
Abstract
Objective
To determine the effectiveness of communication training and its impact on burnout among healthcare providers (physicians, physician assistants, nurse practitioners), in the setting of the COVID-19 pandemic.
Methods
To evaluate the effectiveness of communication training on burnout during the COVID-19 pandemic, healthcare providers participating in a Communication in Healthcare (CIH) module between October 31, 2019, through February 20, 2020, were identified using a scanned sign-in sheet. A 3-question online survey regarding the utilization of communication skills during the COVID-19 pandemic was sent via email. An ordinal scale was used to rate the effectiveness of the training on subsequent burnout and work satisfaction during the pandemic.
Results
Of the 98 surveys distributed via email, a total of 33 participants completed the survey. Seventy-three percent of respondents agreed that communication training helped prevent burnout, and 39% strongly agreed that the modules improved work satisfaction.
Conclusion
Our study found communication training was effective in reducing burnout in healthcare providers, in the setting of the COVID-19 pandemic. The participants felt the communication tools learned from the training modules were useful in improving work satisfaction and communication with patients during the pandemic.
Introduction
As COVID-19 evolved into a pandemic, stressors developed, not only on the medical system, but also on the clinical providers themselves. Limited resources, a novel pathogen, and significant risk of spread to providers are just some of the many pressures facing the healthcare community. During times of intense crises, uncertainty and loss of control can lead to significant stress for health care providers and contribute to burnout.1,2 Learning from past experiences, we understand that a pandemic not only has health implications for patients, but also untold consequences for their healthcare providers.3–5 Additionally, this impact on personnel has highlighted the need for strategies and techniques to decrease provider stress and reduce burnout.
Since 2007, Mayo Clinic Florida (MCF) has incorporated communication training as part of the onboarding process for all advanced clinical providers, including physicians, physician assistants, and nurse practitioners. The curriculum includes didactic and small group exercises focusing on skills to build a rapport and effectively communicate with patients. These skills are developed utilizing communication tools including PEARLS (Partnership, Empathy, Apology, Respect, Legitimization, Support) and SPIKES (Setting up, Perception, Invitation, Knowledge, Emotions, Strategy/Summary).6,7 This training articulates the importance of patient centered healthcare as it has been associated with improved and safer healthcare outcomes, greater patient satisfaction, improved compliance, fewer complaints, as well as reduced provider burnout.6,7
Mayo Clinic has historically used worldwide crises as a catalyst to adapt, innovate and transform healthcare. Over the last two decades, as provider burnout was recognized as a modern healthcare crisis, Mayo Clinic has again used crisis as a catalyst for change, by expanding our focus to include research on strategies to mitigate burnout. 8 We theorize that enhanced communication skills lead not only to improved patient outcomes, but also have an added benefit of improving provider well-being and decreasing stress. Thus, the aim of our study was to assess the effectiveness of our course on communication training as a means of reducing provider burnout in the setting of the COVID-19 pandemic.
Methods
This study was deemed exempt by the institutional IRB. Physicians, physician assistants, and nurse practitioners from MCF who had completed one of our two Communication in Healthcare (CIH) modules (Effective Communication in Healthcare or Cross Cultural Communication in Healthcare) from 10/31/2019–2/20/2020 were asked to complete the survey via email. Surveys were sent out in May 2020, 3–7 months after participants had completed the modules. The survey (Figure 1) consisted of 3 questions regarding the utilization of communication skills, specifically related to COVID-19 pandemic and burnout/work satisfaction. Questions 1 and 2 used an ordinal scale, and the third question was open ended to guide future training. Data was collected in a RedCap database. Proportions were estimated along with 95% confidence intervals (CIs). Statistical analyses were performed using R Statistical Software (version 4.1.2).

Survey questions used to assess effectiveness of communication in healthcare training on reducing burnout during COVID-19.
Results
Of 98 surveys sent out, a total of 33 participants completed the survey (33.7%, 95% CI: 25.1%-43.5%). Survey responses are displayed in Table 1. Of the 33 respondents, 26 (78.8%, 95% CI: 62.2%-89.3%) rated their ability to communicate with patients during the COVID-19 pandemic as somewhat above average, or far above average. Twenty-four respondents (72.7%, 95% CI: 55.8%-84.9%) agreed or strongly agreed that the tools learned in the communication modules helped with work satisfaction and decreased burnout. When asked how we could assist in continuing to improve your communication skills (Ex. More training/classes, more practice/simulation time, video examples, email remainders, etc.), six participants responded and answers included: “more of all of the above”, “email reminders with written training materials based on content covered in the training;” “more practice/simulation time as well as training;” “training/classes - always something new to learn;” “video examples;” “real life stories;” “virtual visit skills- how to best navigate a virtual consult.”
Summary of Survey Responses.
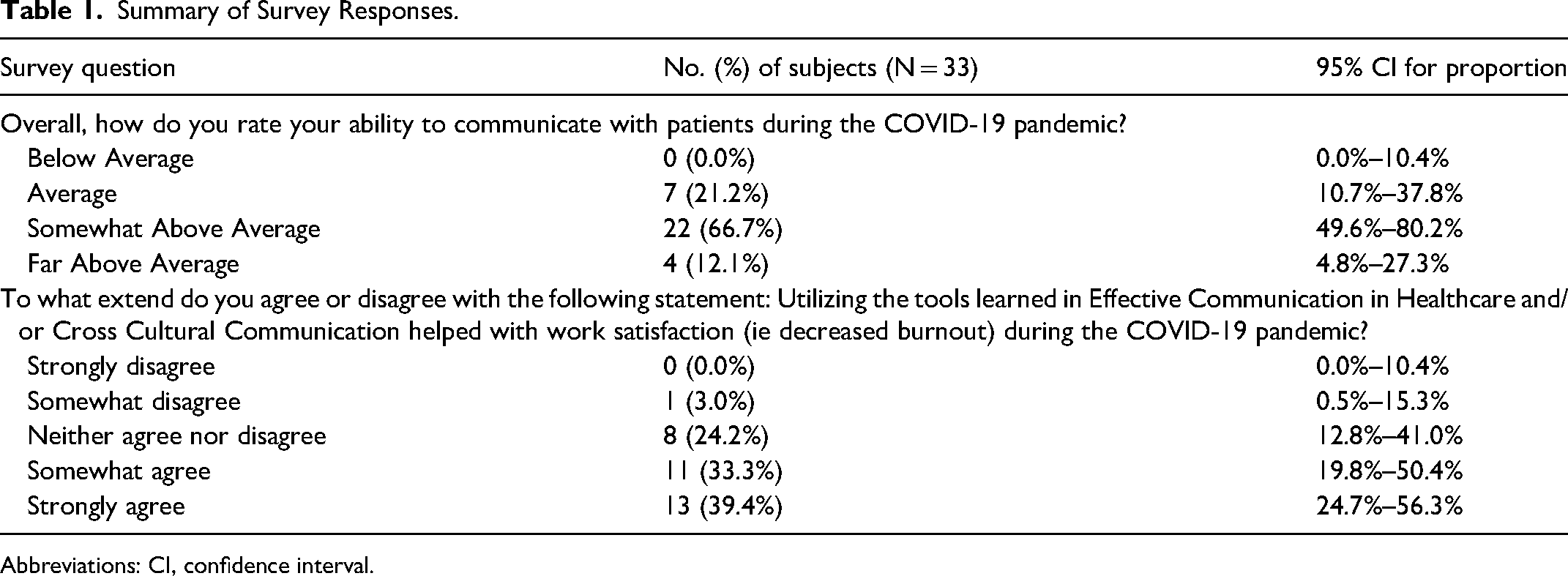
Abbreviations: CI, confidence interval.
Discussion
Globally, the COVID-19 pandemic may represent a greater problem for health care providers as they face challenges imposed by the pandemic both in the workplace and at home. Fortunately, our survey has demonstrated that formal communication training can not only help improve communication skills, but also improve work satisfaction. There are reports documenting the psychiatric toll of the current pandemic on health care providers, many of these studies from locations which were first impacted by COVID-19. In Tunisia, younger health care providers reported greater symptoms of stress as compared to their older colleagues. Similarly, female providers reported more stress than their male counterparts. 9 In Wuhan, China, where cases of COVID-19 were first reported, physicians and nurses directly treating COVID positive patients reported fewer symptoms of burnout when compared to providers who were not on the front line of care. 10 The investigators suggested that those who were directly treating infected patients felt a greater sense of control of their current situation, possibly believing that they were better able to manage risk of self-infection and subsequent infection of a family member, than those who were not directly treating COVID positive patients. 10 The long-term effects of the COVID-19 pandemic on health care providers are not known; however, data from other crises in the recent past may be instructive. Registry data from the public as well as rescue/recovery crew exposed to the trauma at the World Trade Center on September 11, 2001, has reported increased prevalence of post-traumatic stress syndrome and depression in this cohort when compared to a non-exposed population, even decades after the event. 4
In a pandemic situation, one of the greatest tools of the health care provider is the ability to offer correct and timely information to the patient. This ability was tested during the early portions of the COVID-19 pandemic given the multiple venues of incorrect information easily available to the patient. 11 Therefore, any tool that facilitates a provider to communicate effectively and counter disinformation may offer an improved feeling of control in the workplace. This sense of control is a major driver of provider engagement and helps avoid provider burnout. 10 Using formal communication tools helps provide a structured approach to challenging conversations with patients and their families. Mayo Clinic advocates the use of one such tool, the mnemonic PEARLS, to build relationships and improve communication. 12 This tool is particularly useful in the current climate as providers seek to convey important clinical instruction to patients regarding COVID-19 when these patients may already be exposed to conflicting information. In such cases, PEARLS is used to build trust and foster a meaningful clinical relationship between provider and patient and ultimately may improve compliance with proposed treatment recommendations. Similarly, the SPIKES technique is another communication tool that is shown to be helpful. 13 While SPIKES was developed to share diagnoses with oncology patients, it is a communication tool capable of broad application. For instance, SPIKES could prove effective in sharing a stigmatized medical diagnosis, such as a positive test result for COVID-19. The diagnosis may evoke a strong emotional response from the patient and this tool can help providers navigate such barriers and allow the delivery of important clinical information.
Throughout the world, provider burn-out and the need to improve work-life balance are recognized as critical issues in modern medicine. In 2014, Shanafelt and colleagues surveyed 6880 US physicians and reported that 54% met the criteria for burn-out, which is an increase from their survey in 2011 when only 46% of physicians reported similar symptoms.8,14
Limitations
Given that only 34% of participants completed the survey, our study is inherently limited due to response rate bias. Responders may represent a biased subset who value the impact of these tools in the clinical workplace. However, the response rate obtained is comparable to response rates of other research studies using online questionnaires. 15 We did not assess participants’ current level of burnout or how communication skills impacted their burnout prior to their module training. To keep the survey short, we did not ask which tools were most effective in reducing burnout and we did not use a validated burnout instrument. Future studies should use validated burnout instruments before and after communication skill training to best elucidate the effectiveness of training. Based on the respondent's comments, additional simulations and email reminders with written training materials may help with retention of skills learned. Finally, our surveys were sent to participants who had completed training less than seven months prior to the pandemic. Thus, we are unable to comment on the sustainability of these tools specific to the unique challenges of the current pandemic.
Conclusions
Based on our results, the communication tools utilized at Mayo Clinic are helpful in increasing work satisfaction by improving communication with patients during the current COVID-19 pandemic. Our survey also suggested that those who used these communication tools may experience less symptoms of burnout. This finding is consistent with other studies which demonstrated that health care providers who had completed communication skills training had long-term improvement in communication as perceived by the patient's family. 16 Boissy and colleagues also showed that the training improved patient satisfaction and reduced burnout. 17
Our study evaluated the effect of recent communication skills training and its effect on reducing burnout in the setting of the COVID-19 pandemic. Techniques that emphasize empathy, effective listening, trust-building, and how to convey difficult information are critical elements to help both the patient and the provider as they both navigate the challenges imposed by the current health crisis.
Footnotes
Abbreviations
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Authors’ Contributions
LS collected and analyzed the surveys. All authors were major contributors in writing the manuscript and have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article