
Abstract
Background
Childhood stunting has a long-term impact on cognitive development and overall well-being. Understanding varying stunting profiles is crucial for targeted interventions and effective policy-making. Therefore, our study aimed to identify the determinants and stunting risk profiles among 2-year-old children in Ethiopia.
Methods and materials
A cross-sectional study was conducted on 395 mother–child pairs attending selected public health centers for growth monitoring and promotion under 5 outpatient departments and immunization services. The data were collected by face-to-face interviews, with the anthropometric data collected using the procedure stipulated by the World Health Organization. The data were entered using Epi Data version 4.6 and exported to STATA 16 and Jamovi version 2.3.28 for analysis. Bayesian logistic regression analysis was conducted to identify potential factors of stunting. Likewise, lifecycle assessment analysis (LCA) was used to examine the heterogeneity of the magnitude of stunting.
Results
The overall prevalence of stunting in children under 24 months was 47.34% (95% confidence interval (CI): 42.44-52.29%). The LCA identified 3 distinct risk profiles. The first profile is
Conclusion
Our study identified 3 distinct risk profiles for stunting in young children. A substantial amount (almost half) is in the high-risk category, where stunting is far more common. The identification of stunting profiles necessitates considering heterogeneity in risk factors in interventions. Healthcare practitioners should screen, provide nutrition counseling, and promote breastfeeding. Policymakers should strengthen social safety nets and support primary education.
Introduction
Stunting, defined as low height-for-age, is a significant public health concern in children under 2 years old. 1 It is an indicator of developmental delays, poor child health, and chronic malnutrition, affecting children's recovery, vulnerability to long-term illnesses, missed learning opportunities, and school performance.2,3 It is estimated to be a significant contributor to around 45% of children's deaths. 4 Despite the global prevalence decreasing from 32.4% in 2000 to 22.3% in 2022, 5 this reduction is insufficient to meet the World Health Organization (WHO)'s Global Nutrition Targets 2025. 4 In 2022, Africa had the highest number of stunted children, accounting for 43%. 6 Ethiopia's stunting rate is pervasive, with an overall rate of 35.1% among children under 2. 7 This highlights the urgency for effective strategies to address childhood stunting.
The Ethiopian government began implementing growth monitoring and promotion (GMP) in the 1990s as part of its attempts to tackle child malnutrition.8–10 GMP is a nutritional intervention that measures, plots, and interprets child growth regularly to counsel and take action when abnormalities are detected, empowering mothers to improve their children's nutritional status. 11 However, despite this intervention, the prevalence of stunting remains unacceptably high in the country.12–14 Several studies have identified inadequate dietary intake, maternal nutrition, breastfeeding practices, and frequent infections as significant contributors to stunting in young children15–18 and emphasizing the need to consider heterogeneity and the complex interplay between these factors.19–21
Despite existing research providing valuable insights into the overall prevalence and risk factors of stunting,12–14 there is a need for more nuanced analyses that go beyond broad categorizations to uncover hidden patterns and variations within the stunted population. Studies in India have yielded diverse findings on subgroup analysis.22,23 For instance, a study in Gondar City, Northern Ethiopia identified a strong association between stunting and occupational status of a mother, 15 while another in Rwanda revealed a more significant influence of water and sanitation. 24 Similarly, a study finding from South Africa revealed socio-demographic and infant and young child feeding (IYCF) factors associated with stunting. 20 These contrasting results highlight the need for further research that delves deeper into subgroup variations across Ethiopia to address the knowledge gap. Moreover, subgroup analyses may offer new insights for identifying and targeting specific populations, providing valuable insights into underlying mechanisms and potential interventions. 25 Therefore, our study aimed to identify the determinants of stunting and identifications of stunting profiles among two-year-old children in Ethiopia. The findings would provide insights into childhood stunting and offer targeted interventions, contributing to the development of more effective approaches to combat stunting.
Methods and Materials
Study Design
We used a facility-based cross-sectional study to investigate potential subgroups of stunted children under 2 years old.
Study Area and Period
The study was conducted in the West Guji Zone, Southern Oromia Regional State. Its administrative center is Bule Hora town, which is located at a distance of 467 km from Addis Ababa, the capital city of Ethiopia, on the paved Addis Ababa to Moyale highway. The zone has 9 woredas and 2 town administrations. It has an estimated total population of 1,389,821, of which 681,012 are males, and 708,809 are females. The zone has immense potential due to its coffee cultivation, mineral wealth, and cultural richness and largely focuses on pastoralism or subsistence farming. Its situation contrasts significantly with some of the region's more stable and developed zones. There is 1 teaching hospital, 3 primary hospitals, 42 health centers, and 166 health posts. The total number of pregnant women, as estimated from the total population of West Guji Zone in 2021, was 48,234 (West Guji Zone Health Department HMIS Report, 2022). The study was conducted from May 1 to 30, 2023.
Population, Sample Size Determination, Sampling Technique, and Procedure
Children aged below 24 months, accompanied by their mothers, who were attending 3 randomly selected public health centers for GMP, in 5 outpatient departments and immunization services in West Guji Zone, Southern Ethiopia, were included in our study. To ensure the accuracy and reliability of our data, we excluded mothers who were only visiting the health center while not living permanently in the area. The sample size was determined using the single population proportion formula. Considering the proportion of children short for their age or stunted 37.1%, 13 95% confidence interval, 5% degree of precision, and 10% non-response rate were also considered. The final calculated sample size was 395. To identify factors associated with stunting, the adequacy of the sample size was examined using Epi-info version 7.1. We employed a simple random sampling technique (using the lottery method) to select 3 health centers (Bule Hora Health Center, Finchawa Health Center, and Guangua Health Centre) based on the availability of functional growth monitoring and promotion (GMP), immunization service, and security issues. Thus, to account for variations in the number of clients visiting each health center daily, we estimated the daily attendance based on the previous month's data. The total sample size needed for the study was then divided proportionally among the 3 centers, ensuring that each center had adequate representation. Within each health center, participants were selected using systematic random sampling. This involved randomly selecting a starting point from the daily client list, and then choosing every 2nd children thereafter until the required sample size for that center was attained. This sampling method helped ensure that the participants were selected randomly.
Study Variables and Operational Definitions
Stunting was the dependent variable of the study. In contrast, sociodemographic and economic factors, maternal obstetric and reproductive health-related factors, child health and dietary and feeding practices, water, sanitation and hygiene, and maternal food and nutrition knowledge were the independent variables of the study.
Stunting: A child with a height-for-age Z-score (HAZ) less than minus 2 standard deviations (<−2 SD). 26 Nutrition and food knowledge refer to an individual's understanding of nutrition, including the intellectual ability to remember and recall food- and nutrition-related terminology, specific pieces of information, and facts. 27 A total of 24 items were used to assess the nutrition and food knowledge of mothers, and each correct answer was scored as “1,” while each “I don't know” answer was scored as “0.” The maximum score that was obtained by correctly answering all the knowledge questions was 24, while the minimum was 0. Thus, women who scored ≥70% (out of 24) on the knowledge questions were regarded as having good knowledge, whereas women who scored <70% (out of 24) on the knowledge questions were regarded as having poor knowledge. 28 Food Insecurity Access Scale (HFIAS) was used to estimate the prevalence of food insecurity and assess the various ways in which households may experience food insecurity by collecting data on access to food, frequency of food insecurity, and the severity of its effects. 29 Therefore, when the average HFIAS score is 0 or 1, households are regarded as food secured. When the average HFIAS score is greater than or equal to 2, households are regarded as food insecure. 29
Dietary diversity score: This is the number of food groups consumed by a child aged 6 to 23 months in the last 24 h out of 7 food groups: (a) grains, roots, and tubers; (b) legumes and nuts; (c) dairy products; (d) flesh foods; (e) eggs; (f) vitamin-A-rich fruits and vegetables; and (g) other fruits and vegetables. 30
Minimum dietary diversity 13 : A child aged 6 to 23 months having the minimum diet diversity in the last 24 h consumed at least 4 food groups out of the 7 food groups. Thus, a child with a DDS of less than 4 was classified as having poor dietary diversity, whereas a DDS of greater than 4 was good dietary diversity. 13
Data Collection Instruments, Methods, and Quality Assurance
The data collection tool was constructed by adapting previous peer-reviewed and published articles13,28,31,32 and the United Nations Children's Fund (UNICEF) 2020 framework. 33 Three BSc degree nurses collected the data using a face-to-face interview and were supervised by 2 Master of General Public Health holder health workers. The anthropometric data (height/length) was measured as per the procedure stipulated by the WHO/UNICEF for taking anthropometric using 34 a horizontal wooden length measuring board, without shoes, with the child in a recumbent position on a hard surface and recorded to the nearest 0.1 cm. 35 Data quality was ensured through proper training of data collectors and supervisors, covering study objectives, participant approach, instrument approach, data handling, and time management. The questionnaire was pretested before the actual data collection on 5% of the sample size in Gerba. The collected data were checked for consistency, completeness, and relevance daily during data collection by the supervisors and principal investigator.
Data Processing and Analysis
Data were entered into Epi Data version 4.6, and then exported to STATA 16 for analysis. Descriptive statistics, including percentages, frequencies, mean with standard deviation, and median with interquartile range, were run to describe the data. To identify the associations between independent variables and stunting prevalence in children, we used a Bayesian logistic regression. Random-walk Metropolis–Hastings (RWMH) sampling algorithm was used to obtain samples from the posterior distribution. MCMC iterations = 12,500, burn-in = 2,500, 10,000 samples from the posterior distribution at 500 burn-in terms discarded. We computed posterior medians, odds ratios, and 95% credible intervals with equal tails to appraise the statistical significance of each independent variable's influence on stunting. Furthermore, the accuracy of posterior estimates was assessed based on the Markov chain (MC) error. Nutritional indices (HFA) were determined using the Emergency Nutrition Assessment (ENA) for Standardizing Monitoring and Assessment of Relief and Transition (SMART) 2011 software, and nutritional status was determined concerning age- and sex-specific growth based on the WHO Child Growth Standards. 26 Diagnostic tools, such as a trace plot, density plot, autocorrelation plot, and histogram, were used to assess the convergence of MCMC (Supplementary file 1). The algorithm's convergence is evident in the plots of significant predictors. We used latent class analysis (LCA) to identify unobservable subgroups within a population based on observed variables and run using Jamovi software version 2.3.28.0 for LCA analysis using the SnowRMM module. 36 Key indicators included maternal food and nutrition knowledge, birth intervals, hand washing, maternal education, ANC follow-up, family planning utilization, unsafe drinking water, breast milk, and food insecurity. Meanwhile, sex, age, dietary diversity, early breastfeeding initiation, maternal occupation, hand washing before child feeding, and sanitation facility were taken from previous studies. 23 The optimal number of latent classes was selected using statistical fit indices like the Akaike information criterion, Bayesian information criterion, consistent Akaike information criterion, log-likelihood, entropy, and Elbow plot.37,38 AIC and CAIC penalize complexity models, with lower values indicating better fit, while BIC penalizes models with more parameters for parsimony. Entropy measures group assignments’ certainty, with higher values indicating clear risk separation and lower values indicating potential overlap and uncertainty, with values above 0.80 considered good classification markers. 39 The elbow plot shows the relationship between latent class numbers and fit statistics, with plateauing points indicating diminishing returns and overfitting indicating model complexity.
In our research, Figure 1 displays that in the elbow plot, the CAIC and BIC exhibit a discernible inflection point at 3 classes, signifying that the inclusion of additional classes does not notably enhance the model's goodness of fit. Similarly, Figure 1 indicates that the initial decline in BIC as the number of classes’ increases signifies a substantial improvement in fit, while a marginal upsurge from 3 to 5 implies that a 3-class model is the most easily comprehensible solution. Consequently, as indicated in Table 1, the 3-class model was selected for further examination due to its optimal balance of fit, complexity, and interpretability.
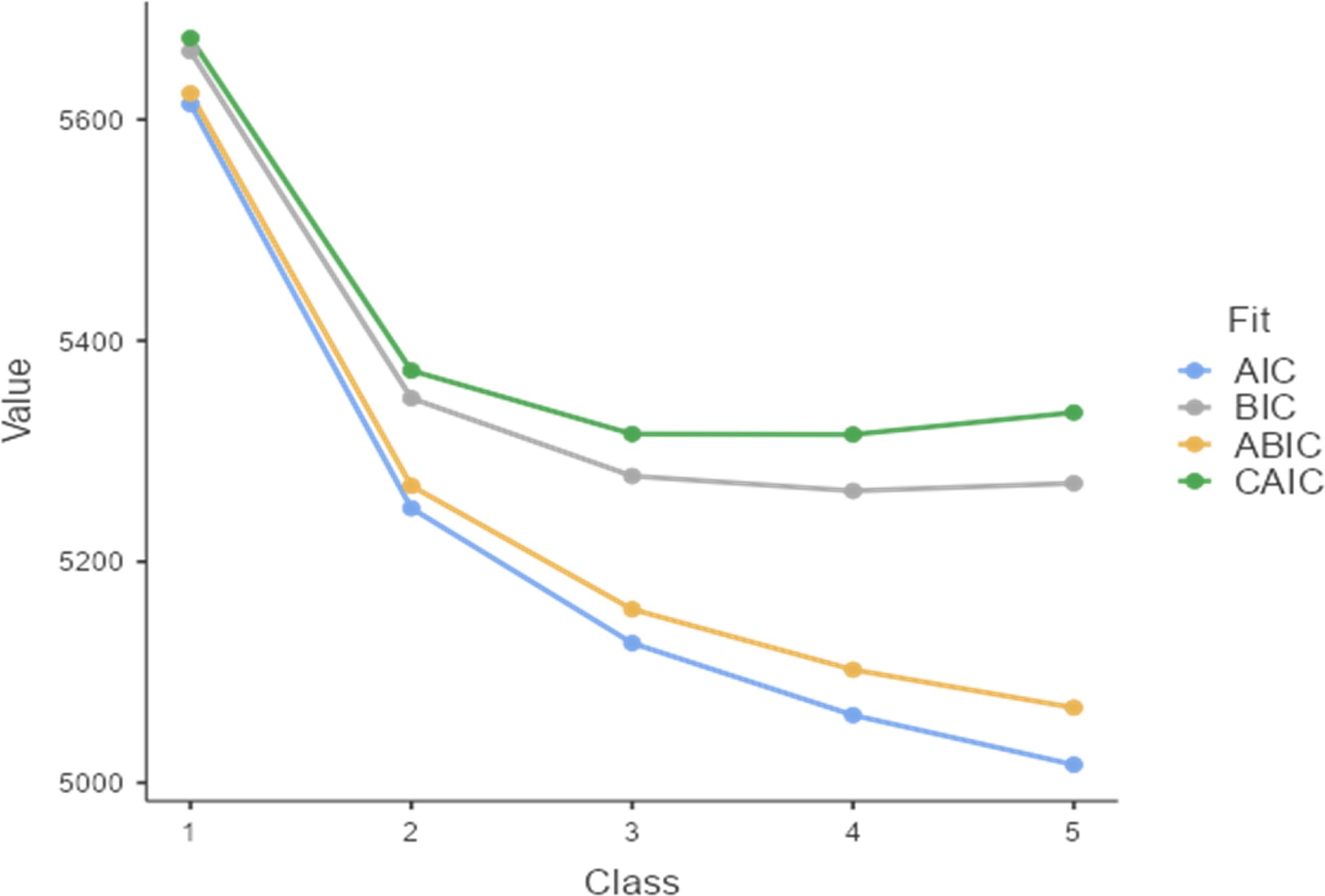
Elbow plot examining model fit statistics to determine the optimal number of latent classes.
Model Comparison for Selecting Optimal Latent Classes.

Results
Sociodemographic and Economic Characteristics of the Respondents
Table 2 shows that mothers’ median (IQR) age was 30 (27-34) years, with the highest number (64.6%) falling from the 26 to 34 age range. In contrast, the children's median (IQR) age was 12 months, ranging from 9 to 18 months, with the highest percentage of 29.6% falling in the 18 and 23-month age range. In terms of the child's gender, 54.9% of them were girls. The majority of mothers, 61.5%, reported moderate food insecurity, while only 15.7% reported having food security.
Socio-Demographic and Economic Characteristics of Mothers with Children Less Than 24 Months of Age in West Guji Zone.

Student, private employee, government employee, merchant; # NGO, merchant, private employee.
Maternal Obstetrics and Reproductive Health and Infant and Young Child Feeding Practices
Table 3 shows that a majority (53.7%) of mothers reported a birth interval of less than 24 months between consecutive births. A total of 349 (88.4%) and 249 (63%) mothers received ANC follow-up and utilized family planning, respectively. Breastfeeding initiation within the first hour of birth remained relatively low (27.6%). Likewise, 61% of children have inadequate dietary intake. Over half (51.4%) of mothers reported a lack of adequate food and nutrition knowledge.
Maternal Obstetrics and Reproductive Health and Infant and Young Child Feeding Characteristics in West Guji Zone, Southern Ethiopia.

Environmental Health-Related Characteristics of the Participants
Table 4 shows a significant proportion of (21.3%) of the study participants relying on unimproved water sources, including rivers, ponds, wells, and unprotected springs. This aligns with the result that a substantial majority (53.4%) did not employ water treatment methods before consumption. Moreover, hand washing practices were also inadequate, with less than half of 48.1% adhering to proper procedures at critical times.
Water, Sanitation, and Hygiene (WASH) Practices Related to the Characteristics of Participants.
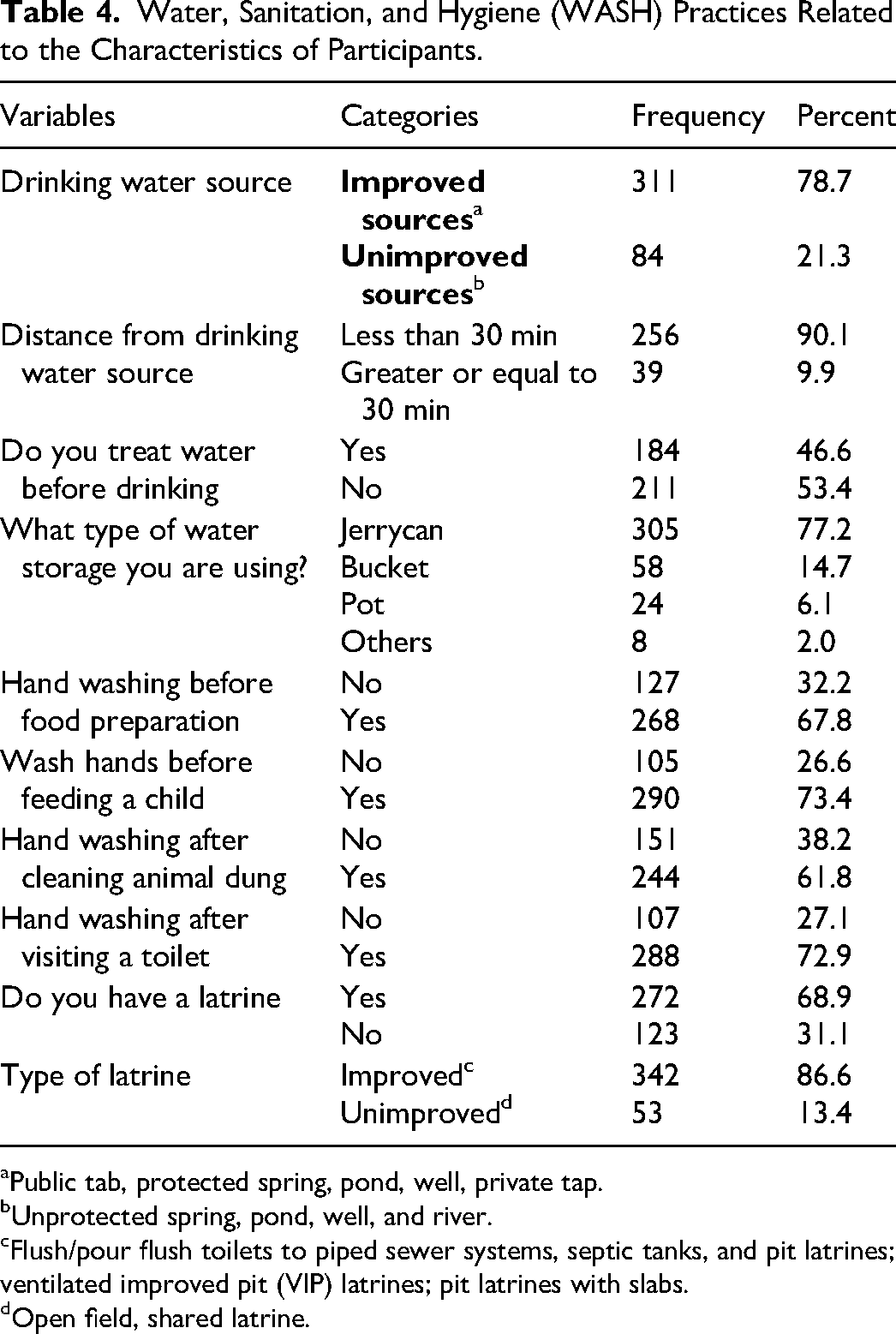
Public tab, protected spring, pond, well, private tap.
Unprotected spring, pond, well, and river.
Flush/pour flush toilets to piped sewer systems, septic tanks, and pit latrines; ventilated improved pit (VIP) latrines; pit latrines with slabs.
Open field, shared latrine.
Bayesian logistic regression analysis of factors linked to stunting in children aged 24 months
As Table 5 shows, a Bayesian binary logistic regression model found that mothers with good knowledge of food and nutrition significantly reduced the odds of having a stunted child (OR = 0.023, 95% CI: 0.004, 0.061). Longer birth intervals (OR = 0.24, 95% CI: 0.105, 0.480) and having primary education (OR = 0.26, 95% CI: 0.099, 0.560) also reduced stunting odds. Additionally, practicing hand washing after toilet use reduced stunting by 88% in children (OR = 0.119, 95% CI: 0.033, 0.299).
Result of Bayesian Logistic Regression Analysis of Stunting Among <24-Month Children.
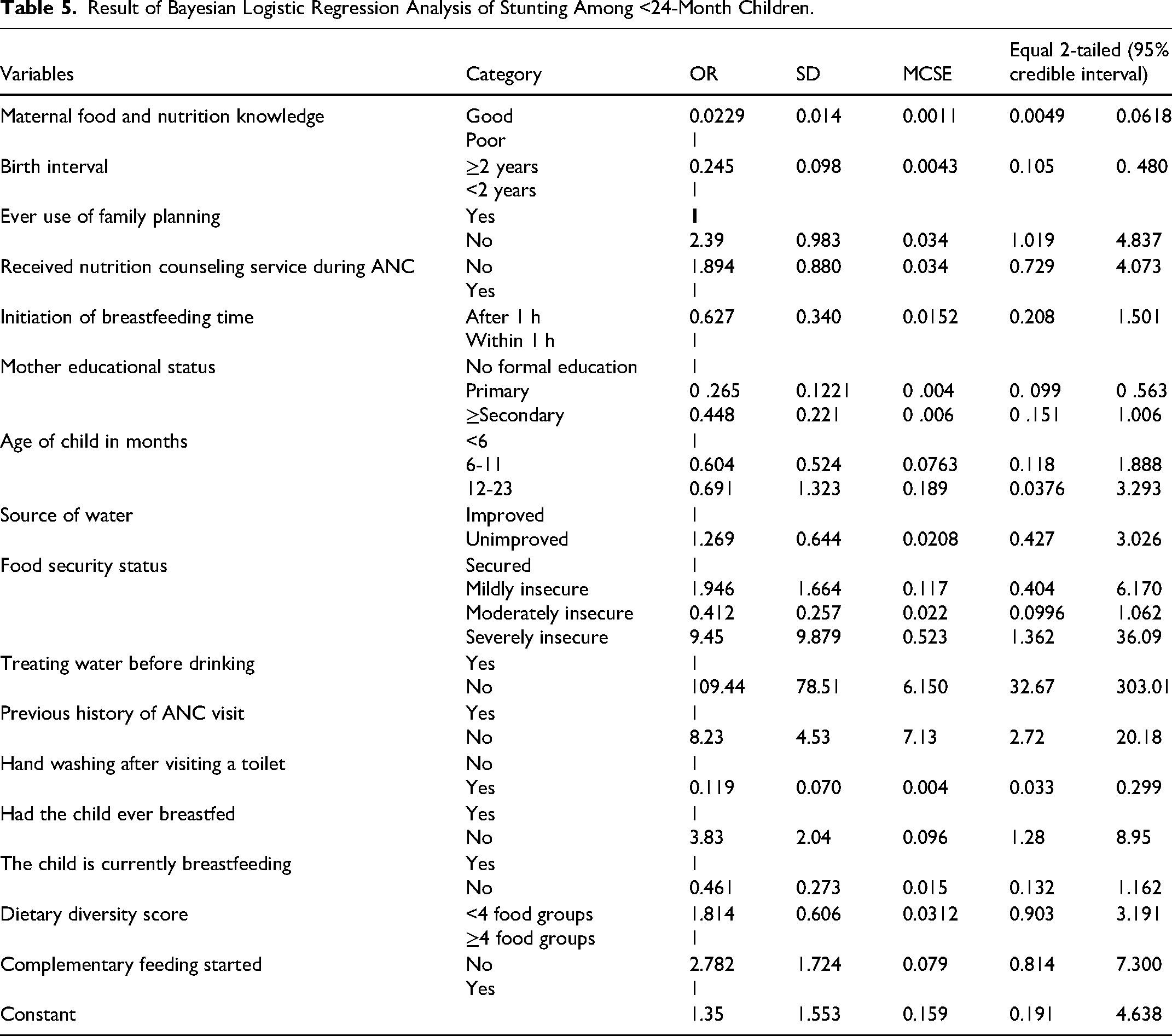
Conversely, children of mothers without ANC history (OR = 8.23, 95% CI: 2.72, 20.18), living in households without safe drinking water (OR = 109.44, 95% CI: 232.67, 303.01), children whose mothers never used family planning methods (OR = 2.39, 95% CI: 1.019, 4.837), and children who never received breast milk (OR = 3.83, 95% CI: 1.28, 8.95) have a higher risk of stunting. Additionally, severe food insecurity in the household (OR = 9.45, 95% CI: 1.367, 36.09) also increases the risk of stunting.
Categorization of Child Stunting Prevalence and Heterogeneity in Risk Factors
The overall prevalence of stunting in children aged 24 months was 47.34% (95% CI: 42.44%, 52.29%). However, our LCA identified 3 distinct subgroups of children under <2 years old with heterogeneity or varying risk profiles for stunting. Following the identification of latent classes, children were categorized into 3 classes based on their posterior probabilities of belonging to each category and subsequently analyzed and outlined using the conditional item-response probabilities. Table 6 shows the conditional probabilities of each latent class and the latent class prevalence. The classes differed in terms of the underlying factors that contributed to their risk of stunting. Each latent class is explained below according to its attributes.
Characteristics of a 3-Group Latent Class Analysis Based on the Estimated Probabilities of Each Risk Factor Within Each Latent Class.

Class 1: Low Risk with High Awareness and Practice of Hygiene and Nutrition
This class represents the smallest proportion of 23.8% of the children and likely faces the lowest risk of stunting. The class collectively indicates a group that is well-informed about and actively practices key hygiene and nutrition-related behaviors, which can greatly reduce the risk of childhood stunting. Nearly all mothers in this class wash their hands before feeding children and after using the toilet. Family planning is also widely used, and most mothers possess good nutritional knowledge. While access to safe water is not universal, a good portion of households has it. Compared to the other classes, two-fifth of the mothers is employed. Most importantly, these mothers prioritize their children's health. The space births effectively, with high rates of antenatal care and early breastfeeding initiation. They also ensure food security and a varied diet within their households. The low prevalence of stunting (only 23.4%) in this class is a testament to the positive impact of these combined factors.
Class 2: High Risk With Socioeconomic Disadvantage and Limited Maternal and Child Healthcare Access
This is the largest group, comprising nearly half the children (47.1%). They are likely at a higher risk of stunting compared to Class 1 due to the presence of various risk factors. The majority of mothers within this group are unemployed, reflecting tight household finances and limited resources to meet basic needs. Typically, these mothers have never utilized family planning methods, leading to a high occurrence of short birth intervals among women, which can result in maternal nutrient depletion and hinder child growth. Despite over 80% of women attending antenatal care, a considerable portion, exceeding 20%, lacks this crucial preventive healthcare service. Poor nutrition and a lack of food knowledge are widespread among these mothers, affecting their ability to provide optimal diets for their children. Moreover, nearly all households experience food insecurity, with approximately 90% of children having insufficient dietary diversity, consequently exacerbating potential nutritional deficiencies. A significant 66.7% of the children in this group suffer from stunted growth.
Class 3: Mixed Risk With a Combination of Positive and Negative Factors
This group falls in between the other two in size (29.1%), and their risk of stunting also likely falls somewhere between Class 1 (lowest) and Class 2 (highest). This class presents a complex picture, defying easy categorization due to a mix of positive “Good Nutrition and Early Breastfeeding Practices” and negative “Economic Deprivation and Resource Insecurity” indicators impacting child stunting. While most mothers in this group practice good hygiene (washing hands before feeding and after using the toilet), many also utilize family planning and prioritize healthcare through high rates of antenatal care and early breastfeeding. However, this progress is challenged by widespread unemployment, limited access to safe water, and inadequate dietary diversity in over half of their children's diets. This combination, despite some positive behaviors, results in a significant proportion of 35.7% of children suffering from stunting, suggesting underlying nutritional deficiencies or chronic health problems.
Discussion
In our study, the overall prevalence of stunting in children under 24 months of age was 47.34%. However, our nuanced subgroup analysis findings reveal a significant disparity in stunting prevalence among the identified subgroups, emphasizing the importance of understanding the unique characteristics and vulnerabilities of each class. Accordingly, Class 1, labeled as 'Low-Risk,' comprised 23.8% of the children and exhibited the lowest prevalence of stunting at 23.4%. Class 2, labeled as 'High-Risk,' comprised 47.1% of the children and had a significantly higher prevalence of stunting at 66.7%. Class 3, categorized as 'Mixed-Risk,' had a moderate stunting prevalence of 35.7%. Remarkably, more than half, that is, 51.4%, of mothers had poor knowledge of food and nutrition. Likewise, 53.4% of mothers had unsafe drinking water. Similarly, the majority of children (61%) had poor dietary diversity. On top of that, only 15.7% of households had food security. Notably, our findings highlight the importance of early prevention and intervention strategies to mitigate the long-term consequences of stunting, particularly among high-risk subgroups.
The overall prevalence of stunting among under 24 months was comparable with a study conducted in Kenya, where 51% of children were also reported to be stunted. 40 The similarity in these findings may be attributed to shared demographic and socioeconomic characteristics among the communities studied. Contrastingly, several other studies have reported lower prevalence rates of stunting in young children. For instance, research conducted in Egypt found a rate of 20.3%, 41 while in Indonesia, the prevalence was reported to be 33.7%. 42 Similarly, studies in Southern Ethiopia 43 and Mumbai (India) 44 and a systematic review and meta-analysis pooled estimate in Ethiopia 7 reported rates of 37%, 38%, and 35.1%, respectively. Despite the geographical disparities in prevalence indicating potential variations in underlying risk factors across populations, it is noteworthy that all studies mentioned above uniformly classify the prevalence levels as 'very high,' with the sole exception of Egypt at 20.3%, which falls within the 'high' category, as defined by the WHO. 6 Therefore, this highlights the need for a standardized response to the public health crisis that is tailored to address the specific risk factors in each location.
However, our LCA successfully identified 3 distinct subgroups of children under <2 years old with varying stunting risk profiles. The “Class 1: Lower risk” exhibits the most remarkable combination of positive maternal behaviors, good nutritional practices, and access to healthcare. These factors work synergistically to create an environment that significantly reduces the risk of stunting in children.8,45,46 However, despite having a positive indicator, the observed moderate prevalence of food insecurity and limited safe water access suggest areas for potential improvement. Interestingly, this subgroup has a much lower stunting rate (23.4%) compared to other groups. This suggests that their high awareness and practice of hygiene and nutrition may be making a real difference. This indicates that implementing education and behavior changes focusing on hygiene and nutrition can effectively decrease the prevalence of child stunting.46,47 More importantly, in this class, mothers can serve as advocates and peer educators, sharing their knowledge and experiences with mothers in higher-risk groups to improve children's eating habits. 48
Conversely, Class 2 is characterized by socioeconomic disadvantages and a lack of maternal and child healthcare access. This Class of women has less formal education, limited access to family planning and safe water, lower breastfeeding initiation rates, and maternal unemployment, which are leading to higher stunting rates. Unsurprisingly, this class of children experiences a high rate (66.7%) of stunting. Our study result supported the existing research on the intricate interplay of various factors causing stunting in Class 2 children.23,40,49,50 The finding implies that interventions aimed at enhancing the health of mothers and children who are struggling with various challenges are crucial. 51 Although LCA does not directly identify individual households within particular latent classes; 52 it can identify similar groupings based on available data. Thus, stakeholders had better focus on this high-risk group by screening and tracking mothers with similar risk profiles to latent classes. Community health extension workers (CHEWs) play a vital role in rural communities and often have a good understanding of local households, 53 can identify mothers with similar risk profiles during home visits or health post visits, and may also administer screening questionnaires during ANC visit for key indicators and can consider for identifying mothers with similar risk profiles.
Class 3 is a group that displayed both higher and lower stunting risk characteristics, indicating a complex interplay of factors influencing their stunting. This complexity can make it difficult to determine the overall risk level for stunting and the most effective interventions to address the situation. 4 Despite good nutrition knowledge, high antenatal care and early breastfeeding can mitigate stunting risk factors;19,54–56 however, economic hardship, food insecurity, low family planning utilization, and limited access to diverse foods contribute to high stunting prevalence.23,57,58 Analyzing the distribution of positive and negative factors within Class 3 could provide further insights for intervention design. This suggests the potential for nutrition-focused behavior change communication intervention to promote hygiene practices, address food insecurity through social safety nets programs, and promote consistent family planning use can be effective strategies for Class 3 in resource-constrained settings.
In our study, we found that a child living in a household without access to clean drinking water has an increased chance of stunting. This finding is consistent with different studies conducted in Ethiopia.19,21,59 We also found that maternal hand-washing practice after visiting a toilet is a significant protective factor of child stunting. This finding aligns in diverse settings, including Indonesia, 60 Ethiopia,19,21,61 Bangladesh, 55 and Kenya. 62 The similarity suggests a potential mechanism to prevent the transmission of parasites and enteric bacteria, which cause diarrheal diseases and stunting in children. 46 Therefore, this result implies that, in order to lower childhood stunting, public health interventions should priorities hand washing and access to clean water through behavioral modification, infrastructural development, and water quality monitor. We also found that children with a long birth interval (≥2 years) had a lower likelihood of stunting, which is consistent with numerous studies.18,63,64 Moreover, stunting is higher in children born to a woman who had never used family planning and had no antenatal care follow-up history. Consistent with this, numerous studies18,63,64 have shown that short birth intervals are associated with an increased risk of stunting, while longer intervals are associated with a decreased risk.44,65,66 This might be due to the fact that consecutive pregnancies spaced closely together reduces the maternal recovery time and nutrient replenishment. 67 This suggests that increasing the demand for family planning use is necessary to ensure the best possible health and development of children throughout crucial times.
Our study reveals a significant link between maternal food and nutritional knowledge and child stunting, with women with better knowledge having a 77% lower risk. This finding is consistent with previous studies that found a significant relationship between stunting and maternal nutritional knowledge.41,68–72 This might be because nutrition knowledge is crucial for selecting nutritious foods for children, promoting healthy growth,73,74 and equipping mothers to feed on time, prepare healthy meals, and identify early disease signs. 75 This result implies the need for overarching nutrition education programs for pregnant mothers, particularly those who are undernourished, to improve their knowledge and practices regarding child feeding and nutrition. In our study, mothers with at least primary education have a lower likelihood of having a stunted child, which is in line with previous research.7,63,64,74,76 This might be due to improved health-seeking behavior, nutrition knowledge, and child growth.73,77 Likewise, maternal education significantly reduces the stunting risk by providing opportunities for healthy practices during pregnancy and lactation, 77 boosting self-efficacy, financial independence, health-seeking behavior, and enhancing knowledge about healthcare and child nutrition.. 73 By contrast, children born from households with severe food insecurity were more likely to be stunted, which is consistent with previous studies conducted in Ethiopia and Southeast Asia.57,78,79 The similarities might be due to the fact that food insecurity is linked to child stunting due to limited dietary diversity, increased susceptibility to infections, and inadequate nutrient intake. Thus, addressing this issue and promoting dietary diversity are crucial for optimal the child's growth and development.
Our study employed advanced statistical models (Bayesian logistic regression and LCA) to identify groups of children sharing similar stunting risk factors. This approach provides a deeper understanding of the issue, allows for targeted interventions based on stunting risk profiles (Low-Risk, Mixed-Risk, and High-Risk), and this approach enables subgroup analysis. However, we acknowledge the limitations inherent to LCA. While it effectively identifies at-risk groups, it does not pinpoint the exact risk factors defining each group. Further research is needed to shed light on these specific characteristics. Additionally, the study's design (cross-sectional and institution-based) limits generalizability to other populations. Finally, we used a relatively small sample size, which could potentially impact the reliability of the results, as LCA usually requires larger datasets for accurate risk group identification.
Conclusion
This study identified a concerning high stunting prevalence of stunting among under 2-year-old children, disproportionately impacting vulnerable populations. Notably, factors like good nutritional knowledge, longer birth intervals, maternal education, and consistent hand- washing practices were associated with a significant reduction in stunting odds. Conversely, lack of antenatal care, family planning services, access to safe drinking water, and consistent breastfeeding, coupled with food insecurity, emerged as significant risk factors. On top of these all, our nuanced subgroup analysis revealed previously undetected patterns within the stunted population. Three distinct stunting risk profiles were identified: “Low-Risk Group” exhibiting consistently positive behaviors; “High-Risk Group” facing multiple challenges; and “Mixed-Risk Group” demonstrating a combination of both positive and negative factors. The identification of these distinct latent classes underscores the crucial need to account for heterogeneity in risk factors when designing interventions. Therefore, healthcare practitioners should conduct screenings for stunting, provide nutrition counseling, promote breastfeeding, and educate families on nutrition and healthcare access. Policymakers should enhance food access, strengthen social safety nets, and support primary education. Moreover, future research should focus on elucidating the biological and social mechanisms driving these disparities in stunting prevalence.
Supplemental Material
sj-docx-1-hme-10.1177_23333928241271921 - Supplemental material for Analysis of Determinants of Stunting and Identifications of Stunting Risk Profiles Among Under 2-Year-Old Children in Ethiopia. A Latent Class Analysis
Supplemental material, sj-docx-1-hme-10.1177_23333928241271921 for Analysis of Determinants of Stunting and Identifications of Stunting Risk Profiles Among Under 2-Year-Old Children in Ethiopia. A Latent Class Analysis by Anteneh Fikrie, Berhanu Adula, Jitu Beka, Dejene Hailu, Cheru Atsmegiorgis Kitabo and Mark Spigt in Health Services Research and Managerial Epidemiology
Footnotes
Acknowledgments
We would also like to extend our deepest gratitude to Bule Hora University Research and Publication Directorate for the financial support to conduct this research. We would also like to express our great appreciation to the data collectors, supervisors, and all sincere study participants for their voluntarism and willingness to participate in our study.
Author Contributions
AF, BA, and JB: conceived, designed the study, supervised data collection, performed analysis, and data interpretation, drafted the manuscript, and approved the final manuscript. DH, CAK, MS: supervised data collection, performed statistical analysis, interpreted data, and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
All methods were performed according to the relevant ethical guidelines and principles of the Declaration of Helsinki. Accordingly, an ethical approval letter was obtained from the Bule Hora University, Institute of Health, and Institutional Ethical Review Committee (Ref. No: I/O/H/I/R//B/023/14). Informed written consent was obtained from all respondents after an explanation of the purpose of the study. Confidentiality of the participant's response was maintained by excluding personal information, such as the patient's name or card number throughout the study. All study participants were encouraged to participate in the study, and at the same time, they were also informed that they had the right not to participate
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bule Hora University financially supported the study.
Data Availability Statement
Data essential for the conclusion are included in this manuscript. Additional data can be obtained from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.