
Abstract
Introduction
Postnatal period is a crucial stage of illness for mothers and their newborn children. Lack of post-natal care (PNC) services during this period is lifethreatening for both the mother and the babies. This study aims at examining the associated factors of PNC utilization among the mothers to explore the opportunities to accelerate it.
Methods
This study utilized the latest data from Bangladesh Demographic and Health Survey (BDHS) 2017–18, a nationally representative survey. A weighted sample of 5043 Bangladeshi women who gave birth three years prior to the survey was studied. Bivariate and multivariate analyses were performed to identify the underlying factors associated with the utilization of PNC.
Results
Around 63% women sought PNC from any kind of provider within 24 h to 42 days of the delivery among whom more than 48% received it from medically trained providers. Together with several sociodemographic factors- administrative division, place of residence, educational level, employment status, wealth status, some maternal factors such as- antenatal care (ANC) visits, place and mode of delivery- played a significant role in utilizing PNC services from trained providers.
Conclusion
To further improve utilization of post-natal care, national and local level action plans should be introduced to promote health facility delivery irrespective of their place of residence. In the meantime, PNC awareness campaigns, intervention and economic empowerment programs targeting mothers from the poorest quintile needs to be implemented, particularly those who are unable to attend at least four ANC visits, and have accessibility issues to education.
Introduction
Despite having noteworthy accomplishments in reducing maternal death in the last two decades, globally about 295,000 women die from complications related to pregnancy, of which most of them occured in developing countries including Bangladesh. 1 Most of the causes of maternal mortality are due to excessive bleeding, which often occurs after childbirth, postpartum infections, prolonged labor, and unsafe abortion. 2 Postnatal care (PNC) for the new mother and her child is crucial to treat any future complications emerging from the child delivery and to provide the mother with important health information. 3 Bangladesh, located in South Asia and being a part of the Least Developing Countries (LDCs), witnessed around 5100 maternal death due to pregnancy and related complications in the recent year 1 ; more than 50% of which could have been prevented by ensuring proper care in the post-partum period starting about an hour after the delivery of the placenta and includes the following six weeks.4,5
According to the recommendation of the World Health Organization (WHO), all mothers and newborns should receive postnatal care (PNC) within the first 24 h of birth and they should also receive at least three additional postnatal check-ups within 42 days of the birth.5,6 Circumventing routine postnatal check-ups can pose a major challenge to safe motherhood resulting in post-partum hemorrhage, eclampsia, puerperal genital infection, thromboembolic disease, difficulties in breastfeeding, and psychological problems (baby blues). 4 Globally around 30% of maternal deaths occur during the post-partum period 7 ; while in Bangladesh mothers are enduring more than 68% of deaths in the post-partum period mostly (31%) caused by post-partum hemorrhage 8 which has shed light on the perilous consequences of inadequate utilization of PNC. Such figures can create a major hindrance in reaching the maternal mortality target of fewer than 70 deaths per 100,000 live births by 2030 (which is a major indicator of the third UN Sustainable Development Goal (SDG) 9 ), while also delaying the country's progress towards achieving Universal Health Coverage by 2030. 10
Comprehending the importance of adequate utilization of PNC, the Government of Bangladesh is aspiring to achieve 80% postnatal care coverage within 48h of the delivery from a medically trained provider by 2025 and 100% by 2030. 11 Therefore, it is imperative to focus on the factors associated with the utilization of PNC among the women of Bangladesh to inform the policymakers to be concerned of. An ample of studies highlighted the association between PNC utilization and various factors such as socioeconomic factors (educational level, employment status, and economic status of individuals),3,12–24 demographic characteristics (administrative division, place of residence, and mother's age at birth),3,12,13,19–22,25,26 and birth-related factors (antenatal care visits and, place and mode of delivery).3,13,16,18,19,21,22,24,27–35 Although, a body of literature in Bangladesh have focused on post-natal care services of mothers from the perspectives of different region,36–38 income level 39 or age, 12 a dearth of studies using recent nationally representative data in this topic is still dominant. Furthermore most of the studies focused on early utilization of PNC 13 ; whereas the condition of the mother can worsen at any time during the post-partum period which makes the entire period of PNC highly crucial for maintaining maternal well-being. 4 To make a proper understanding of the various demand-side factors associated with PNC, this study utilized recent nationally representative data. The findings from the study will contribute developing up-to-date evidence for the policymakers and other stakeholders to design more effective interventions needed to accelerate the utilization of PNC and improving maternal health in Bangladesh.
Materials and Methods
Study Design and Settings
The study was conducted among Bangladeshi mothers and we used the latest Bangladesh Demographic and Health Survey (BDHS) 2017–18 data, which is a nationally representative cross-sectional household survey designed to obtain demographic and health indicators. The survey was implemented from October 2017 to March 2018, under the National Institute of Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare covering all 8 administrative divisions of Bangladesh. The survey design adopted a two-stage stratified cluster sampling procedure to select households. The survey selected 675 enumeration areas (EAs) in the first stage and conducted household listing for each EA in both rural and urban areas. Consistently, an average of 30 households were selected systematically from each EA in the second stage. The detailed method, sampling procedure, survey design, instruments, measuring system, data validity, reliability, and quality control are described elsewhere. 40
Population and Sample Size
A structured questionnaire was administered by trained and experienced interviewers, and 20,127 ever-married reproductive (15-49 years) women who had childbirth in the last 3 years prior to the survey were interviewed to capture socio-economic, demographic, and health care utilization data at the household level. Data regarding the most recent live birth were collected in the cases of women with a history of giving more than one live birth which made the total number of samples to be 5051. Disregarding the missing values, a weighted sample of 5043 mothers was included in the analysis.
Outcome Variables
This study focused on three outcome variables: first, outcomes related to post-natal care utilization of mother aged 15 to 49 years for the last birth in the last 3 years (coded into “1” if utilized the care within the first 24 h and 42 days of delivery and “0” in case of the opposite); second, timing for PNC visits/checkups was defined into three categories- as the majority of maternal and newborn deaths occur during the first few hours and days after birth, 5 it was coded as of visited within first 24 h, 2–6 days and 7–42 days and third, the health care seeking behavior for PNC utilization of mother was coded into “Trained Health Care Providers” (qualified doctor, nurse/midwife/paramedic, family welfare visitor, community skilled birth attendant, community health care provider, health assistant, family welfare assistant, trained traditional birth attendant, NGO workers were considered as trained health workers) and “Untrained Health Care Providers” (untrained traditional birth attendant, unqualified doctor and others).
Explanatory Variables
Different independent variables including socio-demographic and type of delivery assistance were focused on to explain the influencing factors of PNC utilization. Divisional distribution, urban-rural classification, mother's age at birth (coded into 15-19 years, 20-24 years, 25-29 years, 30-34 years, and 35-49 years), and educational status of both respondent and her husband (categorized as “No education”, “Primary level”, “Secondary level” and “Higher”) were included in this study. In addition to these, the mother's occupation was categorized as “Homemaker/ no formal occupation”, “Agriculture related employment” (landowner, farmer, agricultural worker, fisherman, poultry raising, cattle raising, home-based manufacturing), and “Professional”. Moreover, the wealth index of the participants was categorized as “poorest,” “poorer,” “middle,” “richer,” and “richest” and access to media was recorded as the frequency of reading newspapers, listening to the radio, and watching TV (categorized as “Yes” if they had access to anyone these media at least once in a week; and “No” otherwise).
Other variables included utilization of antenatal care (ANC) (categorized as “No ANC”, “1 to 3 ANC” and “4 and above”), birth order of child (coded into four-category as the first order, second-third order, fourth-fifth order, sixth and more births), and mode of delivery which was categorized into “Normal Vaginal Delivery (NVD) and “Cesarean Section”. Again, place of delivery was coded into “Respondent's home”, “Public hospital” (public hospital, district hospital, maternal and child welfare center, Upazila health complex, Upazila health and family welfare center, other public sector and community clinic), “Private hospital/clinic”, and “NGO and Others”. If the respondent confronted at least one challenge to access health care (e.g., not getting permission to go, not getting the money needed for the treatment, distance to a health facility or not wanting to go alone), then the variable perceived difficulty to access health care was coded into “1” (facing at least one problem); otherwise, it was “0” (facing no problem).
Statistical Analysis
Descriptive analysis such as frequency distribution as well as cross-tabulation was applied for calculating the prevalence of PNC utilization focusing on important variables. A Chi-square test of association was applied to test the statistical significance of bivariate distributions of dependent variables across independent variables. To determine the factor affecting PNC utilization and health care-seeking behavior, two logistic regression analyses have been used- model I presenting the factors affecting the utilization of PNC and model II capturing the variables working behind healthcare-seeking behavior for PNC utilization. The results were presented in terms of adjusted odds ratios (AORs) with a 95% confidence interval (CI) and statistical significance was considered at a P-value of <.05 in all analyses. The variance inflation factor test was employed to detect the multicollinearity in the regression model. All statistical analysis was done using the statistical package Stata/SE 14 software.
Results
Background Characteristics of the Participants
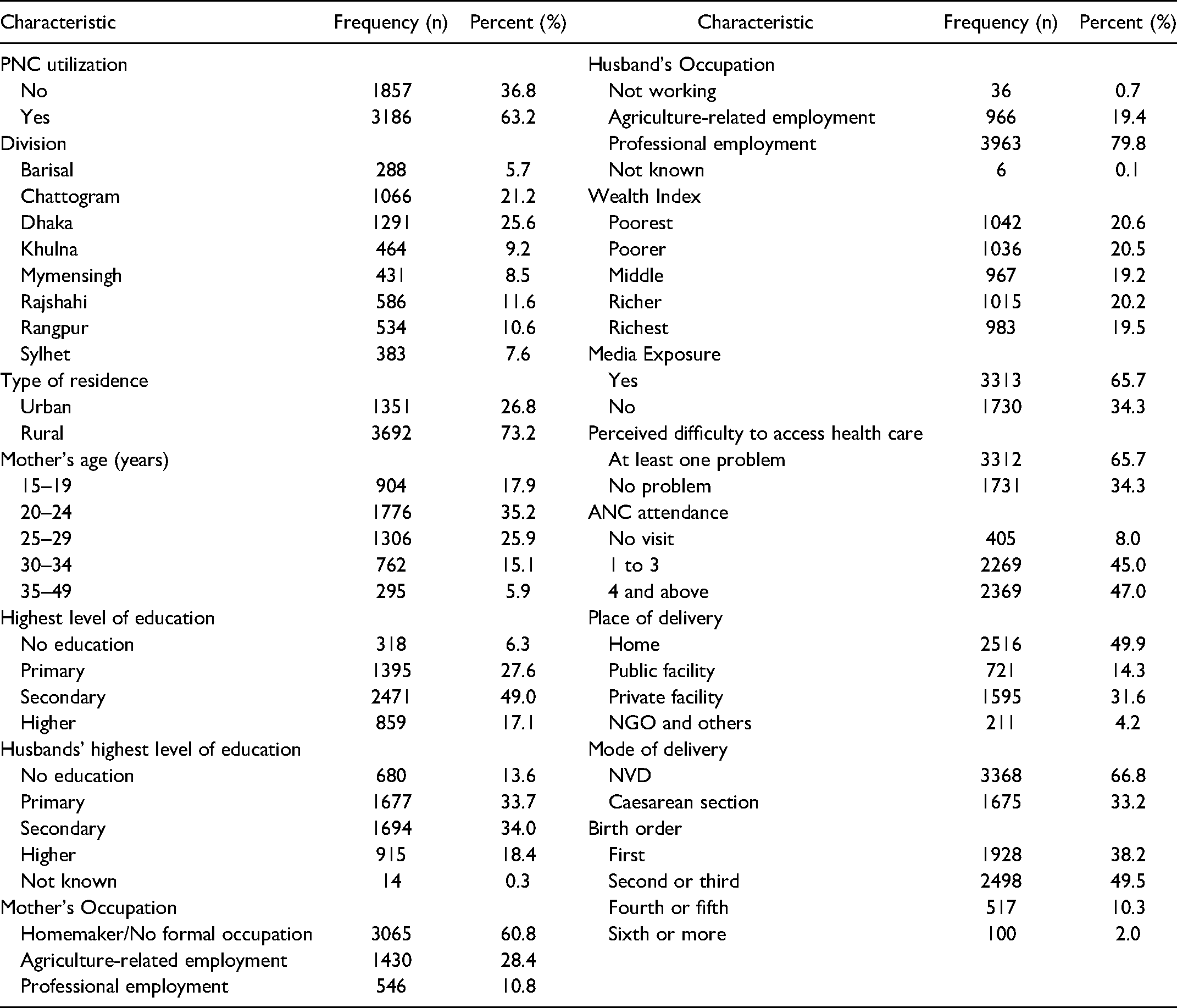
Table 1 illustrates the background characteristics of 5043 respondents in the study. More than half of the women (63.2%) utilized post-natal care from any sort of health care provider. The result showed that most of the respondents (25.6%) were from Dhaka division and majority (35.2%) belonged to the age group of 20–24 years. The lion part of the women (73.2%) belonged to rural area with majority having no formal occupation (60.8%); whereas, most of the respondents’ husbands (79.8%) had professional employment. Almost half of the respondents (49%) had passed the secondary level while 34% of their husbands had the same educational qualification. Almost an equal portion of participants belonged to each quintile of the wealth index and the majority of them (65.7%) had exposure to some form of media. Almost half of the mothers (47%) attended 4 or more antenatal care visits although 65.7% of them faced some sort of challenges to access health care. Almost 67% of mothers had normal delivery and 50% of the women had their delivery done at home.
Socio-Demographic and Maternal Characteristics of Women (n = 5043).
Utilization of Post-Natal Care Across Background Characters
Table 2 picturizes the percentage of women utilizing PNC services from both trained and untrained providers from different backgrounds. Utilization of PNC was higher among the mothers from Mymensingh division (69.7%) followed by the mothers from Chattogram division (69.6%). The rural and the middle-aged (30-34 years) mothers utilized more PNC; while the mothers having secondary and higher education utilized less PNC (56.7%). Women who were engaged in agriculture-related work frequently utilized PNC (70.5%); whereas women from the richer quintile were more vulnerable to using PNC services. Further, women having home delivery and also who did not pay any ANC visit utilized more PNC.
Percentage Distribution of Women by Utilization of Postnatal Care.

In the case of timing for PNC check-ups, the frequency varied by different factors (see Table 2). Within the first 24 h after the delivery, the majority of the women (31.3%) from the poorest quintile utilized PNC; whereas, the richest participants utilized PNC within 7–42 days after the delivery. Mothers who delivered at home had a higher percentage (99%) of utilizing PNC within the first 24 h than their counterparts who availed institutional facilities; the majority of the participants (73.3%) who had their check-up after 7–42 days, availed the private facilities. Women undergoing cesarean section delivery mostly had their PNC check-ups within 7–42 days (84%), while women utilizing PNC within the earliest period (24 h) experienced NVD. In addition to these, utilizing PNC during different time spans varied by residential and divisional disparities, educational qualification, occupation, birth order of the child and perceived difficulties to access health care.
Health Care Seeking Behavior of PNC
In Figure 1, the health care-seeking behavior is illustrated. Among the total prevalence (3186), 48.3% (CI = 47.3, 49.3) of respondents visited the medically trained provider to utilize post-natal care within 24 h to 42 days after the delivery. If the socioeconomic condition is considered, mothers from the poor groups (first 3 quintiles) mostly sought treatment from untrained PNC providers, whereas utilization of care from the trained provider is the highest (30.2%) among the mothers from the richest quintile. The figure also reveals the fact that mothers who sought care from untrained providers mostly (33.4%) belonged to the poorest quintile.

Proportion of PNC utilization among women across wealth quintile.
Factors Associated with PNC Utilization
The factors that are closely related to the prevalence of PNC utilization and the health care seeking behavior are demonstrated in Table 3. From the binary logistic model, we found that divisional and residential variation, educational qualification and occupation of the respondents, economic status and other maternal characteristics (ANC visits, delivery mode, and place) played a significant role to influence the mothers for utilizing PNC and that also from a trained provider. The result showed that the mothers from Chattogram (aOR = 2.14, 95% CI = 1.73, 2.64), Rangpur (aOR = 1.64, 95% CI = 1.25, 2.16), Sylhet (aOR = 1.54, 95% CI = 1.15, 2.08), and Mymensingh (aOR = 1.45, 95% CI = 1.09, 1.92) were more likely to seek PNC than the mothers from the capital city, Dhaka. In the case of seeking treatment from trained providers, the respondents from the Barisal division had higher odds (aOR = 1.61, 95% CI = 1.08, 2.4); although the mothers from the Rajshahi division were 32% less likely to visit the trained PNC provider (aOR = 0.68, 95% CI = 0.47, 0.97). The respondents from urban area were more prone to utilize PNC (aOR = 1.35, 95% CI = 1.13, 1.62) and also from the trained provider (aOR = 1.69, 95% CI = 1.33, 2.15) than their counterpart from rural area. Women passing the secondary and higher level of education had higher likelihood of receiving treatment from trained PNC providers than women with lower or no educational qualification (aOR = 1.76, 95% CI = 1.17, 2.66, and aOR = 2.46, 95% CI = 1.48, 4.11). The study also found that mothers engaged in agricultural-related employment were 1.37 times more likely to receive PNC and had 1.27 times higher odds to receive that treatment from trained providers than the mothers with no formal occupation. If the economic status is considered, mothers from the richest quintile were 86% more likely to seek PNC from trained providers than the mothers from the poorest quintile; while the odds of the richer mothers for the same purpose was 1.39 (95% CI = 1.01, 1.92).
Factors Associated with post-Natal Care Utilization among Mothers who Gave Birth in the 3 Years Preceding the Survey (BDHS 2017-18) in Bangladesh.
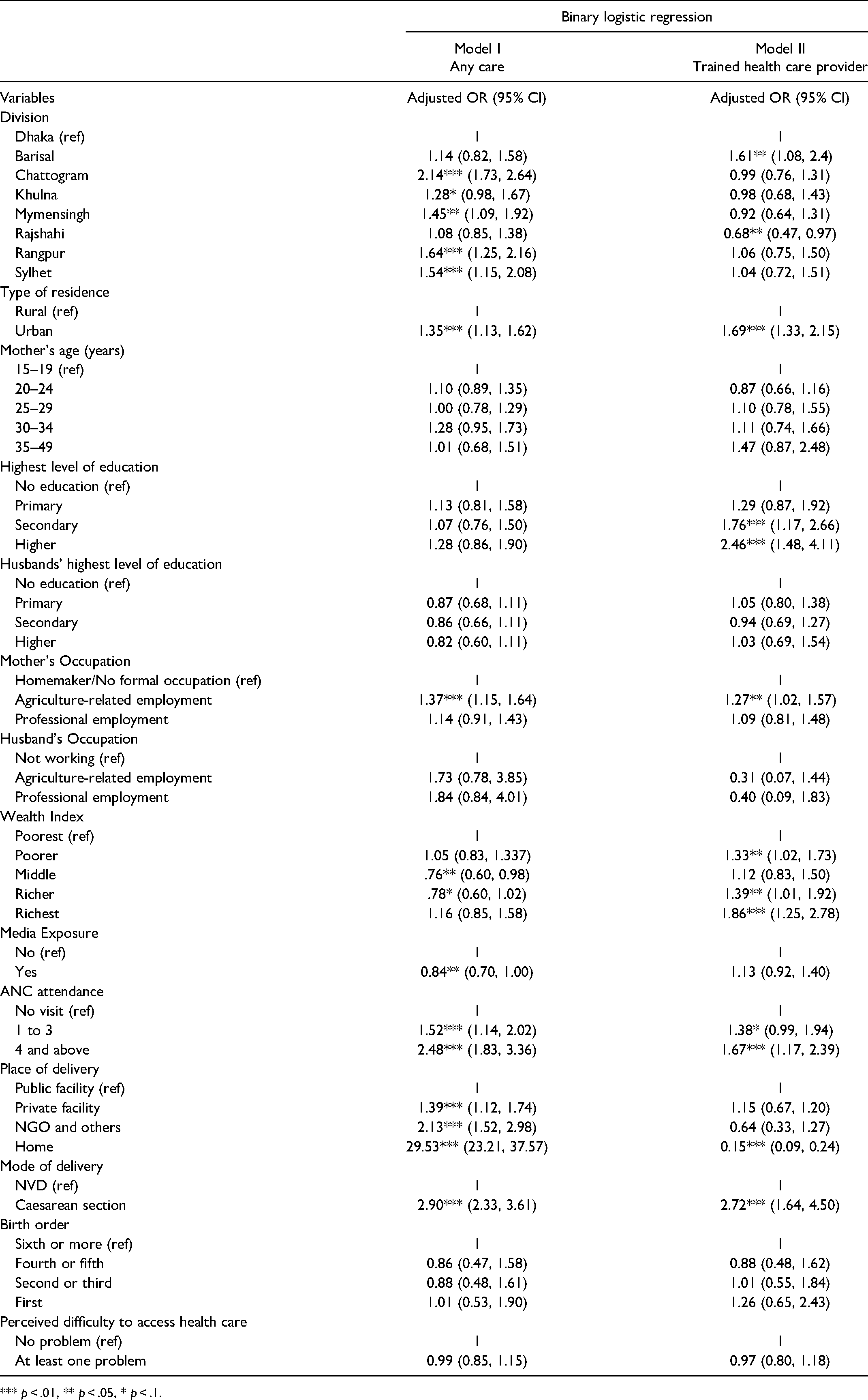
*** p < .01, ** p < .05, * p < .1.
During the pregnancy period, the mothers who paid optimal number of antenatal care visits (4 and above) were 2.48 times more likely to utilize post-natal care than the mothers who had no visit at all. In the case of receiving treatment from trained providers, they (paying ANC visits 4 and above) were 67% more likely than their counterparts to pay no visit. In the case of utilizing PNC from any sort of provider, the women who had home delivery had the highest odds of doing it than those having institutional delivery (aOR = 29.53, 95% CI = 23.21, 37.57). However, the result turned in an opposite direction when the trained providers were considered. Women having delivery at home were the least inclined to avail PNC services from the trained health care providers than the mothers having intuitional deliveries (aOR = 0.15, 95% CI = 0.09, 0.24).
Discussion
Utilizing post-natal care from a medically trained provider can prevent severe complications during the post-partum period by detecting and providing proper treatment to the mothers resulting in reduction of maternal morbidity. Nevertheless, the prevalence of PNC is still quite low in Bangladesh. This study made an effort to identify the underlying factors causing the low prevalence of PNC among mothers in Bangladesh using the latest nationally representative data.
During our analysis of BDHS 2017–18 data, we discovered that nearly half of the women utilized PNC from medically trained providers within 42 days of the delivery which is almost similar to the findings of the national survey within 2 days of the delivery (52%). 40 This figure is higher to some extent than the prevalence reported in BDHS 2014 (34%). 41 Though the prevalence has risen over the years, this figure is not so impressive compared to other neighboring countries such as India (65%), 18 Myanmar (68%), 42 Nepal (59%), 43 Indonesia (78.5%) 34 and African countries such as Benin (68%) 44 and Zambia (63%). 35 While some other African countries such as Nigeria, 19 Ethiopia, 3 Rwanda, 45 and Kenya 46 have a lower prevalence of PNC than Bangladesh. Such distinctions can be a reflection of the variation in country-specific factors and, also the strength of the health care system providing maternal and child care.
The results of the multivariate analysis of the study indicated the following factors as correlates of PNC utilization in Bangladesh: variation in administrative divisions and place of residence, women's educational level and employment status, wealth status, ANC attendance, place of delivery, mode of delivery and exposure to media. From our analysis, it was observed that compared to the capital city Dhaka, all other divisions performed better regarding utilizing PNC from any provider- trained or untrained; while the scenario was different when only trained provider was considered. This wide range of variation in utilization of PNC across the administrative divisions is evident in several studies conducted earlier.13,20,25 Existing disparity in availability of and accessibility to health facilities and also the quality of health services in the divisions can be the possible reasons for working behind this.
The study also revealed that the mothers from the urban area had higher odds of utilizing PNC within 42 days of the delivery-irrespective of the type of providers. This finding is consistent with an ample of studies- conducted both in the national and international context.3,12,19–22,26,38 In rural areas, distance to the nearest health facilities might be a major hindrance in accessing health care services which have been validated by many studies. 12 Moreover, lack of improved electricity, transportation, water and sanitation services, and access to health promotion programmes often prevent mothers in rural areas from utilizing adequate PNC services.
Our participants completing the secondary and higher level of education were more prone to receive PNC from provider who are medically trained. This finding is in agreement with the evidence from several South Asian and African Countries.14,15,19–24,27,28 This kind of association can be explained by the fact that educated women are expected to realize the risk of not utilizing PNC resulting in improved health-seeking behavior. Additionally, knowledge and information on the availability of health care services influence educated women to attain and preserve better health. Completing the secondary or higher level of education may empower women with higher socioeconomic status and enable them to take decisions independently regarding any health care service utilization.
This study also demonstrated that women engaged in agricultural-related employment were more likely to utilize PNC than their counterparts who were not employed in any sector. Another study conducted in Uganda using Demographic and Health survey data from 2016 also supports this finding. 24 In Bangladesh, 65% farm labor force is constituted by women and more than 70% of female workers are engaged in the agricultural sector.47,48 This huge participation of women in such activities empower them with a more secure position in society by improving their socioeconomic status which resulted in their independence in decision-making while taking any care from the trained provider. 49 Indeed, the power of decision making often comes from achieving education influencing women to utilize PNC services which is also associated with women's autonomy and control over resources.
Several studies from different countries revealed that mothers from rich households are more inclined to avail PNC services from trained providers which is also an indication of comparatively lower utilization among mothers from poor households.3,12,13,16,18–23,50 Our study also echoes similar findings in the case of PNC utilization among Bangladeshi mothers. This might be due to their dependency on the out-of-pocket cost for availing healthcare which is excessively high in Bangladesh. Indeed, it was observed that women from the wealthier index belong to households who can afford the medical and non medical cost of PNC. Allocating only 5.4% of the total budget for the health sector which is less than 1% of gross domestic product (GDP) share, compels the people of Bangladesh to bear around 74% of health care costs from their pocket.51,52 This huge burden of health care costs also justifies the hypothesis that poor families are unable to afford the additional cost resulting from using services from qualified healthcare providers.
This study highlighted that the mothers who had exposure to any kind of media such as radio, television, or newspaper were less inclined to avail PNC from any kind of providers irrespective of their qualification compared to their counterparts who were not exposed. This result differs from the study conducted in Uganda, 24 Ethiopia, 16 Nigeria, 17 and Malawi 53 where only qualified providers were considered. This counterintuitive incidence can be explained by the fact that highly educated women who are already aware of the seeking behavior are more likely to be exposed to media. 54
If the enabling factors are considered, the mothers who had optimum ANC visits (four or more) had higher odds of receiving a PNC checkup than their counterparts who had fewer visits, which is validated by the previous findings of India, 18 Pakistan, 21 Nepal, 22 Ethiopia,3,16,27,29 Nigeria, 19 and Uganda. 24 A possible explanation of this finding is that exposure of pregnant women to counseling and knowledge during ANC visits about the health risk of the post-partum period encourage them to utilize adequate PNC services which keep them at a beneficial position irrespective of their socioeconomic status.
When only the medically trained providers of PNC were considered, the findings of the study revealed that women having delivery at home were less likely to utilize PNC compared to the mothers who had institutional delivery, which was completely different from the result of other studies where the type of providers were not being accounted for. This interesting finding resonates with the results of several previous studies to some extent.3,13,19,22,24,27–32,34,35 In Bangladesh almost 50% of the delivery is done at home in the presence of a traditional birth attendant and nearest relatives which poses a great challenge for the mother to utilize PNC from trained providers. 40 Alternatively, institutional delivery provides more opportunities for the mothers to pursue knowledge about the importance, accessibility, and availability of PNC utilization as they had to stay in the facility for a significant duration of time. 55 Moreover, this finding also made it obvious that women who had cesarean section delivery at different facilities had higher odds of receiving PNC from trained providers within 42 days of the delivery. Studies conducted in India, 18 Ethiopia 32 and Tanzania 33 also validate these findings. The mothers having cesarean section delivery are more prone to face complications that can be mitigated by required follow-up services resulting in improved health care-seeking behavior.56,57
There are several limitations of this study. The study was based on cross-sectional data, which failed to establish a causal relationship. All information related to the PNC services was provided by mothers which makes it subjective. Further, the self-report system of the participants makes this study suffer from recall bias. The BDHS dataset lacks the queries about the numbering and the contents of PNC recommended by WHO which can be pointed as another limitation. However, the current study has used high quality, nationally representative household survey data from both the urban and rural areas, which is the strength of this study.
Conclusion
This study observed more than half of the women sought PNC from various health care providers within 24 h to 42 days of the child's delivery while about 48% of mothers received PNC services from medically trained providers. The findings of the study accentuate the importance of reinforcing the health system and improving the maternal care services focusing especially on women who are from rural areas, have lower than secondary level of education, receive no ANC visit, deprived of institutional delivery, and from the lowest wealth quintile having no employment status. Apart from paying special attention to educate the women, national and local level action plans should be materialized to strengthen the health facilities to provide quality maternal care involving ANC, delivery care, and PNC services. To attain the targets and objectives of Bangladesh National Strategy for Maternal Health 2019–2030 in reality, PNC services should be made accessible to all women in need irrespective of their socio-economic status; thus, opening the door towards achieving UHC within 2030 by reducing maternal morbidity and improving overall maternal health and well-being in Bangladesh.
Footnotes
Author's Note
The study analyzed a publicly available DHS data set by taking consent from the MEASURE DHS program office. DHS followed standardized data collection procedures. According to the DHS, written informed consent was obtained from women enrolled in the survey.
Acknowledgments
We are grateful to Measure DHS for allowing us access to the 2017–18 DHS dataset for Bangladesh.
Authors’ Contributions
All the authors conceptualized and designed the study. All of them were involved in data analysis, interpretation, and writing of the manuscript. Finally, all of them critically read and reviewed the manuscript before giving final approval for publication.
Availability of Data and Materials
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article