
Abstract
Objectives
A woman's health and wellbeing are impacted by illegal abortion since improper procedures can lead to consequences like extreme bleeding, infection, and damage to the reproductive organs and low awareness and attitude toward abortion law is one of the public health problems in Ethiopia. This study aimed to assess the knowledge, and attitude, and identify the effect of short birth interval and wealth index on the abortion law among reproductive-age women in Bule Hora town, Southern Oromia, Ethiopia.
Methods
A community-based cross-sectional study design was conducted from June 20 to July 20, 2022. A systematic random sampling technique was carried out to select 402 reproductive-age women. Data was collected by using a structured questionnaire with face-to-face interviews after the tools were pretested. The data was cleaned, coded, and entered into Epidata 3.1 and exported to STATA 14 for analysis. The model goodness of fit was checked using the Hosmer-Lemeshow test. Statistical significance is declared at P < .05 and a 95% confidence interval.
Results
The study revealed that 153 (38%) of respondents had good knowledge and 192 (47%) had a favorable attitude toward the Ethiopian abortion law, with a 100% response rate. Women's educational status, having information regarding the criteria of legal abortion services, and short birth intervals as a reason for induced abortion were significantly associated with knowledge. On the other hand, women who attended secondary education and above, have information regarding the criteria of legal abortion services, wealth index middle/average and richer, using the contraceptive method, and short birth interval as a reason for induced abortion were predictors of attitude toward Ethiopian abortion law.
Conclusion
This study shows that knowledge and attitude toward Ethiopian abortion law was not sufficient. So focusing on awareness creation and health education strategies by mobilization of the community to minimize the knowledge and attitude gap is essential.
Keywords
Introduction
Abortion is the expulsion of a fetus from the uterus or termination of pregnancy before fetal viability. 1 The World Health Organization (WHO) defines abortion as the termination of pregnancy and the expulsion of an embryo or fetus before the age of survival or 20 weeks of gestational age or <500g and, according to the Ethiopian definition of abortion, is the termination of pregnancy before viability (gestational age <28 weeks or fetal weight <1000 g).2,3
Globally, illegal abortion is the number one contributor to maternal mortality and morbidities, as well as the most significant social and economic burden on women, communities, and health systems, as well as physical and mental health issues. 4 Maternal deaths are caused by many factors, including hemorrhages, infections after delivery, and illegal abortions. 5 According to the WHO reports, 4.70% to 13.20% of maternal deaths that occurred in developing countries were due to illegal abortion. Roughly half of the abortions (21.6 million) performed worldwide are unsafe, and nearly all unsafe abortions (98%) occur in developing nations. 6
In Mexico, more than half of the women did not know about the legal status of abortion; as a result, they believed that abortions were never legal which increased the unsafe abortion problem in Mexico. 7 Because of restrictive laws in the United States, approximately 300,000 to 400,000 abortions take place each year; the majority of these are performed “underground,” with appalling maternal morbidity and mortality.8,9
In Africa, the majority of abortions are illegal and unsafe, and this remains alarming. 10 Because of restrictive laws in sub-Saharan Africa (SSA), abortion is clandestine and unsafe, contributing significantly to maternal mortality in Ethiopia, 6 in 10 abortions were unsafe, and estimated that up to 50% of gynecological beds are occupied by abortion-related causes. 11 Illegal abortions are a critical public health issue in Zimbabwe; due to low levels of knowledge about legal abortion. 12
In Ethiopia, since 2005 in circumstances of rape, incest, or fetal impairment, abortion is permitted. Additionally, a woman has the legal right to end a pregnancy if her life or physical wellbeing is at risk if she suffers from a physical or mental impairment, or if she is a minor who is not physically or mentally capable of giving birth. 13 A different study conducted in Ethiopia revealed that more than half of reproductive-age women have poor knowledge and unfavorable attitudes toward abortion law and don’t think that women would have the right to use the service or terminate their pregnancy even if the pregnancy fulfills the criteria. 14
The consequence of low awareness and attitude toward abortion law is one of the public health problems worldwide. As a result of low awareness and attitude toward abortion law; illegal abortion complications account for 5.80% of maternal deaths in Zimbabwe. 12 Several studies indicate that unsafe abortion accounts for up to 25% to 35% of maternal deaths and more than half of women didn’t know about the complications of abortion in Ethiopia. Illegal abortion complications account for a higher proportion of maternal morbidity, mortality, and gynecological admissions due to a lack of awareness and attitude toward abortion law. 15
Several studies in Ethiopia revealed that abortion-related complication such as shock, incomplete evacuation, infection, infertility, bleeding, emotional side effect, anemia, eclampsia, ruptured uterus, genital tract infection, and renal failure accounts for increased maternal morbidity and mortality. 16 A study shows that age, occupation, educational status, information source, family size, marital status, abortion history, a place where the abortion was done, and use of contraceptive method were significantly associated with knowledge and attitude toward Ethiopia's abortion law.5,14,16
The majority of women of childbearing age live in countries where abortion laws are extremely or moderately restricted, but the proportion of the abortion rate has almost doubled from 4.3 million to 8 million between 1995 to 1999 and 2015 to 2019, respectively. 17 Knowledge and attitudes about abortion laws can affect a woman's behavior in seeking care and her ability to access safe and legal abortion services. This study assessed new variables like short birth interval and wealth index association with knowledge and attitude toward Ethiopia's abortion law. The results of this study were useful to researchers in related fields. This study aimed to assess the knowledge, attitude, and associated factors of reproductive-age women toward abortion law in Ethiopia in the city of Bule Hora. The conceptual framework was adapted by reviewing different literature of knowledge and the attitude of reproductive-age women toward abortion law (Figure 1).

Conceptual framework of knowledge and attitude of reproductive-age women toward Ethiopian current abortion law and associated factors in Bule Hora town, southern Oromia, Ethiopia, 2022.
Methods and Materials
Study Area and Periods
The study was conducted in Bule Hora town, West Guji zone, Oromia Regional State South Ethiopia from June 20 to July 20, 2022. West Guji zone is found 467 km long away from Addis Ababa toward the south direction at 5°35′N latitude and 38°15′E longitude. Bule Hora town has an estimated population of 59,024 of whom 29,326 are males and 29,698 are females, 10,996 are reproductive age group, and 12,343 households. The estimated population in each kebele were Arda Biya (7130), Bule Kagna (7453), Bule Kilta (8060), Burka Mididi (6907), Ejersa Fora (9424), Gorro Abay (7319), Gorro Gudina (7118), and Kacha Ya’a (5613).
Study Design
A community-based cross-sectional study was conducted.
Population
Source Population
All reproductive-age (15-49) women in Bule Hora town.
The Study Population
All selected reproductive-age (15-49) women in Bule Hora town.
Study Unit
All selected individuals of reproductive-age women from the selected household.
Eligibility Criteria
Inclusion Criteria
All reproductive-age women who resided for at least 6 months in the study area were included in the study.
Exclusion Criteria
Those who were mentally ill and unable to communicate during the data collection period were excluded from the study.
Sample Size Determination and Sampling Technique
Sample Size Determination
The sample size for the first objective is calculated by using a single population proportion formula by considering the following assumptions: confidence interval (CI) = 95%, critical value Zα/2 = 1.96, degree of precision d = 0.05, and the prevalence of good knowledge of the Ethiopian current abortion law is 23.4%.
15


The sample size for the second specific objective is calculated using the single population proportion formula.


Where:
Z = 1.96, the confidence limits of the survey result (value of Z at α/2 or critical value for normal distribution at 95% CI) d = 5%=0.05 the desired precision of the estimate N = the total sample size p = prevalence of positive attitude on the legalization of abortion law 61.17%.
14
Sampling Technique
All kebeles in Bule Hora town were included. The number of reproductive-age women living in each kebele was taken from the Woreda health office. Then, the sample was proportionally allocated for each kebele. Finally, the systematic random sampling method was employed to select the women by every K interval household, and all reproductive-age women in the kebeles who fulfilled the eligibility criteria were incorporated into the study. From the household randomly select one participant. A revisit was conducted 3 times in closed households. The samples from a single kebele were calculated by the total sample size needed (402) was multiplied by the total number of households in the kebele and divided by the total number of reproductive-age women in 8 kebele (10,996) (Figure 2).

Schematic presentation of sampling procedures of reproductive-age women in Bule Hora town, southern Oromia, Ethiopia, 2022.
Method and Tools of Data Collection
The data was collected through a structured questionnaire used to collect the required quantitative information through a face-to-face interview. The data was collected by BSc nurses. Five data collectors and 2 supervisors were recruited to conduct the study. The principal investigator is responsible for coordination and supervision. The questionnaire consists of 39 questions divided into 5 sections that cover questions to assess sociodemographic, obstetric characteristics of reproductive-age women toward Ethiopian current abortion law, abortion-related factors, knowledge-related characteristics of reproductive-age women toward Ethiopian current abortion law, and attitude-related characteristics of reproductive age women toward Ethiopian current abortion law.5,14,15,17,18
Study Variables
Dependent Variables
Knowledge of Ethiopian abortion law
The attitude of Ethiopian abortion law
Independent Variables
Sociodemographic factors (age, marital status, wealth index, occupation, family size, educational status, and information source)
Obstetric-related factors (parity, gestational age, and gravidity)
Abortion-related factors (used contraceptive, history of induced abortion, short birth interval, and place where the abortion was done).
Operational Definitions
Data Quality Assurance
First, the questionnaire was developed in English and then translated into Afan Oromo, and then back to English by fluent speakers of the language. To keep the quality of the data, the questionnaire was adapted from Ethiopia Demographic and Health Survey and different literature conducted in similar geographical areas. The tool is pretested on 20 (5%) of the sample size in another town, Dugda Dawwa town, which is out of the study site 2 weeks before the actual data collection period. Based on the pretest, questions were revised, and edited, and those questions found to be unclear or confusing were removed before the actual study. The Cronbach’s alpha reliability test was performed to measure the checklist's internal consistency of knowledge questions and the coefficient was 0.85 and for attitude questions Cronbach's alpha at 0.79. 5 In addition, the supervisors and data collectors were trained for 2 days by the principal to investigate, the rules and regulations during data collection. Closer supervision was undertaken during data collection. The investigator collected the completed questionnaires every day and checked each for inconsistencies and omissions. Any format with a defect was rejected from the study.
Data Processing and Analysis
The collected data were checked for completeness and coded. Then it was entered into the Epi-data 3.1 version and exported into STATA version 14 23 for data cleaning and analysis. Descriptive statistics were presented with frequency, tables, charts, and graphs. The binary analysis was performed to calculate Crude Odds Ratio (COR) and to screen out potentially significant independent variables at a 20% level of significance to be included in the multivariable logistic regression model. 5 Multicollinearity was checked before the final multivariable analysis using the variance inflation factor, which was <2. The final multivariable model goodness of fit was checked using the Hosmer-Lemeshow test, and its value becomes insignificant (for knowledge 0.456 and attitude 0.590), which indicates that model goodness was fit. Finally, an adjusted OR together with 95% CI and a P-value <.05 were used to declare the statistical significance of the findings in this study.
The wealth index was calculated using the principal component analysis method. First, components were standardized. Then, the covariance matrix was constructed. Finally, components were extracted based on eigenvalues >1, factor loadings > |0.4|, and the cumulative proportion of variance explained by each component.
Ethical Consideration
An ethical clearance letter was obtained from Bule Hora University's research and publication directorate (reference number BHU/RPD/852/13). The official letter was written to the town health office to get permission for data collection. Town health bureau wrote an official letter to kebele administrations. Then written permission was also gained from kebele administrations. Confidentiality was ensured since the participants were anonymous. Every respondent was informed about the purpose of the study and voluntary basis participation, and the collected data were kept confidential. Finally, written informed consent was taken from each participant, and for those 15- to 17-year-old women, verbal consent from them only with parental/guardian permission was secured before data collection started.
Results
Sociodemographic Characteristics of Study Participants
A total of 402 study participants were included in this study, with a 100% response rate. Out of these, the majority of participants age 119 (29.6%) were from the 20 to 24 age group, and 114 (28.36%) were in the 25 to 29 age group. The mean age was 25.87 (SD ± 6.72) years. In terms of educational status, 93 (23.13%) of them attended primary school and 153 (38.06%) attended above college. The majority of them, 277 (68.9%) were married. In terms of occupation, 138 (34.33%) of women were housewives. Regarding religion, 269 (66.92%) and 70 (17.41%) of them were Protestant and Orthodox, respectively (Table 1). The wealth index in the study was 95 (23.63) and 115 (28.61%) of them were the middle/average and poorest, respectively (Figure 3).

Wealth index of reproductive-age women in Bule Hora town, southern Oromia, Ethiopia, 2022 (n = 402).
Sociodemographic Characteristics of Reproductive-Age Women Toward Ethiopian Current Abortion Law in Bule Hora Town, Southern Oromia, Ethiopia, 2022 (n = 402).

Obstetric Characteristics of Study Participants
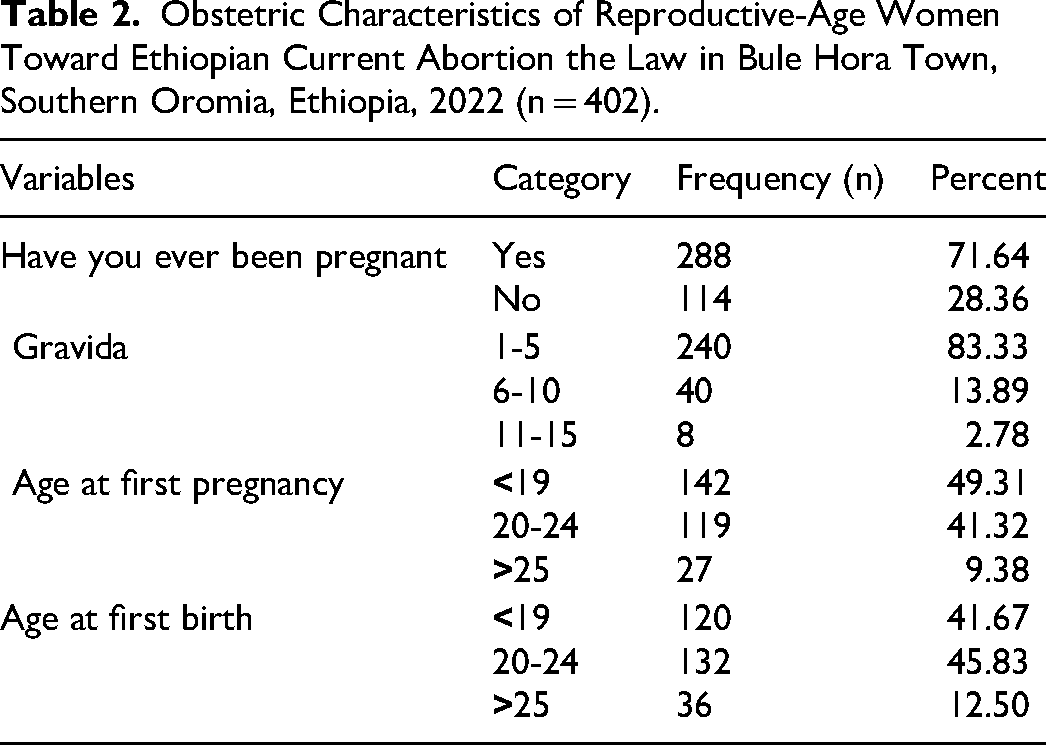
The majority of participants, 288 (71.64%) had a history of pregnancy. In terms of gravida, 240 (83.33%) were less than 6. One hundred forty-two participants got pregnant for the first time in <19 years. One hundred thirty-two respondents gave birth for the first time in 20 to 24 years (Table 2).
Obstetric Characteristics of Reproductive-Age Women Toward Ethiopian Current Abortion the Law in Bule Hora Town, Southern Oromia, Ethiopia, 2022 (n = 402).
Abortion-Related Characteristics of Study Participants
The study revealed that 74 (18.41%) had a history of abortion. The majority of them (78.38%) had a history of spontaneous abortion and 14 (18.92%) had a history of induced abortion. The study revealed that 246 (61.19%) of the participants used contraceptive methods and 106 (26.12%) respondents think that a short birth interval is a reason for induced abortion (Table 3).
Abortion-Related Factors Characteristics of Reproductive-Age Women Toward Ethiopian Current Abortion Law in Bule Hora Town, Southern Oromia, Ethiopia, 2022 (n = 402).

Knowledge-Related Characteristics of Reproductive Age Women Toward Ethiopian Abortion Law
Among reproductive-age women, 138 (34%) had heard about the Ethiopian abortion law. Regarding their knowledge level, considering 7 knowledge-assessing questions, 153 (38.06%) had good knowledge (Figure 4 and Table 4).

The composite score of knowledge of Ethiopian current abortion law in Bule Hora town, southern Oromia, Ethiopia, 2022 (n = 402).
Knowledge-Related Characteristics of Reproductive-Age Women Toward Ethiopian Current Abortion Law in Bule Hora Town, Southern Oromia, Ethiopia, 2022 (n = 402).

Attitude-Related Characteristics of Reproductive Age Women Toward Ethiopian Current Abortion Law
Regarding the attitudes of respondents, 48% of them had a favorable attitude toward the Ethiopian abortion law and almost 339 (84.33%) of the participants said that induced abortion shouldn’t be allowed by law and 63 (15.67%) women thought abortion should be utilized in certain situations such as rape, incest, harm to maternal health/life. The majority of respondents (67.91%) disagreed with interrupting pregnancy by age < 18 years and by mental abnormality (58.96%) (Table 5).
Attitude-Related Characteristics of Reproductive-Age Women Toward Ethiopian Current Abortion Law in Bule Hora Town, Southern Oromia, Ethiopia, 2022 (n = 402).

Factors Associated With Knowledge Toward Legalization of Abortion
Binary logistic regression analysis was conducted using an OR and 95% CI. The variables having a P-value of <.2 were transferred into multivariable logistic regression. On binary analysis, women's education, women's occupation, and partners’ occupation had information regarding the criteria of legal abortion services, wealth index, using the contraceptive method, and short birth interval reasons for induced abortion were candidate variables.
All factors of knowledge regarding Ethiopian abortion law were entered into a logistic regression model and the final associated factors were identified. The Hosmer and Lemeshow test was 0.456. In the multivariable logistic regression analysis from those entered into the model, women's education, information sources regarding the criteria of legal abortion services, and short birth interval reasons for induced abortion were statistically associated with women's knowledge status of the Ethiopian abortion law (P < .05). The study revealed that the knowledge of Ethiopian abortion law among women who had obtained their diploma certificate was 3.156 times (adjusted OR [AOR] = 3.156, 95% CI: 1.145-8.697) more likely to have good knowledge as compared to those unable to read and write. Similarly, women who had information sources regarding the criteria of legal abortion services were 4.009 times (AOR = 4.009, 95% CI: 2.492-6.451) more likely to have good knowledge as compared with women who had no information sources regarding the criteria of legal abortion service. Again, women who believe the short birth interval reason for induced abortion were 3.917 times (AOR = 3.917, 95% CI: 2.319-6.614) more likely to have good knowledge as compared with women who don’t believe the short birth interval reason for induced abortion (Table 6).
Factors Associated With Knowledge of Reproductive-Age Women Toward Ethiopian Abortion Law in Bule Hora Town, Southern Oromia, Ethiopia, 2022 (n =

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Factors Associated With Attitude Toward Ethiopian Abortion Law
Binary logistic regression analysis was conducted using an OR and 95% CI. The variables having a P-value of <.2 were transferred into multivariable logistic regression. On binary analysis, women's education, women's occupation, Partners’ occupation, having information sources regarding the criteria of legal abortion services, wealth index, type of abortion, use of a contraceptive method, and thinking of short birth interval reason for induced abortion were candidate variables.
In the multivariable logistic regression analysis from those entered into the model, women's education, having information sources regarding the criteria for legal abortion services, using the contraceptive method, and thinking of short birth interval as a reason for induced abortion were statistically associated with women's attitude status of the Ethiopian abortion law (P < .05). The Hosmer and Lemeshow test was 0.590. The study found that women with secondary education and above college status were 2.826 and 2.555 times (AOR = 2.826, 95% CI: 1.071-7.462, AOR = 2.555, CI: 1.108-5.892) more likely to have a favorable attitude toward abortion in Ethiopia than women who couldn't read or write. Similarly, women who had information source regarding the criteria of legal abortion services were 2.348 times (AOR = 2.348, 95% CI: 1.516-3.637) more likely to have a favorable attitude as compared with women who had no information source regarding the criteria of legal abortion services. The attitude toward the legalization of abortion among women who have a wealth index of middle/average and richer was 62.8% and 56.9% times (AOR = 0.372, 95% CI: 0.176-0.783) and (AOR = 0.431, CI: 0.201-0.923) less likely to have a favorable attitude as compared to women who have the richest wealth index.
Again, those who had used the contraceptive method 1.994 times (AOR 1.994, 95% CI: 1.288-3.086) were more likely to have a favorable attitude as compared with women who hadn’t used the contraceptive method. Similarly, women who thought the short birth interval reason for induced abortion was 2.442 times (AOR = 2.442, 95% CI: 1.492-3.998) were more likely to have a favorable attitude as compared with women who didn’t think the short birth interval reason for induced abortion (Table 7).
Factors Associated With Attitude of Reproductive-Age Women Toward Ethiopian Abortion Law in Bule Hora Town, Southern Oromia, Ethiopia, 2022 (n = 402).

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Discussion
This study aimed to assess the knowledge, attitude, and associated factors toward Ethiopian abortion laws among reproductive-age women in Bule Hora town, southern Ethiopia. This study found that 38.06% and 48% had good knowledge and a favorable attitude about Ethiopian abortion, respectively. According to this study, the knowledge of study participants about Ethiopian abortion law was lower than in a study conducted in Ethiopia, like Axum town 49.50%, 24 Yirga Chaffe town 48.90%, 14 Dabat district 62.80%, 25 Ambo University 55.10%, 17 and Nigeria University 50%. 26 Again, this finding was much lower than the study done in Debra Markos Hospital, 92%, 27 South Africa, 80%, 28 and Nepal (94.40%). 29 The possible reasons for the difference in the results were the difference in socio-economic conditions, variations in the study period, the accessibility of information services, and a lack of information dissemination. The possible difference might be due to the study design, and the sociocultural difference.17,29
This study was consistent with a study done in Bahir Dar city, which showed that 43% had good knowledge of Ethiopian abortion law, 5 the study done in Harari town revealed that about 35.70% of female students knew Ethiopian abortion law, 18 and Nepal, 41%. 30 The possible similarity might be due to the similar study design. 5 But, the finding of this study was higher than the studies done in Mozambique, 28.80%, 31 Zambia, 16%, 32 Mizan Aman town, 5.70%, 19 and Arba Minch University in southern Ethiopia, 32.10%. 33 The possible reason for the difference might be that there is a discrepancy in awareness-creation for women about the Ethiopian abortion law from place to place. This may be attributed to the participant's background, personal beliefs, health education about abortion law, social media coverage, and other sociocultural and religious factors. 20
Concerning women's attitudes toward abortion law, 47.76% of the respondents had a favorable attitude toward abortion legalization. This was similar to studies done in Bishoftu town, 48.40%, 34 and Axum, 47.50%. 24 However, it was lower as compared to the study in Yirga Cheffe town, 61.70%, 14 Mizan Aman town 54.40%, 20 Arba Minch town (56%), 15 and Nepal (94.30%) of women had a positive attitude toward the legalization of abortion. 29 This variation might be due to a lack of an information dissemination strategy throughout the country. This means that the majority of women do not get information on their affairs. In addition, the differences are probably due to the study design differences in community and institutional-based and study setting differences.20,29
But, the result was somewhat higher than the study done in Debra Markos Hospital, 23%, 10 Dire Dawa City, 30.60%, 35 North-West Ethiopia, Bahir Dar City, 43.50%, 11 Arba University, 30.30%, 36 and Bahir Dar city, 38%. 5 The possible justification might be due to different backgrounds, personal beliefs, and sociocultural. 5 About 84% of the study participants believe that induced abortion shouldn’t be legalized.
This study revealed that the diploma certificate educational status was a determinant of knowledge of Ethiopian abortion law. The finding is consistent with a study conducted in Yirga Chefe town, 14 Mozambique, 31 Zambia, 32 and Nepal. 30 The findings of these results are inconsistent with a study conducted in Bahar Dar City, 5 Debre Markos University, 27 and Gondar City. 37 The result of this study revealed that the odds of a woman's education positively influenced the likelihood of a woman's knowledge of the Ethiopian abortion law. As a woman's educational status increases, the probability of child-bearing women having good knowledge also increases. The possible justification was that when women are more educated, the probability of seeking information and using social media will increase; as a result, childbearing women might have better access to health information dissemination and might increase their knowledge of Ethiopian abortion law.5,30
Having an information source regarding the criteria of legal abortion services was statistically significantly associated with women's knowledge status of the Ethiopian abortion law. This finding is in line with a study done in Axum town. This is because women who have information about the criteria of legal abortion services have more knowledge about Ethiopian abortion law. 24
The thinking of a short birth interval, especially <1 year, as the reason for induced abortion was a statistically significant knowledge of the Ethiopian abortion law. Previously, studies done at national and international levels were missing this variable. The possible reason was that women who didn’t use the contraceptive methods suffered from short birth intervals, especially those of <1 year. For this reason, they try to induce their pregnancy in illegal ways. During this time, they seek information about Ethiopian abortion law, which increases knowledge of reproductive-age women. 38
Women who had attended secondary school and above were statistically significantly associated with positive attitudes toward Ethiopian abortion laws. This result is comparable with the studies conducted in Axum 24 and Arba Minch town. 15 The possible explanation is that as educational status increases, the chance of gaining more favorable attitudes increases due to gaining information in different ways. Individuals who had higher education levels had different sources of information and a better attitude toward abortion law. In addition, women with a higher education were more likely to be aware of the abortion law than those who did not have an education. This could be because these women could talk about issues such as family planning methods, abortions, or sex-related issues with their friends without being reluctant. 24
Having an information source regarding the criteria of legal abortion services was a statistically significant association with the attitude toward the legalization of abortion services. The finding is supported by a study conducted in Axum. The possible reason might be that women who have known the criteria for legal abortion services have a more positive attitude toward the legalization of abortion. 24 The wealth index was middle/average and richer and was statistically significantly associated with attitudes toward abortion law. This finding contradicted research done in Arba Minch town, 15 Bahir Dar city, 5 North West Ethiopia, 11 Dabat, 17 and Nepal. 30 The possible difference might be because a previous study revealed that monthly income, is not a wealth index. Women who have middle/average and richer wealth status could abort in the case of induction than those who are poor. During this process, they got information about Ethiopian abortion laws and improved their attitude. In addition, the difference could be due to study design differences and the study setting. 39
Using a contraceptive method was statistically significantly associated with an attitude toward Ethiopian abortion law. This result is not in line with studies done in the Dabat district 25 and the Harari region. 40 This might be due to those who used the contraceptive methods having more contact with a health professional and gaining information about maternal health and abortion-related issues, which might have changed their attitude toward Ethiopian abortion law. The thinking of a short birth interval, especially <1 year, as the reason for induced abortion, was statistically significantly associated with women's attitudes toward the Ethiopian abortion law. Previously, studies were missing this variable. The possible justification might be that lactating mothers are at greater risk of not using contraceptive methods due to fear of change in breast milk content, religious reasons, side effects, and partner refusal to use contraceptives. This causes unintended conceptions, which lead to a short birth interval. Unintended pregnancy might lead to induced abortion. When trying to induce abortion, they got information about abortion laws, which changed their attitude toward abortion laws. 38
This study was not without limitations. The study was conducted only in urban settings, and thus it is difficult to generalize the results to both urban and rural communities and cross-sectional study design was used, which makes it impossible to determine the causal relationships between the variables in the analysis.
Conclusion
Generally, the study revealed that the reproductive women in the study area have low knowledge and the majority of them have unfavorable attitudes toward the Ethiopian abortion law. This study shows the diploma certificate of educational status of women, having information sources regarding the criteria of legal abortion services, and thinking of short birth intervals as a reason for induced abortion were statistically significantly related to women's knowledge of the Ethiopian abortion law. On the other hand, women who attended secondary education and above college status, have information sources regarding the criteria of legal abortion services, wealth index middle/average, and richer, using the contraceptive method and thinking of short birth intervals as a reason for induced abortion had significant associations with attitudes toward Ethiopian abortion law. Health institutions should pay attention to providing health education at the town and health facilities with an emphasis on abortion law to the local community and awareness creation should be given based on the availability of legal abortion services and the use of family planning during breastfeeding to decrease the short birth interval problem.
Supplemental Material
sj-docx-1-hme-10.1177_23333928231220493 - Supplemental material for Knowledge, Attitude and Associated Factors Toward Ethiopian Abortion Law Among Reproductive Age Women in Bule Hora Town, Southern Oromia, Ethiopia, 2022
Supplemental material, sj-docx-1-hme-10.1177_23333928231220493 for Knowledge, Attitude and Associated Factors Toward Ethiopian Abortion Law Among Reproductive Age Women in Bule Hora Town, Southern Oromia, Ethiopia, 2022 by Zelalem Jabessa Wayessa, Balela Areri Boneya and Elias Amaje Hadona in Health Services Research and Managerial Epidemiology
Footnotes
Acknowledgments
We would like to express our heartfelt appreciation to Bule Hora University, data collectors, supervisors, and study subjects.
Authors’ Contributions
ZJW, BAB, and EAH designed the study, supervised the data collection, performed the analysis, and interpreted the data, and prepared the first draft of the manuscript. All authors worked on data interpretation and reviewed the manuscript critically. All authors read and approved the final manuscript.
Availability of Data and Material
For those who are interested, the datasets of this study could be accessed from the corresponding author upon reasonable request.
Consent to Participate
Written consent was obtained from all respondents. All respondents were reassured about the confidentiality of their responses. Their voluntary participation and the right to take part or terminate at any time they wanted were assured. The data collectors were trained by the principal investigators on how to keep the confidentiality and anonymity of the responses of the respondents in all aspects.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the Institutional Review Board of Bule Hora University (reference number BHU/RPD/852/13).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bule Hora University funded this research starting from the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Informed Consent
An official letter was obtained from the research and publication directorate of Bule Hora University to the town health office to get permission for data collection. Town health bureau wrote an official letter to kebele administrations. Then written permission was also gained from kebele administrations. Confidentiality was ensured since the participants were anonymous. Every respondent was informed about the purpose of the study and voluntary basis participation, and the collected data were kept confidential.
Data Availability Statement
All data included in this manuscript can be accessed from the corresponding author upon request through the email address.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.