
Abstract
Introduction
This study aims to examine (1) the impact of the pandemic phases on overall and preventable hospitalizations and emergency department (ED) visits, and (2) the effect of the pandemic on these outcomes within subgroup populations including gender, race, patients’ residence in health professional shortage areas (HPSA), and residence in a federal poverty level.
Study Design
We used electronic medical record (EMR) data for the year 2019 and 2020 from a large health system predominantly serving medically underserved patients in the South. We used a difference-in-differences approach to examine changes in weekly rates of overall and preventable hospitalizations and ED visits in the pandemic phase 1 (Mid-March to June of 2020) and phase 2 (July-September of 2020) compared to the same period in 2019 after adjusting for weekly outcome rates in the baseline period (January to Mid-March of 2020) compared to the same period in 2019.
Results
The study sample included 1.4 million hospitalizations and ED encounters. In phase 1 of the pandemic, there were significant reductions in overall (−108) and preventable (−75.3) hospitalizations, and overall (−408) and preventable (−306) ED visits when compared to the same period in 2019. In phase 2 of the pandemic, there were significant reductions in overall (−60) and preventable (−43) hospitalizations and in overall (−360) and preventable (−258) ED visits as compared to 2019. We found greater reductions in ED visits, both overall and preventable, during the early pandemic phases among Black patients than among White patients. Similar patterns in the reduction of ED visits were found in Black versus White patients within subgroups of women, men, and those residing in a HPSA and low-income areas.
Discussion
Substantial reductions in utilization were observed in Black patients in comparison to white patients and these differences persisted among men, women, and those living in underserved and low-income areas.
Keywords
Introduction
A crucial health policy issue centers on how to manage the care and costs related to ambulatory care sensitive conditions (ACSCs). ACSCs are health conditions, including hypertension, diabetes, congestive heart failure, and coronary artery disease, that need to be treated effectively with continuity of care and in a timely manner in outpatient settings by primary care providers. ACSCs are associated with preventable hospitalizations or emergency department (ED) visits and are widely considered as a proxy for access to effective health care. 1 Treating and managing ACSCs effectively and in a timely manner in an outpatient setting can prevent the need for inpatient care.2–7
During the COVID-19 pandemic, disruptions in outpatient care delivery could have impacted continuity of care for patients with ACSCs. Evidence shows that there were reductions in hospitalizations for acute events including stroke and myocardial infarction. 8 Additionally, Black or African Americans and those residing in low-income areas were disproportionately affected by COVID-19 and were more likely to be hospitalized.5,9–11 However, little is known regarding the impact of COVID-19 pandemic on preventable hospitalizations and ED visits among medically underserved populations with ambulatory care sensitive conditions (ACSCs). 12 In fact, the empirical evidence is unclear regarding the extent to which the overall changes in preventable hospitalizations and ED visits are assembled among specific race/ethnic groups. 12
Our study helps fill the void in this literature by examining the effect of the pandemic on healthcare utilization among medically underserved populations with ACSCs who are at higher risk for severe illness from COVID-19. The study aimed to examine (1) the impact of the COVID-19 pandemic phases on overall and preventable hospitalizations and ED visits and (2) examine the effect of the pandemic on these outcomes within subgroup populations classified based on sociodemographic characteristics including gender, race, and patients’ residence in health professional shortage areas (HPSA) and in a poverty level.
Methods
Data Sources
Electronic medical records (EMR) data were used for the year 2019 and 2020 from five adult hospitals belonging to a large healthcare delivery system in the Memphis Metropolitan Statistical Area in the South. The health system predominantly serves medically underserved patients. EMR data is part of the Tennessee Population Health Data Network (TN-POPnet), a data network that includes patient level information including their demographics, diagnosis, health care utilization, procedures, vitals, and laboratory data. 13 Patient-level data were linked with the zip code-level factors obtained from the National Historical Geographic information System (NHGIS) 14 and Centers for Medicare and Medicaid Services (CMS) 15 databases using patient residence zip codes.
Study Design and Population
This study uses a quasi-experimental difference-in-differences (DID) approach. The study included adult (18+ years) patients with a diagnosis of ACSCs including diabetes mellitus, hypertension, chronic heart failure, coronary artery disease, chronic obstructive pulmonary disease, and asthma. The study included encounter-level EMR data that included a period that was divided into two early pandemic phases: the pandemic phase 1 (Mid-March to June of 2020) and pandemic phase 2 (July-September of 2020). These pandemic phases were compared to the same periods in 2019 (Mid-March to June of 2019 and July-September of 2019) after adjusting for the baseline period (January to Mid-March of 2020) compared to the same period in 2019.
Outcome Measures
The outcomes included overall, and preventable hospitalizations and ED visits calculated for each week in the baseline, phase 1, and phase 2 of 2020 and 2019. Hospitalizations included inpatient and observation visits. The Agency for Healthcare Research and Quality Prevention Quality Indicators (PQI) chronic composite measures were used to define potentially preventable hospital and ED utilization. These measures included visits for diabetes short-term complications, diabetes long-term complications, COPD or asthma in older adults, hypertension, angina without procedure, uncontrolled diabetes, asthma in younger adults, and lower-extremity amputation among patients with diabetes. 16
Independent Variables
Patient-level subgroup factors included gender (male, female) and race (white, black). Zip-code level factors assessed for each patient included patients’ residence in health professional shortage areas (HPSA) or low-income areas (HPSA/low-income areas, non-HPSA/non-low-income areas) and proportion of patients living in zip-codes with income less than 100% of the federal poverty level (FPL). The FPL variable, a continuous measure was converted to a binary variable. Patients who resided in zip-codes with majority individuals (>50% individuals) under the FPL were assigned 1 else they were assigned 0.
Statistical Analysis
Weekly rates for all outcomes were assessed for the year 2019 and 2020. These rates were plotted to examine trends in health care utilization in 2020 in comparison to 2019. Additionally, we used a difference-in-differences analytic approach to examine changes in weekly rates of overall and preventable hospitalizations and ED visits in the pandemic phase 1 (Mid-March to June of 2020) and phase 2 (July-September of 2020) compared to the same period in 2019 after adjusting for weekly utilization rates in the baseline period (January to Mid-March of 2020) compared to the same period in 2019. The mathematical equation for the difference-in-differences model is shown below.

We conducted analyses in the overall population and subgroups including race (White and Black), gender (male and female), residence in HPSA or low-income areas (HPSA/low-income areas and non-HPSA/non-low-income areas), and residence in zip codes with majority low-income individuals. To gain insights into mechanisms behind racial disparities, we examined differences in utilization patterns between Whites and Blacks within subgroups including gender (White males and Black males; White females and Black females) and residence in HPSA (Whites living in HPSA or low-income areas and Blacks living in HPSA or low-income areas), and low-income areas (Whites living in areas with majority population under FPL and Blacks living in areas with majority population under FPL).
Results
The study sample included 1.4 million hospitalizations and ED encounters. Figure 1A and B show trends in overall and preventable hospitalizations in 2019 and 2020 among adults with ACSCs. These graphs show reductions in hospitalizations in the phase 1 and phase 2 of the pandemic, however, the reductions were greater in the phase 1 than phase 2. Figure 2A and B show trends in overall and preventable ED visits in 2019 and 2020 among adults with ACSCs. There were reductions in ED visits in both phase 1 and phase 2 of the pandemic. The difference-in-differences models show that in phase 1 of the pandemic, there were significant reductions in overall (−107.5 [−150.8, −64.2]) and preventable (−75.3 [−106.4, −44.2]) hospitalizations, and overall (−408.2 [−516.3, −300.0]) and preventable (−306.6, −387.8, −225.5]) ED visits when compared to the same period in 2019. In phase 2 of the pandemic, there were significant reductions in overall (−60.3 [−92.9, −27.7]) and preventable (−43.1 [−67.2, −19.0]) hospitalizations and in overall (−360.0 [−450.1, −269.9]0 and preventable (−258.5 [−328.3, −188.8]) ED visits as compared to 2019 (Table 1).
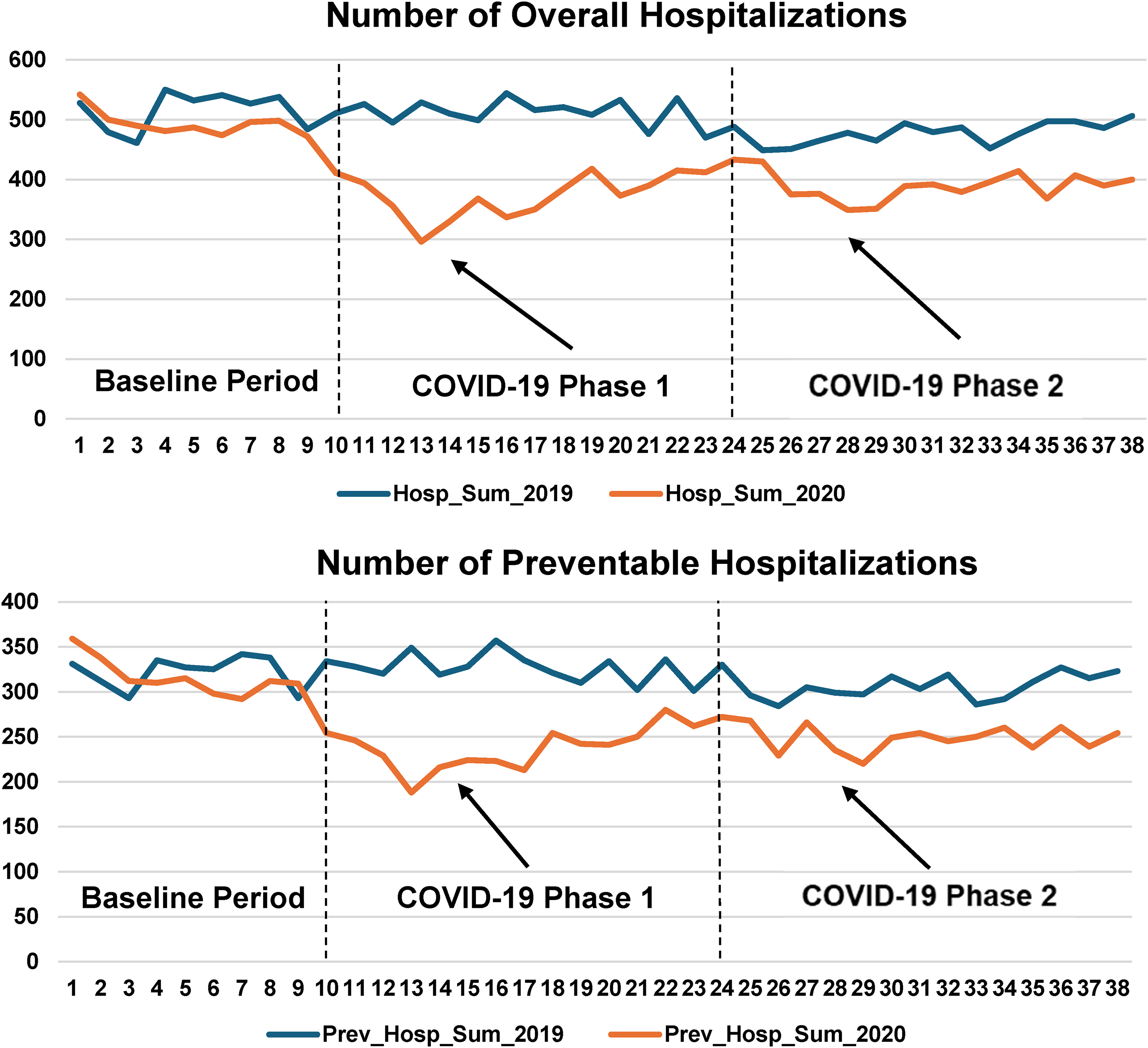
(A and B) Trends in overall and preventable hospitalizations in 2019 and 2020 among adults with ambulatory care sensitive conditions.a X axis represents weeks and Y axis represents total number of overall hospitalizations (Figure 1A) and preventable hospitalizations (Figure 1B).

(A and B) Trends in overall and preventable emergency department visits in 2019 and 2020 among adults with ambulatory care sensitive conditions.a X axis represents weeks and Y axis represents total number of overall emergency department visits (Figure 2A) and preventable emergency department visits (Figure 2B).
Difference -in-Differences Findings for the Overall and Preventable Hospitalizations and Overall and Preventable Emergency Department Visits among Patients with Ambulatory Care Sensitive Conditions.

We found significant reductions in overall and preventable hospitalizations during both phases of the pandemic among patients of white race as well as black race (Table 1). However, reductions in ED visits (both overall and preventable ED visits) during early pandemic phases were much higher among patients of black race than white race (Table 1). Similar patterns were observed in ED visits in our subgroup analyses when we compared utilization patterns between black race with white race among females, males, those residing in HPSA, and low-income areas (Table 2). The reductions were very pronounced among Black women between baseline and the first phase for both ED visits and especially with the preventable ED visits.
Difference in Difference Findings among Subgroup Populations for the Overall and Preventable Hospitalizations and Overall and Preventable Emergency Department Visits among Patients with Ambulatory Care Sensitive Conditions.

Among other factors, we found significant reductions in overall and preventable hospitalizations during both phases of the pandemic among men and women (Table 1). However, reductions in ED visits (both overall and preventable ED visits) during early pandemic phases were much higher among women than men (Table 1).
Discussion
In this study, we found a significant reduction in hospitalizations (both overall and preventable), a finding that is consistent with previous US based research,1,17,18 as well as non-US based studies from OECD countries.19–24 Furthermore, reductions in overall ED visits suggest that patients could have avoided going to ED facilities for nonurgent as well as urgent services. 25
Additionally, we found that Black patients had greater decreases in both overall and preventable ED visits during the early phases of the COVID-19 pandemic than their White counterparts. These findings are in accordance with several other studies that also found Black patients having higher rates of ED utilization than White patients. 26 This may have occurred because Black individuals are more likely to be on either Medicaid and/or uninsured and are less likely to have ongoing primary care and therefore use EDs as a “safety net of health care”. 27 Moreover, we found that there were higher reductions from baseline through the initial pandemic period for black patients residing in a HPSA, and for Black women. These findings are consistent with another study that found that black patients had lower than expected levels of ED visits during the early phase of pandemic. However, unlike this previous study that found rebound in ED visits among blacks, we found that significant reductions in ED visits persisted among blacks after the first 3 months of the pandemic. 12 Our study adds to the existing literature by not only examining racial differences in hospitalizations and ED visits, but also examining these racial differences by gender and HPSA status.
Our study aimed to contribute to a nascent body of literature that differentiated between preventable and overall hospitalizations and ED visits using data from a large ambulatory-care-based healthcare system that serves a racially diverse, large population of low-income patients. Additionally, we employed a quasi-experimental difference-in-differences approach to account for any selection bias that could occur in the examination of racial differences in hospitalizations and ED encounters. 28 This same approach was used to examine health care utilization patterns between blacks and whites by gender, HPSA designation, and income.
Several limitations of the current study exist. First, the generalizability of our findings is limited by our focus on a single geographical MSA in the US. Therefore, our findings may not be generalizable outside of this single geographical MSA in the US, but also for non-US countries. For instance, studies from Low-to-Middle Income Countries (LMICs) argued that healthcare performance before, during and after COVID-19 is contingent upon health care financing factors in these countries that vary from the US.29,30 Second, electronic health record data were used from practices serving predominantly Black patients and likely not generalizable to more racially diverse populations. Third, all our patients had an ACSC, a diagnosis that is associated with high rates of mortality and morbidity. However, it is unclear how our findings are applicable to individuals who do not have a ACSCs (eg, a severe mental illness). Fourth, our results emerged from an observational study. Therefore, we were only able to explore the association between a limited set of demographic, clinical factors and hospitalization and ED utilization and not causality. Despite the extensive number of studies on ACSCs hospitalizations as a proxy for health care quality, ACSCs hospitalizations may be a marker of other factors (eg, social determinants of health) beyond access to high quality of primary care. 2
Conclusion
Our study findings highlight the differences in hospitalizations and ED visits among medically underserved populations with ACSCs in a single geographical MSA in the US. We found significant reductions in overall and preventable hospitalizations and ED visits during the early phases of pandemic. More specifically, we found a significant reduction in hospitalization rates in the early phase of the pandemic, but this trend bounced back in the following phase. Our findings have implications for organizational aspects of access and supply of primary care providers. An abundance of studies suggest that strong and regular primary care in terms of the supply for primary care physicians and having a regular and consistent primary care provider reduces hospitalizations for chronic ACSCs. 5 Our findings also have implications for the importance of timely access to primary care, a longstanding health policy tenet. For instance, over 20 years ago, Blanchard and colleagues 31 indicated that EDs became a “safety net of health care” for people of color and who did not have insurance. 27 Not surprisingly, Black individuals are more likely to designate the ED as their routine place of healthcare, even after adjusting for health insurance. 27 However, with reference to both overall ED visits, as well as preventable ED visits, subgroup analyses found an intersection of race and gender. That is, we found that for Black women, there was a substantial reduction in overall and preventable ED visits between baseline and the first COVID-19 period, and this reduction experienced only a modest bounce-back as time persisted. Our data further suggests that monitoring hospitalization and ED data for adults with ACSCs like we did in the present study can help planners and policy makers and can inform outreach efforts to Black patients, especially Black women, who were most impacted, guaranteeing that they have a seamless and timely access to appropriate levels of care and means to assist them to establish the most suitable care setting. 32 Such actions are critical because ED visits are mission-critical for hospitals and a key source of inpatient admissions. 33 However, at present, ED overcrowding (where an identified demand or emergency medical services exceeds the resources available to treat patients in the ED, the hospital or both) is a persistent problem and is associated with worsening patient outcomes. 34 Despite the fact that we report on data on a single healthcare system in one MSA in the US, our findings have implications for OECD countries. Indeed, a recent systematic review called for the importance of developing and implementing a conceptual framework for inter-country comparisons of ACSC hospitalizations. 21 Health systems and policymakers should focus on strategies to improve chronic disease management during pandemic among socioeconomically disadvantaged populations. Moreover, findings from the present study may have significant public health consequences and warrant additional studies using mortality data because it is unclear the clinical consequences and health outcomes may be for patients, especially Black patients and Black women, in particular, for not receiving inpatient care that may need emergency treatment. 17
Supplemental Material
sj-docx-1-hme-10.1177_23333928241283367 - Supplemental material for Impact of the COVID-19 Pandemic on Healthcare Utilization among Medically Underserved Patients with Ambulatory Care Sensitive Conditions
Supplemental material, sj-docx-1-hme-10.1177_23333928241283367 for Impact of the COVID-19 Pandemic on Healthcare Utilization among Medically Underserved Patients with Ambulatory Care Sensitive Conditions by Neale R. Chumbler, Deborah O. Ogunsanmi and Satya Surbhi in Health Services Research and Managerial Epidemiology
Footnotes
Acknowledgments
The authors would like to acknowledge faculty members including Aram Dobalian, PhD, JD, MPH; Jim Bailey, MD, PhD; Page Powell, PhD; and Courtnee Melton-Fant, PhD for their assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the University of Tennessee-funded 2020 Collaborative Research Network (CORNET) Awards for COVID-19 Research (PI: Satya Surbhi).
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.