. The calculated sample size was 349, which was increased to 980 to account for non-responders and non-technology users.
Owing to the quarantine circumstances in SA during the pandemic, a snowball sampling technique was adopted to recruit study participants from different regions of SA. First, all of the study investigators forwarded the online survey to selected dental interns in different regions. The interns then forwarded the online survey (Google Forms, Google Inc., California, USA) to their social media (e.g., WhatsApp and emails) contacts who met the study criteria. Both the interns and their social media contacts were requested to pass the survey to their contacts who met the study criteria. The same process was continued until the calculated sample of the study was obtained. Upon completion of the questionnaire, the respondents were instructed to submit the web form through the web server. The web server then transferred the data to a spreadsheet for analysis (Excel, Microsoft Corp., New Mexico, USA). The time needed to respond to the questionnaire was approximately 15 min.
The anonymous closed-ended English questionnaire included a covering page that explained the purpose of the study, the voluntary nature of participation, the confidentiality of the obtained data and institutional review board approval. Information about the researchers was also provided in the case of further queries.
The validated questionnaire asked about covariates, including socio-demographic and practice characteristics and explanatory DT usage and perception variables, specifically the general perception of DTD, personal experience, challenges, barriers and perceived actions.11,15,16 The socio-demographic information included the participants’ sex, age, nationality, working region and highest degree obtained and the year it was obtained. Age was further categorised according to the generational cohort in 2021 as ‘Boomers II’, aged 66 through 57 years; ‘Gen X’, aged between 56 and 41 years; ‘Millennials’, aged between 40 and 25 years; and ‘Gen Z’, aged between 9 and 24 years. This categorisation was created because each commonly used current generation has been defined by a unique combination of factors related to technology usage. The participants’ specialities were further categorised into general dentistry, preventive science, diagnostic science and clinical science.
Nineteen digital dental technologies were identified as presently available and most relevant to dental practitioners based on a previous study 11 and discussion between the authors. These technologies were divided into four administrative and communicative technologies, eight clinical technologies and seven diagnostic technologies. The questionnaire included previously validated questions to measure dental practice characteristics and dentists’ perceptions on using DTs in dental practice. 16
The participants were asked to express their agreement with six evidence-based perceived personal challenges when using DTD. 15 They were also asked to rank barriers in relation to the perceived influence of the barrier in preventing the adoption of DT (influence attribute). 15 The range of the ranked scales was equivalent to the number of barriers; that is, where five barriers were present, the participants were asked to rank influence using a scale of 1–5 (higher rank [1] = most influence). In addition, the dentists were asked to rank actions according to the actions they perceived as necessary to encourage embracing DTs in their practice. 15 The range of the ranked scales was equivalent to the number of actions; that is, when six actions were present, the participants were asked to rank influence using a scale of 1–6 (1 = most encouraged).
Data analysis
After the survey closed, the spreadsheets were downloaded and imported into the latest statistical software version for data analysis (SPSS Inc., Armonk, NY, USA). The socio-demographic categorical characteristics of the entire sample and DT use in dentistry (user vs. non-user) were summarised and reported as frequencies and percentages or as median and interquartile range. The associations of the socio-demographic and clinical practice characteristics with the exploratory variables were examined using an independent-samples t test, Kruskal–Wallis test, Mann–Whitney U test and chi-square test. The significance level was set at p < 0.05.
The DT users’ data were then categorised into three groups according to the number of technologies used. 17 The low-frequency technology users used 0–4 DTs of the most frequently used type and included 66.4% of the dentists. The intermediate-frequency technology users used 5–7 digital dental technologies, including those that were very and less frequently used (17.7%). The high-frequency technology users used eight or more DTs, including frequently used technologies and one or more less often used technologies (15.9%). The differences in perception, specifically general perception of DTD, personal experience and challenges, amongst the three levels of DT use were assessed. Associations with previously mentioned exploratory variables were examined using the chi-square test, and the significance level was set at p < 0.05. Furthermore, pairwise comparisons for DTD barriers and possible actions were performed using the Friedman test.
Results
Sample characteristics
Of the 980 questionnaires sent, 621 (response rate, 64%) were completed and returned. Of the total participating dentists, 327 (53%) reported using DT in their dental practices. The median age of the DT users was significantly more likely to be older (median age, 31 years) than the non-DT users (p < 0.001). Of the total sample, 78.3% were grouped into the millennial generation. However, a statistically significantly large share of Gen X (10.1%) used DTs in dental practice compared with non-DT users (4.4% and 1.6%, respectively). No significant sex-related differences were found between the DT users and the non-DT users (Table 1).
Socio-demographic and practice characteristics of respondents (n = 327) and within the digital technology user groups.

Interquartile range (IQR).
Chi-squared and Mann–Whitney U tests used for comparisons of proportions and correlation.
*p < 0.05, deemed significant.
The participants who held a postgraduate qualification were significantly more likely to use DT than those who had no postgraduate qualification (34.5% vs. 29.2%). The DT users were statistically significantly more likely to work in the eastern region (17.8%) of SA, whereas a higher percentage of non- DT users (15.8%) worked in the central region. Table 1 displays the characteristics of the study sample and the differences between digital and non- DT users. Those who worked in the government sector and had longer years of clinical experience been significantly more likely to be engaged with DTs than those who worked only in the private sector or had fewer years of clinical experience (33.4% and 6 [8] vs. 20.4% and 4 [6], p < 0.001).
Digital technology users’ practice characteristics
Of the participants who used DT, 40% received sufficient postgraduate education on DT, 92% agreed that DTD should be included in the undergraduate dental curriculum and 79% actually gained skills or knowledge on DT through workshops and formal courses. No significant differences were found between the levels of DT users in terms of years of experience using technology in practice, whether they received adequate postgraduate education on DT or from which source they obtained their knowledge (Table 2).
Digital technology user characteristics.

Interquartile range (IQR).
Chi-squared and Mann–Whitney U tests used for comparisons of proportions and correlation.
Opinions of the participants and the challenges they experienced
As shown in Table 3, a statistically significant percentage of lower-frequency DT users (41%) believed that treating patients with DT makes treatment more predictable compared with the high-frequency DT users (7%, p < 0.038). In addition, compared with those who used DT more frequently, those who used DT less frequently believed that it simplified their daily work (Table 3).
Respondents perceptions towards digital technology by digital technology users’ groups (n = 327).

Chi-squared and Mann–Whitney U tests used for comparisons of proportions and correlation.
*p < 0.05, deemed significant.
Perceived barriers to the incorporation of DT into clinical practice
As for the barriers to the incorporation of DT into clinical practice, Table 4 demonstrates that 27%, 24% and 23% of the dentists ranked ‘lack of practitioners’ awareness’, ‘Lack of education and pioneers’ and ‘lack of clinical evidence’ as the most frequent barriers. However, less dentists ranked ‘lack of patient awareness and acceptance’ as the least barriers. The mean rank of the highest-ranked barriers to incorporating DT into clinical practice was ‘lack of practitioner awareness’ (2.35), followed by ‘lack of education and pioneers’ (2.78), and the least-ranked barrier was ‘lack of patient awareness and acceptance’ (4.09). The overall Friedman test result indicated a significant difference between the mean ranks of the four executing actions (i.e., χ2 (4) = 234.2, p < 0.001). The post hoc pairwise comparison analysis (Table 4) revealed no significant differences between ‘lack of education and pioneers’ and ‘lack of clinical evidence’ or ‘lack of sustainable technical support’ (mean rank, 2.78 and 3.13 or 3.66, respectively).
Distribution of responses (frequency and percentages), mean rank and pairwise comparisons for DTD barriers and possible actions (n = 327).
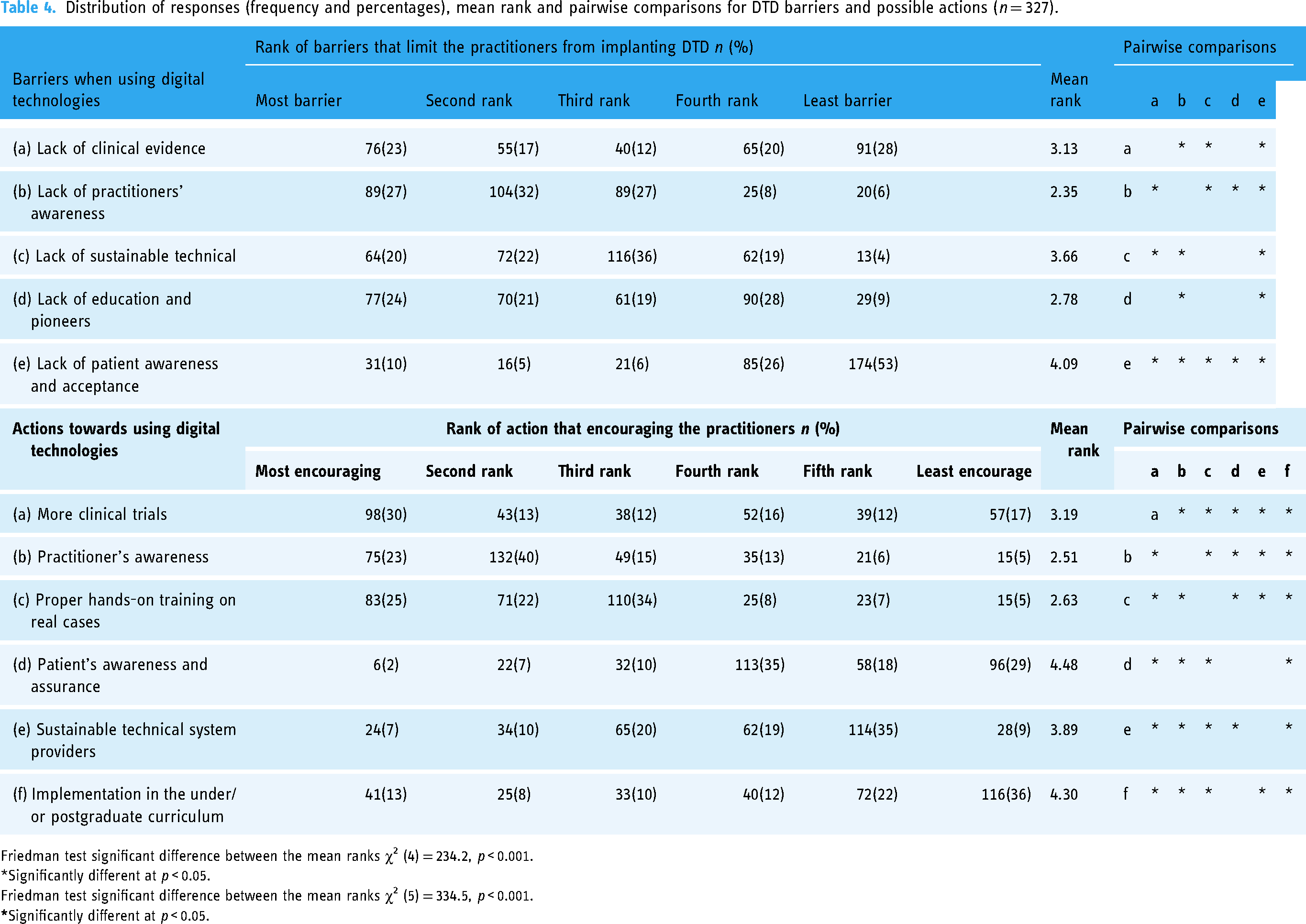
Friedman test significant difference between the mean ranks χ2 (4) = 234.2, p < 0.001.
*Significantly different at p < 0.05.
Friedman test significant difference between the mean ranks χ2 (5) = 334.5, p < 0.001.
Actions required to enhance DT practice in dentistry
The need for more clinical trials was ranked as the most encouraging action to enhance DT use in dental practice by 30%, followed by proper hand-on training or real cases (25%). However, less dentists ranked ‘Patient's awareness and assurance’ as the most encouraging action required to improve DT use in dentistry (2%). The Friedman test result indicated a significant difference between the mean ranks of the six actions (i.e., χ2 (4) = 334.5, p < 0.001). The post hoc pairwise comparisons revealed significant differences in mean ranks between most of the actions except ‘sustainable technical system providers’ and ‘patient's awareness and assurance’ (mean ranks, 3.89 and 4.48, p > 0.05) and between ‘implementation in the undergraduate or postgraduate curriculum’ and ‘patient's awareness and assurance’ (mean ranks, 4.30 and 4.48; p > 0.05).
Discussion
This study aimed to assess dentists’ perceptions of and willingness to use DTs and to identify the barriers and challenges that may hinder their implementation in dental practice. Digital Technologies in Dentistry was adopted by over half of the respondents in their daily dental practices; however, there were no significant differences based on gender. Since age has been demonstrated to be an influential demographic variable in predicting individual use during new technology implementation, 18 generational differences amongst DTD users were also examined. Although millennials constituted the majority of our sample, GenX has integrated technology more seamlessly into their daily practices than millennials. Contrary to another study, 19 this finding indicates that GenX dentists may have accumulated more years of experience and, therefore, been exposed to more DTD compared to younger dentists. There is a lack of research in the literature on the effect of generational differences on DTD adoption amongst dentists, and this study may serve as a benchmark for future longitudinal studies that would be crucial to understanding this phenomenon. Furthermore, those who worked in the government sector were significantly likelier to be engaged with DTs. The Saudi Arabian government places a high priority on utilising DTs and transforming the health industry as well as introducing new approaches to patient care. 20 Considering that it provides 60% of SA's healthcare, the Ministry of Health has a strong focus on developing digital infrastructure for governmental healthcare, perhaps explaining this trend. 21
To prepare the younger generation for technological advances and increase their ability to adapt later in life, DTD training and direct interaction are required early in the undergraduate dental curriculum. Interestingly, most study participants agreed that integrating DTD training into undergraduate curricula would have a positive impact on dentists and that early exposure to DTD can contribute significantly to career choices and technology adaptation. Numerous dental schools worldwide have introduced DTD as a part of their undergraduate dental curricula as a component of their preclinical and clinical courses22–25 found that it has a substantial impact on education and holds great promise for improving patient care. However, some Saudi schools fail to fully utilise the advanced DTs they have acquired because faculty members are not adequately trained to use them. 26 To address this, it is advisable to provide training for dental faculty to promote the integration of DTD into students’ practices.
There were no significant differences amongst DT users when it came to years of practice using technology, postgraduate education on DT or where they acquired their knowledge. One possibility is that the study's measurement instruments for assessing years of experience, education and source of knowledge may not have been sensitive enough to capture meaningful variations amongst the DT users in the sample. Another possible explanation is that years of experience, education and source of knowledge may not be the most relevant factors for determining levels of proficiency with DT amongst users. It is possible that other factors, such as innate ability, motivation and self-directed learning, may be more important determinants of DT proficiency.
Our findings are also in line with other studies in which the incentives brought by DTD, such as relative advantages, enhanced treatment predictability and ease of use, might justify this wider acceptance.27–29 However, the adoption of DTD goes beyond technical aspects. To anticipate future developments in the field of digital dentistry and to promote further uptake and diffusion, it is essential to investigate the challenges and additional constraints imposed on Saudi dentists to incorporate DDT into their clinical practices. Amongst our cohort, ‘lack of practitioners’ awareness’, ‘lack of education and pioneers’ and ‘lack of clinical evidence’ were highlighted as the foremost barriers. Studies in agreement with our findings indicate a lack of clinical evidence regarding various dental technological devices, thereby reducing dentists’ interest in DT.11,30–32 Furthermore, studies that explored the barriers to innovation within the healthcare sector highlight cost as a major limitation facing adaptors, along with lack of interest, comfort and training pertaining to redundancy and the abandonment of technical developments.11,32 These findings can be justified as the continuous and rapid emergence of new innovations in the dental profession and the associated risk of rapid obsolescence and replacement of certain innovations, which requires constant awareness and training by dentists to cope with recent advances. Additionally, existing studies have reported a wide range of other barriers from the individual, organisational and socio-political perspectives that may complicate the understating of how these barriers affect adoption decisions.11,16,17 To nurture this promising field, interdisciplinary collaborative studies are needed to overcome the impeded obstacles and to accelerate the rate of DTD adoption in daily practice.
Despite dentists’ willingness to embrace DTD in their daily practice, respondents ranked more clinical trials as the most encouraging action to enhance DTD use in dental practice, followed by proper hands-on training or real-life experience. Clinical trials and hands-on training courses are essential for improving the adoption of dental technologies in practice. Clinical trials provide evidence of the safety and efficacy of new technologies, which can help dentists make informed decisions about whether to invest in and use them. The availability of well-designed and well-executed clinical trials can also help to build trust in new technologies amongst dentists, dental technicians and patients. Furthermore, hands-on training courses can help dentists and dental technicians acquire the skills and knowledge needed to use new technologies effectively. 11 These courses can provide hands-on experience with the technology and allow participants to learn from experienced practitioners. A sensible recommendation is to incorporate mandatory hands-on training on DTD as a part of dental licensing and license renewal.
Today, DT has revolutionised dental care, making it more affordable and accessible. 33 Additionally, it has allowed for more personalised and minimally invasive treatments, as simulations can be tailored to each patient's individual needs. 33 Additionally, technologies driven by artificial intelligence can improve dental procedures by enhancing their precision and efficiency.34,35 By analysing patient-specific data, such as CT scans, an artificial intelligence program can provide dentists with real-time guidance during surgery. 36 Digital technologies and artificial intelligence provide synchronous solutions to challenges facing dental professionals and healthcare providers worldwide.
Strength and limitation
This study's strengths lie in its comprehensive reflection of different variables that would affect the adoption of DTD amongst dentists while addressing the challenges that are necessary to encounter during embracing these technologies into their practices. Another strength is the inclusion of wide variety of dental practices across SA, including private and governmental clinics. Furthermore, the current study used a validated questionnaire adopted from previous studies. Our study was limited to a self-administered questionnaire; therefore, the information bias could not be ruled out.
Conclusion
Being from GenX and working in the governmental sector have been shown to help dentists integrate technology more seamlessly into their daily practices. ‘Lack of practitioners’ awareness’, ‘lack of education and pioneers’ and ‘lack of clinical evidence’ were highlighted as the foremost barriers. Together, clinical trials and hands-on training courses can help overcome the barriers to adoption of new dental technologies. The Vision 2030 roadmap released by the Saudi government sets out a clear direction towards the digitalisation of the healthcare system and the increased investment in new technologies within healthcare organisations. Technology use and implementation have become so ubiquitous that they are now considered routine parts of daily operations. Therefore, exploring technology adoption and usage has become a topic of broad interest in the research field of technology. To ensure rational and efficient shifting from human-centred healthcare to digital systems, policymakers and stakeholders must understand the characteristics of users to embrace successful implementation.
Footnotes
Acknowledgements
The authors would like to thank Abdulsamad Talaat Habeeb, Eman Ali Alkhudairy and Yasmeed Yahya Muazen for aiding in data collection.
Contributorship
HR, AA and MA have contributed to conceptualisation, Data curation, analysis, Writing-Original Draft-Review & Editing. HR completed the questionnaire validation, distribution and management. MA and BA helped in data collection and writing-literature review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and validated. The study design was approved by the appropriate ethics review board of Prince Sultan Military City Scientific Research Center IRB Approval (No. 1457).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Guarantor
HAR.
Participant consent
This manuscript presents a literature review of publicly available information. For survey participants, no individual data were used for the analysis presented in this manuscript. Completion of the questionnaire was indicative of their consent to participate.