
Abstract
Background
Maternal and infant mortality is a major problem in a developing country like Bangladesh and these deaths are mostly related to incomplete antenatal care (ANC) visits. Adequate ANC visits for women are crucial in controlling maternal and infant mortality.
Aims
To investigate factors associated with ANC visits among women of reproductive age (15-49) in Bangladesh using the Bangladesh Demographic Health Survey 2017–2018 (BDHS) data.
Methods
This study included 5012 respondents, of whom 2414 women (48.2%) were complete ANC visits and 2598 women (51.8%) were incomplete ANC visits. Quantile regression was used for analysis indicating that the effects of different covariates functioned differently across the utilization of antenatal care visits. The results revealed the women's educational level, birth order number, sex of household head, and wealth index were highly significant on the lower, middle, and higher quantiles of the number of incomplete ANC visits. Besides, in the higher quantiles (for example, 75% quantile), the place of residence was highly significant. For division variables, Rajshahi, Rangpur, and Khulna were highly significant in lower and middle quantiles, while Dhaka, Khulna, Mymensingh, and Rajshahi were insignificant in higher quantiles.
Conclusions
This study observed that education, wealth index, birth order of children, and place of residence are associated with utilization of ANC visits and significantly influence maternal mortality. These determinations can help healthcare programmers and policymakers to take appropriate policies and programs for complete antennal care visits among pregnant women in Bangladesh. In order to increase the number of ANC visits among women, it is necessary to establish a mutually coordinated and trusting relationship between the government, non-governmental organizations and NGOs.
Introduction
Antenatal care is the care women of reproductive age receive from health professionals during pregnancy. Worldwide, approximately 830 women died every day due to a lack of proper care in various fields including health, pregnancy period, childbirth, and nutrition. 1 Among these unexpected deaths, the most complicated deaths occur during pregnancy. Complications during pregnancy endanger not only the life of the mother but also the life of the child. Maternal mortality is currently one of the significant impediments to human development worldwide. 2 Maternal mortality refers to deaths due to complications from pregnancy or childbirth. According to UN inter-agency estimates, the global maternal mortality ratio declined by 38% from 342 deaths to 211 deaths per 100 000 live births from 2000 to 2017. 3 World Health Organization (WHO) refers about 303 000 women died in 2019 due to pregnancy-related complications. 2
The government of Bangladesh is committed to achieving the targets for Sustainable Development Goals (SDG). The Sustainable Development Goal 3 target is to reduce the maternal mortality rate to 70 deaths per 100 000 live births, reduce the under-5 mortality rate to 25 deaths per 1000 live births, and reduce the neonatal mortality rate to 12 deaths per 1000 live births by 2030. 4
ANC is one of the most effective interventions to prevent these unexpected deaths.2,5 ANC is a service through which pregnant women are made aware of their health to stay healthy and give birth to a healthy child. The main goals of the ANC are to reduce maternal mortality and improve health care services. There are two types of ANC providers; qualified and unqualified. Medically trained providers (such as doctors, nurses, midwives, and community health care workers) who are considered qualified providers whereas unqualified physicians and NGO workers are considered unqualified ANC providers. 6 Most pregnant women have access to skilled antenatal care at least once, but globally, only 66% received four prenatal care visits from 2015 to 2021. 2 The lowest levels of antenatal care are observed in South Asia, with only 55% receiving four antenatal care visits, where women living in urban areas are more likely to receive at least four antenatal care visits than those living in rural areas, with an urban-rural gap of 21% points (77% and 56%, respectively).2,4
Although the latest WHO 2016 recommended eight visits for complete ANC visits, Bangladesh country guidelines still promote four or more ANC visits. 7 According to the Bangladesh Demographic and Health Survey (BDHS), the prevalence of ANC visits from any healthcare facility has increased. ANC coverage increased by 31 percentage points from 2004 to 2017 (51%–82%).8-10 The percentage of pregnant women who have four or more ANC visits by any provider increased from 17% in 2004, 8 31% in 2014, 10 and 47% in 2017. 11 And the percentage of urban women is more likely than the percentage of rural women to have made four or more antenatal visits (59% compared with 43%). 11
Nowadays, women attend ANC but do not complete their antenatal visits as recommended following clinical guidelines that put their lives and their babies in danger. Women are essential to the survival of our species globally, but they are often accompanied by potential risks that we need to protect. This can be achieved through proper assessment of mothers during antenatal care. Antenatal care during pregnancy is a universally recognized program. Although several kinds of literature are available related to the utilization of antenatal care visits and pregnancy-related consequences, they used such methods as logistics, multilevel, and so.2,12-14 The use of quantile regression for analysis to determine factors for ANC utilization is limited in Bangladesh. Instructed antenatal care (ANC) during pregnancy is a proven health behavior in reducing maternal mortality and morbidity.
Hence, there is a need to develop a better policy to resolve the factors for incomplete ANC visits, which will help strengthen ANC visits and take appropriate measures to improve maternal health. The main objective of this study is to investigate the factors associated with complete and incomplete ANC visits among women of reproductive age in Bangladesh by analyzing different levels of quantiles. This research will help planners and policymakers understand the issues adjacent to incomplete ANC visits and identify those variables related to incomplete ANC among women of reproductive age in Bangladesh. In addition, we also discussed how to estimate the conditional mean and different quantile functions of a response variable by considering a specific regression model. A research methodology including data source, detailed variables, and data analysis tools are discussed in Section “Material and Methods”. Data analysis and statistical model-based evidence are presented in Section “Data Analysis and Results”. The discussion and conclusions are described in Section “Discussion” and “Conclusion”, respectively.
Materials and Methods
Source of Data
In this research, the secondary dataset was used, which was displaced in the Bangladesh Demographic and Health Survey (BDHS) 2017 and constructed for the urban and rural areas of Bangladesh and each of the eight administrative divisions. This survey was conducted by the National Institute of Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare of Bangladesh, which performed a two-stage cluster sampling.
Study Variables
Outcome Variable
In this study, the number of antenatal care (ANC) visits was considered the outcome variable (Y). The outcome was a categorical variable measured as complete and incomplete antenatal care visits. The greater than or equal to four (≥4) antenatal care visits were defined as complete ANC visits, and less than four (<4) antenatal care visits were defined as incomplete ANC visits during women of reproductive age (15–49) in Bangladesh.
Independent Variables
A set of independent variables associated with antenatal care visits were considered. For this study, independent variables were women's age at delivery (categorized as 15–19 years, 20–24 years, 25–29 years, 30–34 years, 35–39 years, 40–44 years, and 45–49 years), women's educational status (no education, primary, secondary, and higher), birth order number (1, 2–3, 4–5, and 6+), sex of household head (male and female), husband's educational level (no education, primary, secondary, and higher), wealth index (poorest, poorer, middle, richer and richest), the place of residence (urban and rural) and division (Dhaka, Chittagong, Barisal, Sylhet, Rangpur, Khulna, Mymensingh, and Rajshahi).
Regression Analysis
Regression analysis is a set of statistical mechanisms for estimating the relationships between a dependent variable (a set of dependent variables in a multivariate setting) and one or more independent variables. Multiple linear regression (MLR) is simply known as multiple regression and it is a statistical mechanism that used various independent variables to predict the outcome of a dependent variable.
15
The main assumption of MLR is that the relationship between the dependent variables and the independent variables is linear and also the independent variables are not highly correlated with each other. MLR is the extension of ordinary least-squares (OLS) regression because it includes more than one independent variable. Suppose Y be a response variable and


Note that the traditional mean regression provides an ideal location estimation function of a conditional distribution when the conditional-response distribution is symmetric. It is unreasonable for heavy tail conditional response distributions. The mean regression only provides the effect of covariates on the average point of the response variable. It does not analyze the impact of predictors
Quantile Regression Analysis
Quantile regression analysis refers the relationship between an arbitrary quantile of a dependent variable and a set of independent variables. Quantile regression was first introduced by Koenker and Bassett 16 and it provides insight into the non-linear and asymmetric effects of covariates on different quantiles in the conditional response distribution. Median (50% quantile) regression is a specific case of quantile regression, usually preferred for the skewed data set. Although quantile regression analysis is often used to model specific conditional quantiles of the response, the full potential lies in modelling the full conditional distribution. Quantile regression is an extension of mean regression used for any skewed response distributions and bell-shaped distributions.17,18 When the assumptions of the linear regression are not met, quantile regression is used. Quantile regression also has some advantages. 19
The fundamental quantile regression model specifies the conditional quantile as a linear function of independent variables. Let



Data Analysis and Results
Exploratory Data Analysis
Table 1 represented the descriptive statistics of the number of antenatal care visits which was the dependent variable in this study. The total number of women age 15 to 49 years was 5012 of which 2414 women (48.2%) were complete and 2598 women (51.8%) were incomplete antenatal care visits.
Descriptive Result of Complete and Incomplete Antenatal Care (ANC) Visits among Women of Reproductive Age (15–49) in Bangladesh.

In this exploratory section, we presented two crucial covariates that account for complete and incomplete ANC visits. A graphical representation of women's age showed in Figure 1 which strongly suggests that incomplete ANC visits increased more with increasing age than complete ANC visits. Figure 2 showed that women's educational level and wealth index were strongly related to ANC visits. As Figure 2A revealed, women with the lowest education used less ANC visits, while women with the highest education used it more. As shown in Figure 2B, women of higher economic status make fuller used of ANC than women of lower economic status. Other variables can be explained as similarly.
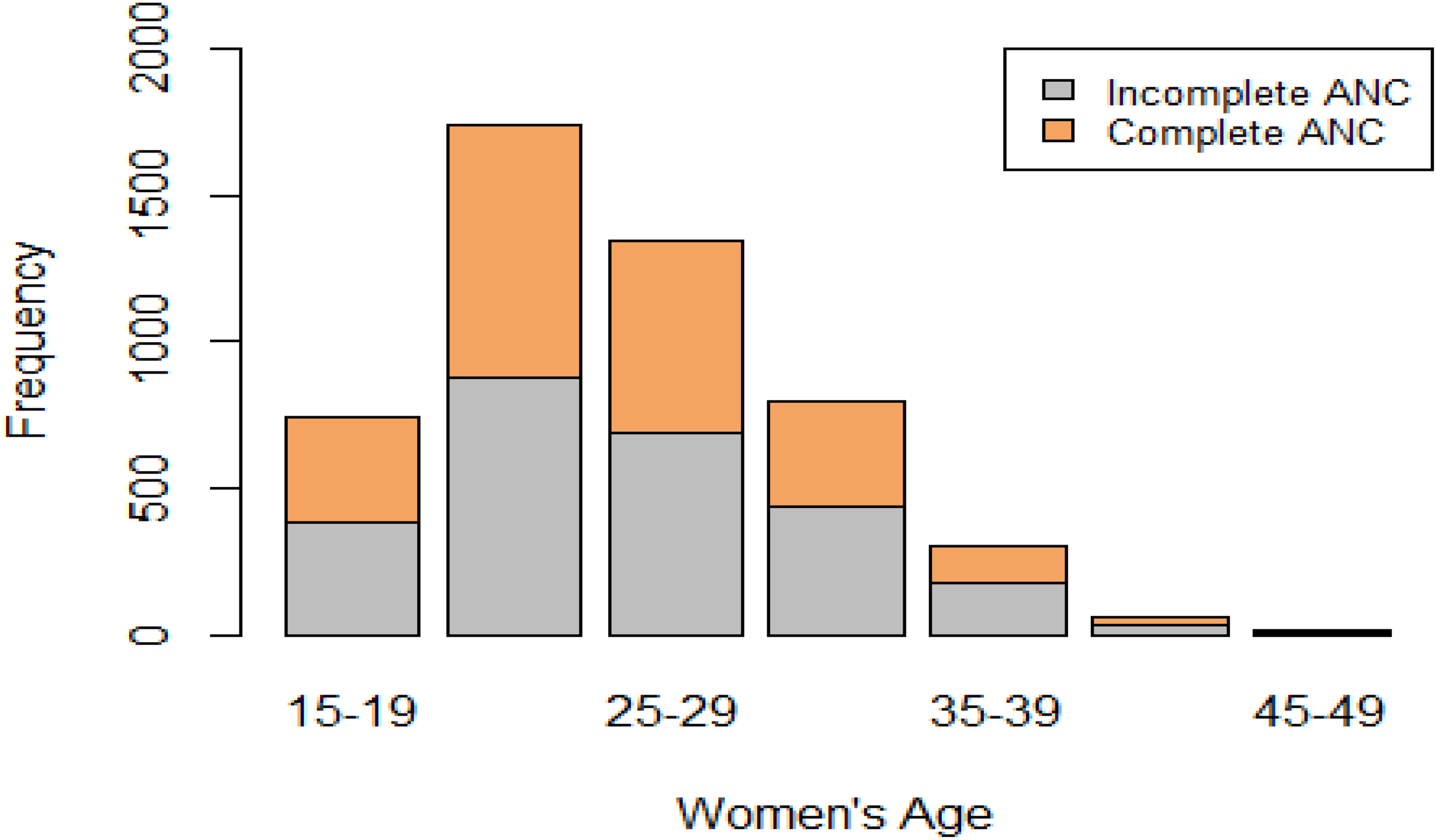
Women's age at complete and incomplete ANC visits.

(A) Women's education level at complete and incomplete ANC visits; (B) Economic status of women in complete and incomplete ANC visits.
The frequency distribution of complete and incomplete antenatal care visits for some socioeconomic and demographic variables illustrated in Table 2. This study included 5012 women from reproductive aged 15 to 49. This result showed that 383(51.27%) of lower women aged incomplete ANC visits, while 6(46.15%) of higher aged women complete ANC visits. It also showed, 249(79.81%) illiterate (no education) women incomplete ANC visits, while 639(70.53%) of highly educated women complete ANC visits.
The Frequency Distribution of Some Socioeconomic and Demographic Variables with Complete or Incomplete Antenatal Care (ANC) Visits among Women of Reproductive Age in Bangladesh.

854 (44.60%) women were incomplete ANC visits for the birth of their first child while 18 (16.82%) women was complete ANC visits for the birth of 6 or more children. Moreover, mothers’ utilization of ANC visits decreased if the number of their children increased.
For the variable sex of household head, 2270 (51.54%) women incomplete ANC visits if the head of the household was male and 280 (46.05%) women complete ANC visits if the head of the household was female.
For husbands’ educational attainment, 524(69.13%) of women with illiterate (no education) husband was incomplete ANC visits and 694(72.14%) of women with highly educated husband was complete ANC visits.
The number of ANC visits increased for higher income households. For example, 746(69.14%) of the poorest women was incomplete ANC visits, while 729(71.26%) of the richest women was complete ANC visits. Rich women had a relatively more percentage of complete ANC visits in comparison to poor women.
The percentage of incomplete ANC visits were 707(40.99%) and 1891(57.53%) for women from urban and rural areas, respectively. So, the result showed that urban women was more aware than rural women of the utilization of ANC visits. Finally, among the eight divisions Barisal, Chittagong, Mymensingh and Sylhet were the most affected by the incomplete ANC visits.
Result of Linear Regression Analysis
A linear regression model was performed separately for both incomplete and complete antenatal care visits. We set two response variables, Y = number of incomplete ANC visits and Y = number of complete ANC visits, and women's age, women's educational level, birth order, sex of household head, husband's educational level, wealth index, place of residence and division were independent variables. For only the relationship between the average of a response variable and covariates exploration purposes, the summary results of mean regression analysis were tabulated in Tables 3 and 4. The basic theory of mean regression analysis is mentioned in Section “Regression Analysis”.
The Summary Statistics of Quantile Regression for Incomplete Antenatal Care Visits with β = (0.25,0.50,0.75).

Note: ref=categorical reference.
The Summary Statistics of Quantile Regression for Complete Antenatal Care Visits with β = (0.25,0.50,0.75).
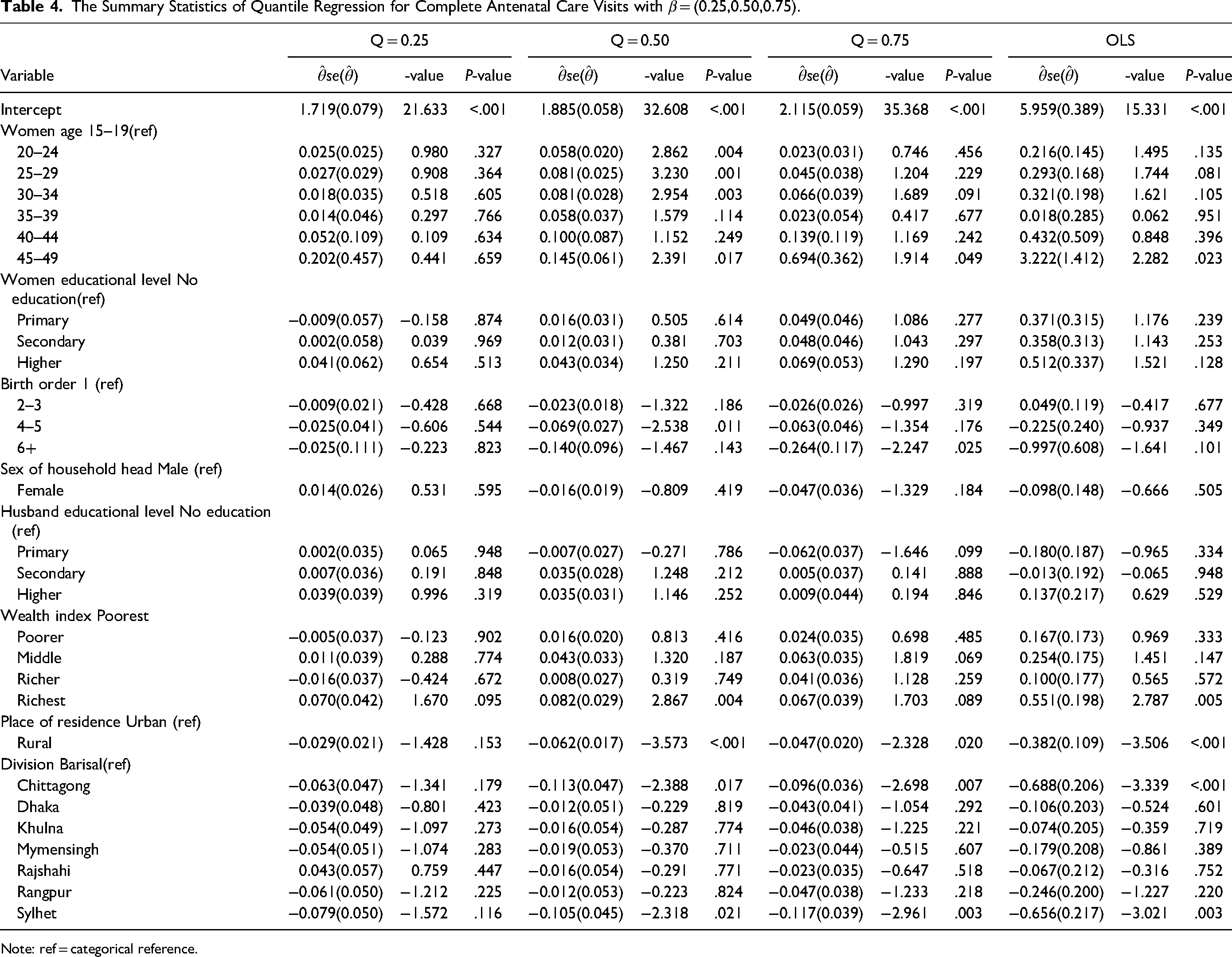
Note: ref = categorical reference.
The OLS result revealed that there was a relationship between incomplete ANC visits and other demographic and socioeconomic variables. For the variable women's age, there was a positive relationship except for the age group (45–49) and had a significant effect (except for the age group (20–24), (40–44), and (45–49)) with incomplete antenatal care visits at 5% level of significance. For the variable women's educational level showed a positive relationship among all categories (primary, secondary, and higher) and had a highly significant was observed when compared to the reference category. The slope coefficient of the birth order number (1, 2–3, 4–5, and 6+) was negative which indicates that there was a statistically significant negative relationship with incomplete antenatal care visits. The sex of the household head variable indicated a strong negative relationship with incomplete antenatal care visits.
For the husband's educational level, this variable indicated a positive relationship and was highly significant except for the primary level. For the variable wealth index (poorest, poorer, middle, richer, and richest), there was a positive relationship and highly significant except for the poorer group. For the place of residence among the urban and rural, there was a statistically significant negative relationship with incomplete antenatal care visits. For the variable division (Barisal, Chittagong Dhaka, Khulna Mymensingh, Rajshahi Rangpur, Sylhet), there was a positive relationship and had a significant effect except for Barisal, Chittagong, and Khulna with incomplete antenatal care visits.
On the other hand, the results of using OLS for complete ANC visits showed that for the variable women's age, there was a positive relationship with the complete antenatal care visits and all regression coefficients were not significant (except for the age group (45–49)) at 5% level of significance. For the variable women's educational level showed a positive relationship among all categories (primary, secondary, and higher), and no significant was observed when compared to the reference category. The slope coefficient of the birth order number (1, 4–5, and 6+) was negative which indicates that there was a negative relationship in all except birth order (2–3). The sex of the household head variable indicated a strong negative relationship with the complete antenatal care visits.
For the husband's educational level, this variable also indicated a negative relationship but no significant was observed. For the variable wealth index (poorest, poorer, middle, richer, and richest), there was a positive relationship and no significant except for the richest group. For the place of residence among the urban and rural, there was a statistically significant negative relationship with the complete antenatal care visits. For the variable division (Barisal, Chittagong Dhaka, Khulna, Mymensingh, Rajshahi, Rangpur, Sylhet), there was a strong negative relationship and no significant except for Sylhet with the complete antenatal care visits.
Result of Quantile Regression Analysis
The number of antenatal care visits was selected for regression analysis as a response variable. For the analysis, we first tested the linearity assumption between the covariate and the response variable to determine whether there was a non-linear relationship between the covariate and the response variable. Note that this response variable was a countable and a non-negative number. Hence, this variable was not suitable for the quantile regression analysis. 16 Therefore, the transformation of the response variable added a 1.1 value that did not affect the final results due to sharing equivariance properties. 17
In quantile regression analysis, we focused on the estimation of the conditional quantile of the response variable Y given demographic and socioeconomic variables by using the model (2). Quantile regression analysis was performed to find the impact of those covariates on the 25%, 50%, and 75% quantile levels of the response variable. Tables 3 and 4 were presented the summary statistics of quantile regression estimates of 25%, 50%, and 75% quantiles for the incomplete and complete number of antenatal care visits.
For the variable women's age, there was a positive relationship with the incomplete antenatal care visits except for the age group (45–49) at 50% quantile and age group (35–39) at the 75% quantile. For the variable women's educational level showed a positive relationship among all categories (primary, secondary, and higher) and had a significant effect at all three levels of quantiles.
Birth order number (1, 2–3, 4–5, and 6+) indicated a strong statistically significant negative relationship at all levels of quantiles. The sex of the household head variable indicated a strong negative relationship with incomplete antenatal care visits. For the husband's educational level, this variable indicated a positive relationship and had a highly significant effect at all three levels of quantiles with incomplete antenatal care visits. For the variable wealth index (poorest, poorer, middle, richer, and richest), there was a positive relationship and had a highly significant effect with incomplete antenatal care visits at all levels of quantiles. For the place of residence variable, there was a strong negative relationship with incomplete antenatal care visits at all levels of quantiles and had a highly significant effect at the 75% quantile but not lower 25% and 50% quantiles. For the variable division (Barisal, Chittagong, Dhaka, Khulna Mymensingh, Rajshahi Rangpur, Sylhet), there was a positive relationship with incomplete antenatal care visits at all levels of quantile and had a significant effect but not 25% quantile for Dhaka and Sylhet, 50% quantile for Mymensingh and 75% quantile for Dhaka and Rajshahi.
On the other hand, for the variable women's age, there was a positive relationship with the complete antenatal care visits and all coefficients were not significant except for the age group (20–24), (25–29), (30–34), and (45–49) at the 50% quantile and age group (45–49) at the 75% quantile. For the variable women's educational level showed a positive relationship among all categories (primary, secondary, and higher) except the primary level at the 25% quantile. Birth order number (1, 2–3, 4–5, and 6+) indicated a strong negative relationship and not a significant effect except for birth order number (4–5) at 50% quantile and (6+) at 75% quantile. The sex of the household head variable indicated a strong negative relationship with complete antenatal care visits. For the husband's educational level, this variable also indicated a positive relationship except for the primary level at 50% and 75% quantiles. For the variable wealth index (poorest, poorer, middle, richer, and richest), there was a positive relationship except for the richer group at 25% quantile. For the place of residence (urban and rural), there was a strong statistically significant negative relationship with complete antenatal care visits but, at the lower quantiles (25%), it was not observed. For the variable division (Barisal, Chittagong Dhaka, Khulna Mymensingh, Rajshahi Rangpur, Sylhet), there was a strong negative relationship with complete antenatal care visits at 25%, 50%, and 75% quantiles.
Discussion
This study attempted to explore the influence of demographic, socioeconomic, and health-related factors on complete and incomplete antenatal care visits among women of reproductive age (15–49) in Bangladesh using mean regression and quantile regression analysis. Using BDHS-2017 data, we analyzed separately for complete and incomplete antenatal care visits and finally compared both models. Many studies in previous have commonly used standard linear regression and logistic regression. Sometimes the assumption of linearity is not met, then if we use linear regression (LR) it may produce a misleading result so we used the quantile regression method to recover it. The main focus was on a quantile regression approach to investigate the effects of demographic, socioeconomic, and health-related factors on the utilization of antenatal care visits at different quantiles. Before doing quantile regression we tried mean regression (OLS). Independent variables that were significant at a 10% significance level were taken as candidate variables for mean regression.
According to OLS analysis, we found that women's ages, women's education level, and wealth index have a positive relationship with the complete ANC visits and a negative relationship with birth order, sex of husband head, husband's education level (except higher), residence, and division. On the other hand, incomplete ANC visits have a negative relationship with higher women's age, birth order, sex of husband head, and residence, and a positive relationship with women's age, women's education level, husband's education level, residence, and division.
Investigating the covariate effect at different response quantiles is important as the relationship may be different at different quantile levels of the response. Not only the relationship but also the significance of this relationship may vary with different quantiles of response. For example, for the complete ANC visits in this study, the higher women's age (45–49) was insignificant at 25% quantiles while significant for 50% and 75% quantiles. On the other hand, for incomplete ANC visits, the higher women's age (45–49) was highly significant at 25% quantiles while insignificant for 50% and 75% quantiles.
Similarly, for the complete ANC visits in this study, the women's educational level was insignificant at 25%, 50% and 75% quantiles. On the other hand, for incomplete ANC visits, the educational level of women in 25%, 50% and 75% quantiles were highly significant. This result showed that educational attainment was the most responsible for ANC visits being completed or incomplete. Many studies support these findings.2,12 These findings are realistic as education is a potential means of acquiring knowledge and highly educated women realize the importance of ANC visits during pregnancy.
The analysis identified that birth order is one of the strongest determinants of complete and incomplete ANC visits. The result suggested that complete and incomplete ANC visits have a negative relationship and highly significant for all three quantiles for incomplete ANC visits. Fear of miscarriage and high excitement of being pregnant for the first time, the frequency of ANC visits during pregnancy is high. The result of the wealth index showed that economical status influences incomplete ANC visits during pregnancy. So, we have to ensure complete ANC visits of lower economic pregnant women. Place of residence and division also found significant effects at different quantile levels.
Quantile regression analysis for 50% and 75% quantiles found that Chittagong and Sylhet have a significant for complete ANC visits. However, for incomplete ANC visits, there have a significant on Khulna, Mymensingh, Rajshahi, and Rangpur at 25% quantile, Khulna, Rajshahi, Rangpur, and Sylhet at 50% quantile, and Chittagong, Rangpur and Sylhet at 75% quantile. It varies geographically. So, it is important that it needs immediate attention. This study has some limitations in the analysis due to the use of secondary data. Cross-section data was used for this study.
Conclusions
The main purpose of this article is to predict the factors which are responsible for incomplete antenatal care visits among women of reproductive age in Bangladesh. ANC visits play a vital role in reducing maternal mortality and morbidity. The results of this study found that complete or incomplete antenatal care visits have mainly associated with women's age, women's educational level, birth order number, sex of household head, husband's educational level, wealth index, place of residence and also varied geographically (division) at different levels of quantiles. This study strongly supports that women who are more educated are more likely to have complete ANC visits and less educated women are more likely to have incomplete ANC visits. Overall, women's educational attainment plays a significant role in antenatal care visits. Similarly, economical status is also a vital barrier to the utilization of ANC visits. Barriers to education and economic support should be identified and addressed and it can be reduced by increasing women's education and financing the health sector through insurance policies or organizations. This study suggests an emphasis on women's education, especially in rural areas of Bangladesh. For increased utilization of ANC visits, special focus should be placed on divisions. The appropriate utilization of ANC visits during pregnancy will be reduced the risk of child malnutrition and death, maternal mortality and morbidity.
Footnotes
Authors Contributions
Md. Rezaul Karim is supervised the process of study. Anis Mahmud collected the data, analyzed and interpreted the results. Mst. Bithi Akter tabulated the results and wrote the final draft of the manuscript. Md. Rezaul Karim revised the manuscript and finally approved the manuscript before submission. All authors read and approved the final manuscript.
Data and Code Availability
The data sources are provided the Section “Materials and Methods”. We will provide the data, and R code if anyone needs it.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Committee Approval
The study received ethics approval from The Demographic and Health Surveys (DHS) Program (Approval date: June 02, 2022; Approval number: 169645).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article