
Abstract
Introduction
The COVID-19 pandemic led to a major transition for patients from routine ambulatory-care-based in-person primary care visits to telehealth visits to manage chronic diseases. However, it remains unclear the extent to which individuals access telehealth services and whether such utilization varies along neighborhood characteristics, especially among racial minorities. This study aims to examine the association of outpatient telehealth utilization with sociodemographic, clinical, and neighborhood characteristics among adults with ambulatory care sensitive conditions (ACSCs) during the COVID-19 pandemic.
Methods
We included adults treated for an ACSC between March 5, 2020, and December 31, 2020, at a single ambulatory-care-based healthcare system, which serves a large population of low-income patients in the South region of the United States (i.e., Memphis, TN, Metropolitan Statistical Area). Telehealth utilization was defined by outpatient procedural codes and providers’ notes on the type of visits. Generalized linear mixed models were used to examine the association of sociodemographic, clinical, and neighborhood factors with telehealth utilization in the overall cohort and the racial subpopulations.
Results
Among the 13,962 adults with ACSCs, 8583 (62.5%) used outpatient telehealth services. Patients who were older, female, with mental disorders, and who had more comorbidities had higher rates of telehealth services (p < .05). Controlling for covariates, we observed 75.2% and 23.1% increased use of telehealth services among Hispanics and other race groups, respectively, compared to Whites. Patients who commuted more than 30 minutes to health facilities were slightly less likely to use telehealth services [OR: 0.994 (0.991,0.998)]. Racial minorities (Blacks and Hispanics) with mental disorders were more likely to use telehealth service when compared to Whites.
Discussion
We found that among patients being treated for ACSCs, the use of telehealth services was highly prevalent in Hispanic patients in general and were more pronounced among both Hispanics and Black patients who have mental disorders.
Introduction
Even before the COVID-19 pandemic emerged, many healthcare systems had adopted telehealth for chronic disease management. Indeed, several studies found that telehealth not only was found to increase timely access to health services but was associated with better health outcomes, reduced hospitalizations, and reduced mortality for community dwelling adults with chronic health conditions.1–4 A longstanding challenge with the implementation of telehealth has been related to reimbursement to providers and the extent to which such rules and laws vary across state lines.5,6 However, due to the outbreak of COVID-19, coverage for telehealth services was extended by the Centers for Medicare and Medicaid Services (CMS). 7 Despite the known benefits of telehealth for individuals with chronic health conditions, such services were found to be limited for vulnerable low-income patients and racial minorities with limited digital access and health literacy.7–9 In fact, such inequalities in both access and use of services has existed across several demographic and socioeconomic factors. 7 Due to the extended access to and increased implementation of telehealth services during COVID-19, it is unclear if utilization varies along particular characteristics, especially among racial subpopulations. This lack of knowledge is especially concerning since Blacks and people residing in low-income areas were disproportionately affected by COVID-19 and were more likely to be hospitalized.10–12
Ambulatory care sensitive conditions (ACSCs) are chronic health conditions that can be disabling and include the management of symptoms (e.g., diabetes mellitus) for which access to timely, high quality primary care services are imperative to prevent emergency department visits or hospitalizations. 13 Thus, telehealth interventions are especially applicable for patients as a technique to prevent acute aggravation of symptoms related to the conditions of ACSCs. 13 Little is known on the extent of adults with ACSCs who utilized telehealth services during the COVID-19 pandemic and the extent to which it varied along particular racial subpopulations and other sociodemographic and clinical characteristics.
Furthermore, scant information exists on the extent to which factors other than individual patient-level factors were associated with telehealth services. For instance, a series of neighborhood-level factors could also be correlated with telehealth service utilization, thereby explaining some of the differences as well, especially those that relate to economic and access variables.9,14,15 This lack of information is particularly troubling because both physical and social characteristics of neighborhoods affect one's health status. 16 Also, a recent study found that even after adjusting for socioeconomic and county-level factors, COVID-19 infection and death rates were higher in whole county primary care health professional shortage areas (HPSAs) compared with non-whole county primary care HPSAs, suggesting that HPSAs may experience other unmeasured medical and economic producers of vulnerability. 17 To address these knowledge gaps, we conducted a retrospective cohort study of ACSC patients who utilized telehealth services from a large, single ambulatory-care-based healthcare system during the first 7 months of the COVID-19 pandemic. We investigated potential disparities in telehealth use according to demographic factors, especially along racial subpopulations, clinical factors, and neighborhood-level factors.
Methods
Study Setting and Population
This retrospective cohort study used electronic medical records data from seven ambulatory-care-based federally qualified health centers (FQHCs). These FQHCs serve a large population of low-income and racially, ethnically, and socioeconomically diverse patients in the Memphis, TN, Metropolitan Statistical Area (MSA), a large, urban metropolitan area in the Southern region of the United States. The study included adults (≥18 years) with ASCSs. Patients with ASCSs were defined using the primary diagnoses of any following conditions: diabetes, hypertension, chronic heart failure, coronary artery disease, chronic obstructive pulmonary disease, and asthma. 18 All patients were receiving healthcare for their respective ASCSs diagnoses.
We included adult outpatients treated for an ASCS from March 5, 2020, through December 31, 2020, to assess the association of sociodemographic and neighborhood-level factors with the telehealth service utilization rate during the first year of the COVID-19 pandemic. The starting date was selected based on the date of the first COVID-19 case in the state. We excluded those individuals with missing information on race and other patient-level factors. The information was missing for less than 5% of the total sample. We also excluded census tracks that were outside of Memphis MSA.
Data Sources
Electronic medical records from FQHCs were obtained from the Tennessee Population Health Data Network (TN-POPnet). TN-POPnet stores information about all aspects of the care provided to the individuals served by the TN-POPnet participating health system, including patient demographics, clinical characteristics, and medical encounters with diagnosis and procedure codes. 19 Patient residence addresses were geocoded at the census track level and linked with neighborhood-level factors obtained from the National Historical Geographic information System (NHGIS). 20
Variable Measures
The outcome variable, outpatient telehealth service utilization, was defined based on published literature.7,21,22 The telehealth visits were billable and were defined by outpatient Current Procedural Terminology (CPT)/Healthcare Common Procedural Coding System (HCPCS) procedural codes. The outpatient telehealth visits included virtual check-in encounter codes (G2010, G2012), telephone evaluation and management visit codes (99441, 99443), FQHC distant site telehealth code (G2025), and if the reason for visit was recorded as a telehealth visit.
Individual patient-level factors may be associated with telehealth service utilization and the following baseline patient characteristics were captured at the time of each telehealth visit utilization. Patient race and ethnicity was classified into four categories: (1) Hispanic, (2) Non-Hispanic Black, (3) Non-Hispanic White, and (4) Other race. Other race category predominantly included other race (95%) followed by Asian, American Indian, Native Hawaiian or Pacific Islander, and Vietnamese. Patient age (in years) and gender (male, female) were included. Clinical factors included the presence of a mental disorder (yes/no), and the Charlson comorbidity index (CCI). Mental health disorders included depression, anxiety (ICD-10 codes: F32.3, F33.3, F43.21, F32.9, F41.9, F32.9, F33.9, F43.21, F32.9), bipolar disorder, schizophrenia, or other psychotic disorders (F20.89, F22, F32.3, F33.3, F06.2, F06.0, F30.10, F31.10, F31.30, F31.60, F31.9, F39). The CCI is a longstanding assessment tool of a patient's unique clinical situation that has been found to predict long-term mortality in different clinical populations with excellent reliability, concurrent validity, sensitivity, and predictive validity. 23
The neighborhood-level characteristics were assessed at zip code and census track levels by linking patient residence zip codes and addresses with zip code- and census track-level neighborhood factors, respectively. These factors included residence in a low-income area or a HPSA measured at the zip code level. Patient residence ZIP codes were linked to the CMS database of HPSA ZIP codes to identify patients residing in low-income areas or HPSAs. 24 These are regions with a lack of primary care providers based on need for care. 17 Census track level factors included income defined as percent of population in the census track below 100% of the Federal Poverty Level. The percent population below the federally designated poverty level was classified along the three categories: (1) less than 20%, (2) 20% to 30%, and (3) more than 30%. The other census track level neighborhood-level characteristics that are indicators of socioeconomic status included the percentage of the population who commute more than 30 minutes to a health facility (an indicator of geographic access), percentage of the population who had at least a college education, the percentage who rented a living place, the vacancy rate (i.e., the percentages of all available units in a rental property like an apartment complex that is unoccupied, with higher rates being indicative of lower income in the area), and the percentage of households without internet access. The study was reviewed and approved by the University of Tennessee Health Science Center Institutional Review Board.
Statistical Analyses
Descriptive statistics were conducted using Mann–Whitney U-test for continuous variables given the non-normal distributions, and Chi-squared tests were used for categorical variables. Generalized linear mixed models (GLMMs) with logit link accounting for the nested structure of the data were used to examine the factors associated with telehealth service utilization in the overall sample. Additionally, we ran GLMMs in subpopulations by race. All statistical analyses were performed using SAS v9.4 (SAS Institute, Cary, NC, USA). A two-sided p-value <.05 was considered significant.
Results
There was a total of 13,962 adult patients with ACSCs (mean age 52.3 years, standard deviation [SD] 14.6 years; 61.1% female; 82.5% Non-Hispanic, Black). Of the 13,962 adults with ACSCs, 8583 (62.5%) utilized outpatient telehealth services from March 5, 2020, through December 31, 2020. Twelve percent of the patients with ACSCs had a diagnosed mental disorder. For the neighborhood-level characteristics, 87.2% of the overall sample of ACSCs patients lived in a low-income area or HPSA and 48% of them lived in neighborhoods where more than 30% of the population was below poverty. Twenty nine percent lived in neighborhoods where individuals commute more than 30 minutes to health facilities (Table 1).
Patient- and Neighborhood-Level Characteristics in Adults with Ambulatory Sensitive Conditions Who Used of Telehealth Services.

Abbreviations: SD = standard deviation; HPSA = health professional shortage areas; CCI = Charlson comorbidity index.
The mean age of the telehealth utilizers was significantly greater than that of the non-utilizers (53.8 [SD 13.3] vs 49.9 (16.2), p < .001). The utilization of telehealth also differed by race, with the prevalence of telehealth utilization higher among those who were Hispanic and those in the “other” category (i.e., those who were not White, non-Hispanic and Black). The prevalence of telehealth utilization was significantly higher among female patients, those with mental disorders, those with greater comorbidities, commuters who were less than 30 minutes to health facilities, and those living in neighborhoods with a lower vacancy rate (Table 1).
Table 2 shows the adjusted odds ratios (aORs) for telehealth utilization for the main analysis. In the main analysis, older age was significantly associated with increased odds of telehealth utilization. More specifically, each increment in age was associated with a 2% increase in telehealth utilization (aOR = 1.02, 95% CI 1.017–1.021). Male patients were significantly less likely to use telehealth services than were female patients (aOR = 0.88, 95% CI 0.82–0.94). As compared to White, non-Hispanic patients, those who were Hispanic (aOR = 1.75, 95% CI 1.29–2.39) and from other race categories not including Blacks and Hispanics (aOR = 1.23, 95% CI 1.02–1.48) were both significantly more likely to use telehealth services. Patients with a mental disorder were 42% more likely to have used telehealth services compared to those without such a disorder (aOR = 1.42. 95% CI 1.27–1.59). Patient comorbidity was associated with increased telehealth service utilization. With reference to neighborhood-level characteristics, one variable was associated with telehealth utilization. Patients who lived in neighborhoods with more than 30 minutes of commute to health facilities were less likely to use telehealth (aOR = 0.99, 95% CI 0.98–0.99).
Associations Between the Use of Telehealth Services and Patient- and Neighborhood-Level Characteristics in the Overall Population.

Abbreviations: CI = confidence interval; Ref. = Reference; HPSA = health professional shortage areas; CCI = Charlson comorbidity index. Significance: *p-value < .05.
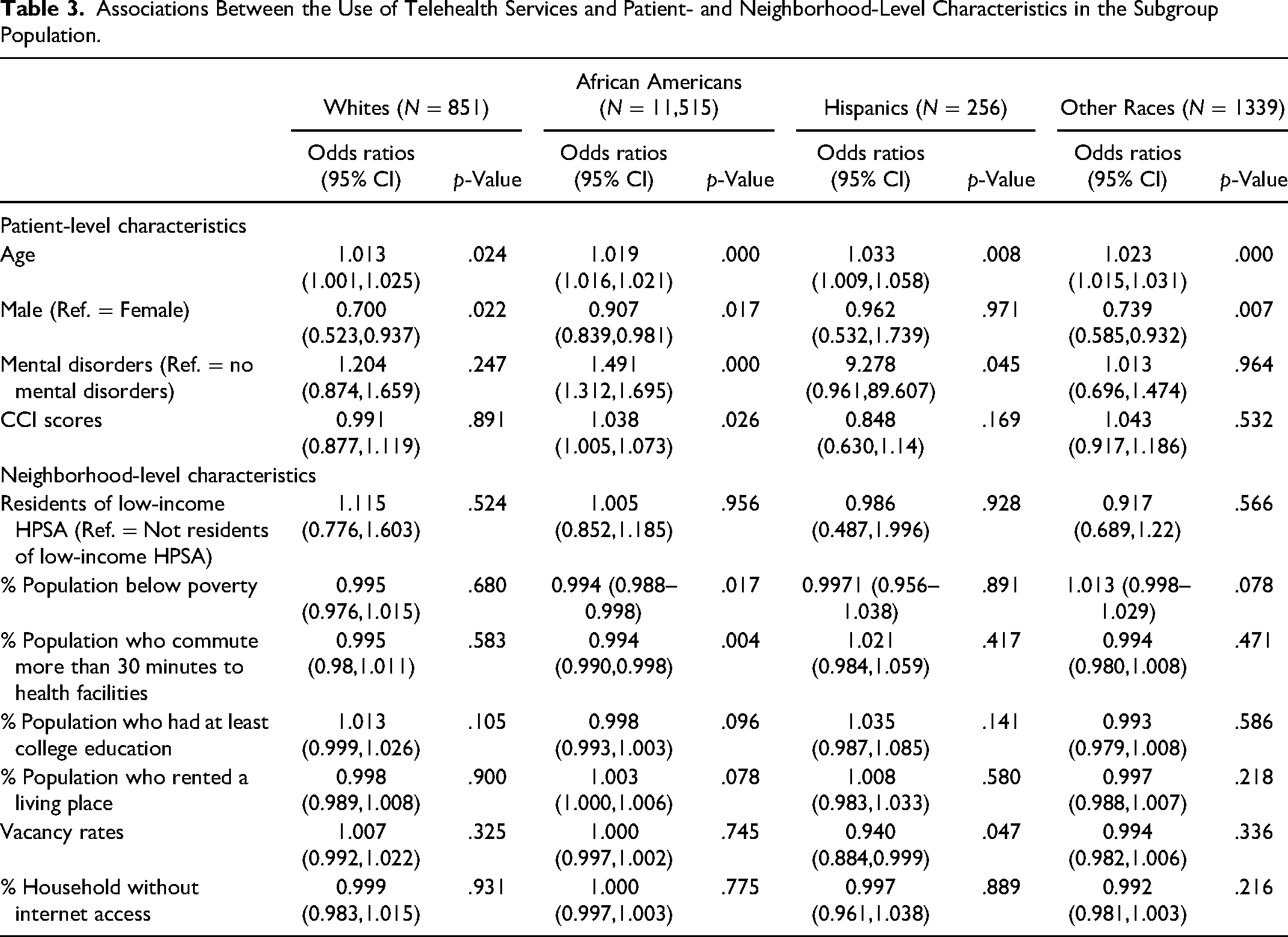
Table 3 displays subgroup analyses by race (White non-Hispanics, Black non-Hispanics, Hispanics, and other races). Older age was associated with increased telehealth utilization across each of the race categories. As compared to female patients, male patients were less likely to use telehealth services among patients who were White, Black, and the other categories (e.g., Asian Americans). Patients who have a mental disorder were associated with increased odds of telehealth utilization among both Blacks and Hispanics. Greater patient comorbidity was associated with increased use of telehealth services among Black patients. An inverse association was found for those who commuted greater than 30 minutes to health facilities and telehealth service utilization in Black patients.
Associations Between the Use of Telehealth Services and Patient- and Neighborhood-Level Characteristics in the Subgroup Population.
Discussion
It is well known that the COVID-19 pandemic not only substantially increased the use of telehealth services, but also caused an extraordinary situation for healthcare.9,25 COVID-19 disproportionately affected individuals with multiple physical comorbidities, obesity, advanced age, and ethnic minorities, 9 all of which represent clinical and sociodemographic characteristics that were found to be associated with worse COVID-19 health outcomes and have been found to be associated with an increased use of health services. Even though telehealth services significantly increased since the inception of COVID-19, it was unclear the extent to which clinical and sociodemographic factors were associated with individuals’ access of telehealth services, especially those with multiple comorbidities and especially among racial subpopulations. In fact, the few studies have reported inconclusive findings. For instance, prior to the COVID-19 pandemic, studies tended to report that Hispanic and Black patients were less likely to use telehealth services as compared to White patients, whereas other studies reported that there were no racial and ethnic disparities in telehealth service use.26–28
Systematic racism could have been associated with racial and ethnic minorities being more likely to suffer from COVID-19 and therefore being at greatest need for telehealth services.29,30 Thus, telehealth services could be extremely beneficial for people of color who had poor health outcomes from COVID-19 to not only to receive medical advice about symptoms related to the virus, but also to manage chronic physical comorbidities because they are more likely to have such conditions (e.g., diabetes) that not only require ongoing medical care, but may lead them to telehealth services.29,31 However, compounded with this challenge is that people of color with both access to and comfort with technology is lower than White individuals. 32 Most of the previous studies have failed to consider community and neighborhood characteristics as covariates. These socioeconomic and community level factors are key variables of social determinants of health and can serve as key covariates in the generalized linear models. To fill an important void in the literature, we employed variables that gauge levels of poverty, percent of population who had at least a college education, and a key indicator of access to care (i.e., percent of population who commute more than 30 minutes to the nearest health facility).
During the first 9 months of the COVID-19 pandemic, we found that 62.5% patients with ACSCs utilized outpatient telehealth services. Our findings underscored several disparities in telehealth service utilization. We found differences by gender, age, race and ethnicity, presence of mental disorders, comorbidity, as well as drive time from patients’ place of residence to the closest health facility. More specifically, GLMMs found that patients who were Hispanic and from other race groups (not including Black patients) were significantly more likely to use telehealth services as compared to White patients, findings that were consistent with a recent secondary analysis of self-report data from national, probability-based online panel of adults (18 or older) living in US households. 29 That is, Campos-Castillo and Anthony (2020) found that as compared to White respondents, Hispanic and those from other race groups (excluding Black respondents) reported using telehealth services more often. This finding from our study was also congruent with a retrospective cohort study of older members of Kaiser Permanente Southern California system. Qian and colleagues (2021), found that those in the Hispanic group had the largest increase in telehealth utilization in response to the COVID-19 pandemic. 33 However, once multivariate analyses were applied to their dataset, only Black respondents were more likely than Whites to report using telehealth services. 29 Another study from a non-profit healthcare system in seven states in the West and Southwest of the US, found that compared to White patients, Hispanic/Latino patients were significantly less likely to use telehealth services before and after COVID-19 diagnosis. 34
Other recent research found that differences between Black and non-Black patients in terms of primary care appointment completion rates narrowed significantly due to the increased use of telehealth services. 35 However, in contrast to these findings, Chunara and colleagues (2021), who conducted a study from a large academic healthcare system in New York City, found that after controlling for individual and community level attributes of telehealth patients, the Black patients were significantly less likely to access care through telemedicine compared to White patients. 36 Similarly, Friedman et al. (2022) from an urban tertiary hospital in the Midwest, found that Black race and participants of other races were less likely to use telehealth compared to Whites. 37 Thus, the current state of the literature has found mixed results on racial and ethnic differences in telehealth service utilization.
Even though our multivariate analyses found that Black patients were comparable to white patients in terms of telehealth utilization, on the other hand, we found that two specific racial minorities (Blacks and Hispanics) with mental disorders were more likely to use telehealth services than their white counterparts. To our knowledge, there have been no previous studies that have specifically examined how the interplay between mental illness and racial minorities is associated with increased telehealth use. However, recent research did report racial/ethnic disparities in outpatient visits for mental health and/or substance use disorders during the COVID surge and partial re-opening in Massachusetts. More specifically Yang (2020) found that Hispanics and non-Hispanic Blacks reported decreases in visits for mental health and/or substance use disorders. 38 Future research should further investigate these relationships, since telehealth services play an important role in access to mental health services, especially in terms of racial minorities. 39 This need is particularly important because there is a “digital divide” with reference to access to computer and home broadband availability for Black and Hispanic adults.38,40 In fact during the pandemic, Black and Southern residents were less likely to use telehealth due to lack of broadband access. 41
Consistent with studies both prior to and during the COVID-19 pandemic, 25 we found that in both the main and subgroup analyses, advanced age was correlated with increased telehealth service use. This is consistent with a longstanding body of research that has found that telehealth services offer an important role in managing symptoms of chronic health conditions for older individuals. 42 In both the main and subgroup analyses, higher CCI scores was associated with increased telehealth utilization rates, with Black patients having higher rates than their White counterparts. A previous study found that Black citizens tend to have higher rates of disabling chronic health conditions (e.g., diabetes) than their White counterparts. 43 Thus, our findings were encouraging that Black patients who had more comorbidities had greater odds of using telehealth services.
The study has some limitations. First, EMR data were used from practices serving predominantly African American populations in the Memphis MSA, and the results may not be generalizable to larger racially diverse populations. Second, it is an observational study, and the analyses could only identify the association of demographic, clinical, and neighborhood-level factors with the outpatient telehealth use and not causality. Third, this study assesses the telehealth service utilization rates during the first year of the COVID-19 pandemic. A longer study period would be essential to examine changes in the rates of outpatient telehealth use after the onset of COVID-19 pandemic. Fourth, our study was limited to low-income zip codes that surrounded the Memphis MSA. Therefore, it is unclear how our findings can be generalizable to other regions, especially those areas with residents who have more income or who reside in suburban and/or rural areas.
Conclusion
In summary, we found that in a large cohort of patients being treated for ACSCs, the use of telehealth services was highly prevalent in Hispanic patients in general and were more pronounced among both Hispanics and Black patients who have mental disorders. Our findings may be applicable for people of color with ASCSs, especially those who experience mental disorders who also need to access timely services to manage symptoms related to their comorbid conditions. Findings from our study support the notion that telehealth can be leveraged to increase access to care among Blacks and Hispanics that may have typically faced barriers to in-person care. Our study also contributes to the existing body of literature by suggesting the importance of the identification of major social determinants of health as key indicators to help explain racial differences in telehealth services by patients with ACSCs who reside in low-income areas. 44 We employed access to care variables, as well as sociodemographic and socioeconomic factors as covariates to adjust for the racial differences in telehealth services. Over the past two and one-half years the COVID-19 pandemic has brought challenges to the US healthcare systems. Even though many US residents have been vaccinated, cases have been on the rise in the US. Even though symptoms are milder for those who have been diagnosed recently with COVID-19, adverse health outcomes could continue to exacerbate for those with chronic health conditions who experience symptoms from COVID-19 and many of such individuals may be confined to their places of residence and have challenges to come to their physician. In fact, our findings along with other recent studies found that telehealth services will continue to play an important role in the management of not only COVID-19 symptoms, but also for the management of chronic health conditions and acute and chronic mental health issues, conditions that require high rates of health service utilization.
Supplemental Material
sj-docx-1-hme-10.1177_23333928231154334 - Supplemental material for Racial and Socioeconomic Characteristics Associated with the use of Telehealth Services Among Adults With Ambulatory Sensitive Conditions
Supplemental material, sj-docx-1-hme-10.1177_23333928231154334 for Racial and Socioeconomic Characteristics Associated with the use of Telehealth Services Among Adults With Ambulatory Sensitive Conditions by Neale R. Chumbler, Ming Chen, Austin Harrison and Satya Surbhi in Health Services Research and Managerial Epidemiology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Tennessee Health Science Center, (grant number University of Tennessee-funded 2020 Collaborative).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.