
Abstract
Objective
To estimate the impact COVID-19 pandemic on healthcare resource utilization (HCRU) among individuals with major depressive disorder (MDD).
Method
A retrospective cohort study was conducted to compare HCRU in the twelve months prior to and six months following pandemic onset among 1,318,709 individuals with MDD and propensity-score matched controls. Outcomes were monthly rates of all-cause and MDD-specific outpatient, inpatient, and prescription medication HCRU. Piecewise random effects models were used to adjust for patient-level clustering, trends over time, and pre-pandemic factors.
Results
In the first month following onset, outpatient HCRU declined with primary care visits down 25.1%. Following this initial decline, outpatient HCRU increased, exceeding pre-pandemic rates within three months. By April 2020, three quarters of all psychotherapy sessions were delivered by telehealth, followed by psychiatry (62.3%), and primary care visits (30.1%). The use of telehealth remained highest for psychotherapy and psychiatry (representing 67.6% and 54.2% of visits, respectively, in September 2020). All-cause partial-day hospitalizations declined 50.5% and remained depressed through July 2020 (down 18.3%). Beginning in the first month post-onset, prescription medication HCRU increased for all antidepressant and antipsychotic medication classes: serotonin modulators ( + 11.8%), bupropion ( + 10.4%), SSRIs ( + 9.0%), SNRIs ( + 8.6%), and atypical antipsychotics ( + 7.5%).
Conclusions
Following pandemic onset, individuals with MDD realized an immediate, but short-lived, reduction in primary care HCRU. Telehealth use remained elevated through the first six months. The most significant and sustained reduction in HCRU was noted for partial-day hospitalizations and all-cause ED visits.
Highlights
During the pandemic, individuals with MDD realized an immediate increase in both psychiatry visits and psychotherapy sessions.
Both psychiatric care and psychotherapy providers rapidly adopted telehealth, with elevated use continuing through the first six months of the pandemic.
During the pandemic, partial-day hospitalizations declined 50.5% and remained depressed through July 2020 (down 18.3%).
Antidepressant and oral atypical antipsychotic use increased and remained elevated through the first six months of the pandemic.
Introduction
Following the COVID-19 pandemic’s onset in the United States, behavioral healthcare providers implemented practice changes to reduce the risk of COVID-19 infection among patients and staff, which included reduced office hours, limited patient volume, physical distancing requirements, and delivery of services via telehealth rather than in person.1–6 At the same time, individuals were reporting worsening mental health, with significant increases in stress, anxiety, depression, and worry.7–9 Individuals who entered the pandemic period with pre-existing disorders, such as major depressive disorder (MDD), reported worsening symptoms 10 and higher rates of anxiety 11 following the pandemic’s onset.
Even in the absence of a pandemic, research indicated that individuals with MDD use substantially more all-cause healthcare services than similar individuals without MDD 12 and that utilization of MDD-specific healthcare services increased with illness severity. 13 As a result, the COVID-19 pandemic has posed unique challenges for individuals with MDD. Without a regular schedule of visits to manage MDD, a provider’s ability to deliver ongoing psychotherapy and supportive management may be compromised. This retrospective research study was conducted to estimate the impact of the COVID-19 pandemic on outpatient, inpatient, and prescription medication healthcare services resource utilization (HCRU) in individuals with MDD by comparing utilization in the six-month period post-onset with pre-pandemic levels.
Methods
The research protocol was approved and granted a waiver of consent by the Advarra Institutional Review Board.
We conducted a retrospective cohort study among adults with MDD and a propensity-score matched historical cohort to assess changes in HCRU associated with the COVID-19 pandemic onset in the United States (U.S.).
Eligible study participants were identified and selected from the Real-World Data Repository, licensed from Clarivate™, an open dataset (ie, that does not include insurance benefits eligibility) of submitted and remitted medical and pharmacy claims. The dataset includes records for more than 300 million Americans, from more than two million healthcare providers and an estimated 98% of payers, including Medicare, Medicaid, commercial plans, and Veterans Affairs.
Eligible adults had at least two outpatient claims associated with International Classification of Diseases (ICD)-10-CM code (F32.x; F33.x) submitted 30-days or more apart or one inpatient claim with the code in the primary position; and had at least one medical or pharmacy claim (for any service or medication) in each calendar quarter of the case-finding and follow-up periods. Individuals were deemed ineligible if diagnosed with bipolar depression (F31.x) or if selected for both the COVID-19 and Control cohorts.
For the COVID-19 cohort, the case-finding period was the twelve-month period prior to the index date; the follow-up period was the six-month period following the index date. The index date in the U.S. was defined for each state and the District of Columbia as the date the infection rate reached 10 per 1,000,000 population, as obtained from the New York Times’ GitHub location. 14 Index dates varied between March 6, 2020 (Washington) to March 28, 2020 (West Virginia). For Controls, the case-finding period was the twelve-month period corresponding to the state-specific index date applied to the prior year, covering March 2018 through March 2019.
Independent Variables
Patient-specific variables included age, gender, insurance, region, Charlson Comorbidity Index (CCI), 15 select medical (hypertension, lower back pain, hyperlipidemia, COPD) and psychiatric (mood disorders, schizophrenia, psychosis, and anxiety, alcohol or substance-related disorders, sleep-wake disorders) comorbidities. Socioeconomic characteristics were obtained by assigning patients to a county of residence and linking, by county, to the 2019 Area Health Resources File and included race, ethnicity, median household income, poverty rate, unemployment rate, population density, education (% percentage who completed high school), and health care access (number of primary care physicians and number of mental health providers per capita).
Outcomes
Outcomes included measures of outpatient, prescription medication, and inpatient HCRU measured per patient per month (PPPM). Acute outpatient services utilization included all-cause emergency department visits, all-cause partial-day hospitalizations, and all-cause and MDD-specific inpatient hospitalizations. Non-emergency outpatient services measures included primary care visits; psychiatry visits (including addiction medicine, behavioral neurology and neuropsychiatry, forensic psychiatry, psychosomatic medicine, psychiatry, and geriatric psychiatry); and psychotherapy sessions (CPT codes 90 832, 90 834, 90 837, 90 839, 90 840, 90 845, 90 847, 90 849, 90 853, 96 152). For non-emergency outpatient services, rates were calculated separately for overall, in-person visits, and visits conducted via telehealth. Medication use was calculated for atypical antipsychotics and antidepressants (ADTs), overall and by therapeutic class, and was measured by count of pharmacy claims, overall and by days’ supply dispensed (< 90 days’ supply vs ≥90 days’ supply).
Propensity Score Matching
The COVID-19 and Control cohorts were matched using a propensity score at a 1:1 ratio with the greedy matching approach and calipers of width equal to 0.02. The propensity score was derived from the case-finding periods and included the characteristics listed in the “Independent Variables” section. Among the 1,484,641 eligible COVID-19 cases and 1,367,005 controls, a total of 165 932 individuals were not matched, resulting in 1,318,709 individuals who were matched and included in the analysis. The magnitude of differences between select variables after matching was assessed using standardized mean differences, calculated as the difference between the estimates in the COVID-19 and Control cohorts divided by the pooled standard deviation.
Statistical Analysis
In the exploratory analysis, time-invariant variables were assessed by completeness and distribution. Outcome measures and other variables expected to vary with time (eg, average psychotherapy visits) were calculated by month across the study period. Trends in healthcare utilization were conducted and year-over-year unadjusted percentage changes were assessed from December 2018-September 2020. Results were calculated starting from 90 days prior to the pandemic index date until 180 days following the pandemic index date of each cohort and converted to per thousand patients per month (PkPPM) measures.
Patient-level piecewise random effects models were used to assess differences in healthcare use between the pandemic Cohort and Controls during the period from March-April 2020 through August-September 2020 while adjusting for patient-level clustering, trends over time, and baseline outcome values. The exploratory analysis revealed a critical junction at June-July 2020 after which utilization for the pandemic Cohort seemed to approach pre-pandemic levels. Due to the nonlinear trend over time, a time spline variable was used to fit the piecewise model. The spline had a value of 0 for the “peak” pandemic period (from March-April through May-June), 1 for June-July, 2 for July-August, and 3 for August-September. Separate models were run for each of the outcomes (dependent variable) defined above. For non-emergency outcomes (eg, outpatient visits), the model used a Poisson distribution and log link with the outcome constructed as number of visits per month. Due to the less frequent occurrence of emergency services (eg, MDD inpatient admissions) and prescriptions per month, emergency and prescription medication outcomes used a binomial distribution and log link with 1/0 indicators constructed for each outcome.
All data management and statistical analyzes were performed with SAS version 9.4 (Cary, NC).
Results
Among the 1,318,709 eligible individuals in the COVID-19 cohort, nearly 70.2% were female with an average age of 57.8 years (SD: 18.2 years), and 35.2% had commercial insurance, followed by 34.2% with Medicare, and 30.3% with Medicaid. The sample included individuals from all 50 states and the District of Columbia. The average CCI was 2.0 (SD: 2.4) and the most common psychiatric comorbidity was anxiety, affecting 57.9% of the population, followed by sleep-wake disorders (28.8%) and alcohol or substance use disorder (24.8%).
Comparison with Unmatched Sample
As noted earlier, 165 932 individuals with MDD (11.1%) who met preliminary eligibility criteria for the COVID-19 cohort were not successfully matched to an historical control. Compared to the population successfully matched, these individuals were significantly younger (49.8 vs 57.8 years; p < .01), more likely to be insured by a commercial plan (53.8% vs 35.2%; p < .01), had lower CCI scores (1.5 vs 2.0; p < .01), but had substantially higher rates of anxiety (73.4% vs 57.9%; p < .01), alcohol or substance use disorder (26.9% vs 24.8%; p < .01), and sleep-wake disorders (31.3% vs 28.8%; p < .01).
Outpatient Care Services
In the three months preceding the index date (December 2019 through February 2020), the COVID-19 cohort had higher use of psychiatry and psychotherapy (overall, including in-person and telehealth-delivered); a difference that increased steadily (Figure 1). By February 2020, the COVID-19 cohort realized a 43.9% increase in psychotherapy sessions, followed by a 15.0% increase in psychiatry visits, and a 2.0% decrease in primary care visits compared to Controls. In the first month of the pandemic (March/April 2020), primary care visits declined substantially (down 25.1%). Increases were noted for psychotherapy sessions (up 31.0%), and psychiatry visits (up 11.3%). By May/June, the total visit rate increased for all outpatient services.

Percent year-over-year change by month for select all-cause primary and mental health care services.
Telehealth Services
Changes in outpatient HCRU were driven by a sharp decline in in-person visits and increase in telehealth visits (Figure 2). Telehealth-delivered HCRU peaked in April 2020, with around three quarters of all psychotherapy sessions delivered via telehealth, followed by psychiatry (62.3%), and primary care visits (30.8%). Through August/September 2020, the use of telehealth remained highest for delivery of psychotherapy (representing 67.6% of all sessions) and for psychiatry (representing 54.2% of all visits). The proportion of primary care visits delivered via telehealth declined steadily from May through September 2020 at which time only 11.5% were delivered via telehealth.
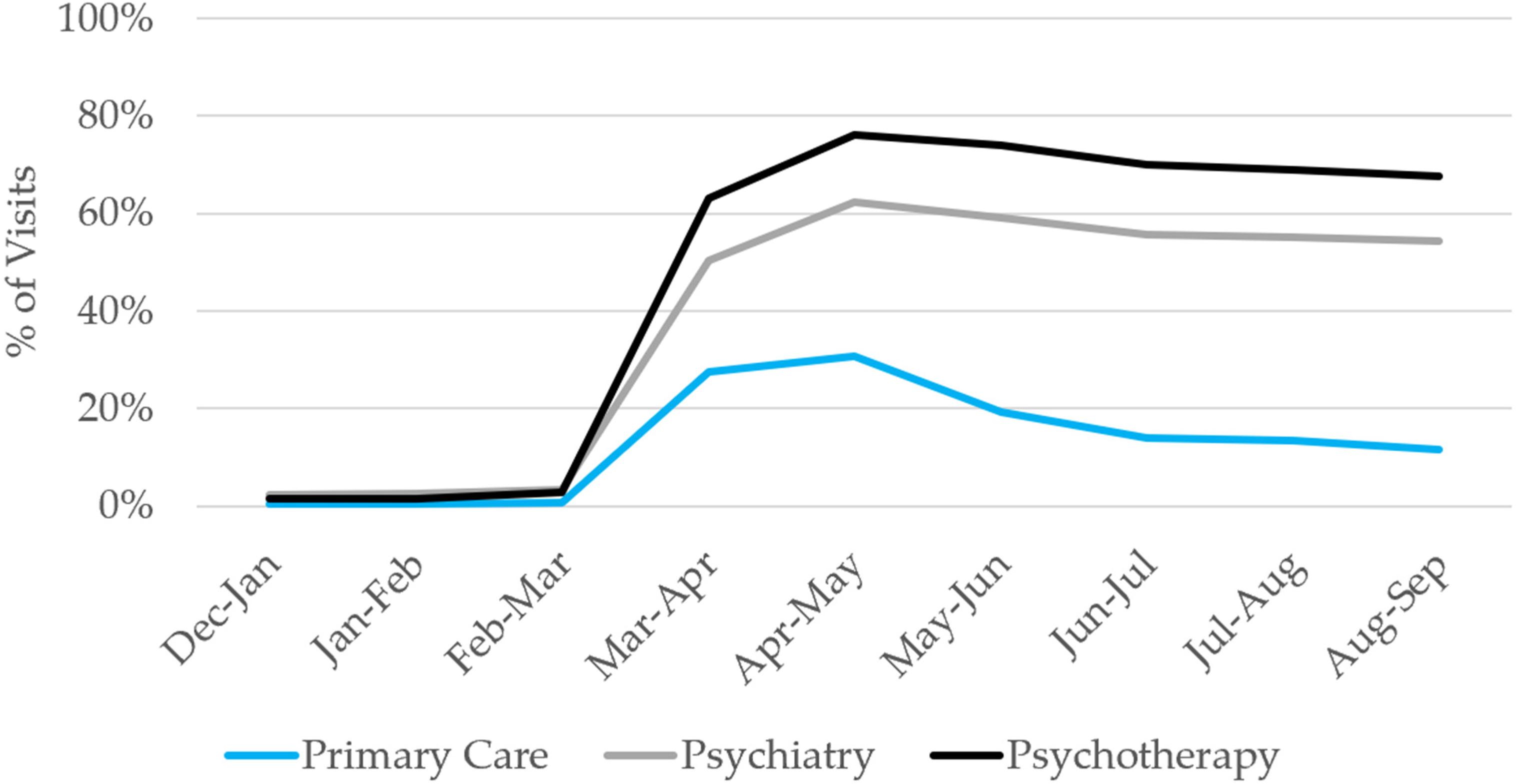
Percent of visits delivered via telehealth, by provider and location, December 2019 – September 2020, COVID-19 cohort only.
Prescription Medication Use
Year-over-year, the utilization of ADTs increased steadily during the first three months of the pandemic (Figure 3). Each therapeutic class realized a significant increase in total days’ supply, with the increase in August/September 2020 highest for serotonin modulators (up 11.8%), followed by bupropion (up 10.4%), Selective Serotonin Reuptake Inhibitors (SSRIs) (up 9.0%), Serotonin and Norepinephrine Reuptake Inhibitor's (SNRI's) (up 8.6%), antipsychotics (up 7.5%), alpha-2 antagonists (up 6.3%), and tetracyclics/tricyclics (up 5.0%). At the claim level, increases were noted in the proportion of individuals on an ADT, in the number of ≥90 days’ supply claims processed, and in the number of 30 days’ supply claims processed.

Percent Year-Over-Year Change by Month for Select Acute Care Services.
Acute Care Services
Post-pandemic onset changes in all-cause acute care services utilization varied by type of service (Figure 4). All-cause hospitalizations and Emergency Department (ED) visit rates declined by 16.8% and 33.7% in March/April 2020. All-cause ED visits remained below pre-pandemic levels through August/September (down 5.6%), while all-cause hospitalization increased steadily, up by 8.0% over pre-pandemic levels by August/September 2020. In contrast, both MDD-specific hospitalizations at a short-term acute care hospital and all-cause inpatient hospitalizations at a psychiatric facility increased following pandemic onset and remained elevated throughout the first six months, up 53.6% and 38.5% by August/September 2020, respectively. The most sustained decline in acute HCRU was for all-cause partial-day hospitalizations, which declined by 50.5% and remained down through July/August (down 18.3%).

Year-Over-Year Change in Prescription ADT and Antipsychotic Total Days’ Supply by Month.
Multivariate Comparisons
Random effects models, adjusted for patient clustering, trends over time, and baseline healthcare utilization, were consistent with the findings described above (Table 1).
Random Effects Piecewise Models for Service Utilization Comparing Pandemic and Pre-Pandemic Cohorts in Follow-Up Period.
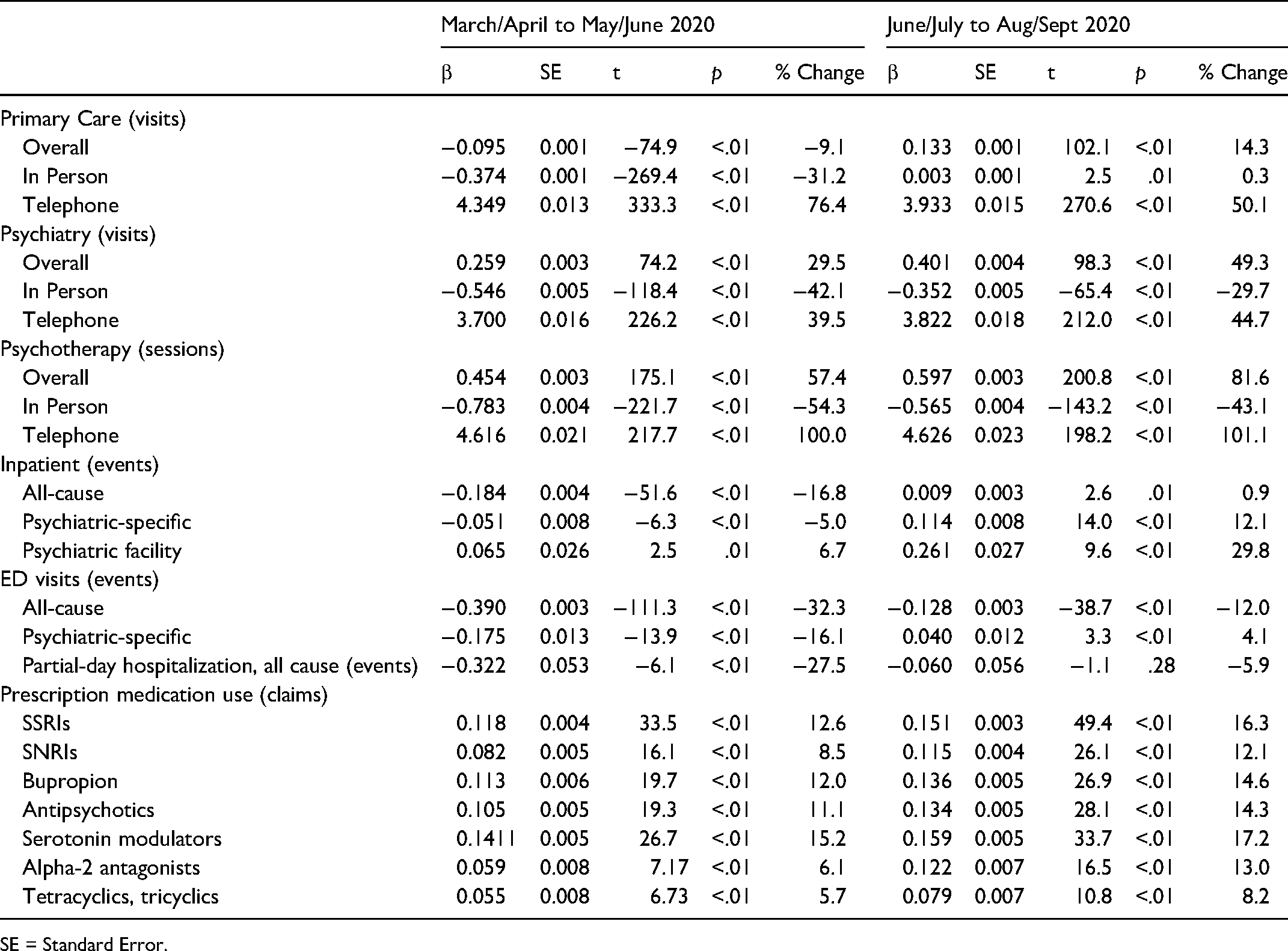
SE = Standard Error.
In the first three months of the pandemic (March/April through May/June 2020), utilization of primary care declined while utilization of psychiatry and psychotherapy services increased, with all realizing a substantial decline in in-person visits and increase in telehealth visits.
In the second three-month period (June/July through August/September), primary care visits, psychiatry visits, and psychotherapy sessions increased substantially. All-cause ED visits and partial-day hospitalizations were lower through the first three months of the pandemic while psychiatric-specific ED visits initially declined but then recovered in the second three-month period. Prescription medication use of all ADT classes and antipsychotic medications realized significant increases throughout the post-pandemic onset period.
Discussion
Our study documented that the COVID-19 pandemic profoundly impacted the HCRU among individuals with MDD. Primary care HCRU declined substantially in the first few months of pandemic onset, but rates recovered quickly, exceeding pre-pandemic levels by June 2020. Psychotherapy services, and to a lesser extent, psychiatry visits increased substantially, driven by a rapid and widespread adoption of telehealth services. HCRU associated with acute care services followed a somewhat different pattern. All-cause partial-day hospitalizations and all-cause ED visits declined substantially and remained low throughout the initial six months of the pandemic. All-cause inpatient hospitalizations at a psychiatric facility and at short-term acute care hospitals did not show a meaningful decline before increasing substantially. Similarly, antidepressant medication use increased following pandemic onset. Finally, outpatient providers rapidly transitioned to telehealth in the early months of the pandemic in the U.S.; however, primary care providers more rapidly returned to in-person visits compared to mental health care providers.
Outpatient Care
In the first two months following pandemic onset, utilization of primary care services declined, with utilization recovering by June 2020. In contrast, rates of both psychiatry visits and psychotherapy sessions increased immediately and persisted through the first six months of the pandemic in the U.S. This increase in psychiatric and psychotherapeutic outpatient care is likely driven by both an increase in symptom severity and the rapid adoption of telehealth-delivered services. The overall increase in telehealth observed in this study is consistent with other reports documenting a substantial increase overall.3,16
Of note, the telehealth designation in claims covers services delivered via both audio-only and video. Satisfaction with telehealth services is higher when the interaction includes video and is higher among individuals with higher levels of eHealth literacy, defined broadly as the ability of a consumer to seek out, evaluate, and apply health-related information from electronic information sources.17,18 Given the ongoing use of telehealth services to deliver behavioral health services, eHealth literacy will likely be a critical issue for mental healthcare providers. It’s likely that access to, use of, and satisfaction with telehealth services varied significantly across individuals and populations.
Inpatient and Partial Day Hospitalizations
The most dramatic decline in outpatient psychiatric care services, however, occurred in all-cause partial-day hospitalizations, an intensive outpatient care service that is delivered in person to individuals with acute psychiatric symptoms. To our knowledge, this is the first study to document a reduction in utilization of partial-day hospitalizations during the first 6 months of the pandemic in a cohort of patients with MDD. Though we did not evaluate the underlying psychiatric condition leading to partial hospitalization, it’s likely that these services are provided for an array of psychiatric illness, not just symptoms of MDD. 19 Further, though virtual partial hospitalization programs are uncommon, Bulkes, et al 20 reported that outcomes associated with a virtual partial hospitalization program were comparable to those of a traditional in-person partial hospitalization program.
Additionally, these changes are in stark contrast to changes in inpatient hospitalizations for psychiatric care, which realized a modest decline initially but rapidly increased and exceeded pre-pandemic levels by more than 20% by August/September 2020, perhaps supporting the likely difference in symptom severity between those occupying partial day beds and those admitted to inpatient psychiatric care. The elevated use of inpatient psychiatric hospitalizations may reflect the combined risk of serious and significant impact of the COVID-19 pandemic on mental health, 21 perhaps exacerbating severe psychiatric symptoms including increased risk of suicidality, 22 changes in effectiveness of outpatient services, or as an alternative to partial-day hospitalizations which were less available.
Regardless of the drivers, elevated psychiatric hospitalization emerged as one of the indirect results of the pandemic. Management of otherwise unnecessary cost associated with elevated hospitalizations is a longstanding goal of managed care. More research is required to improve our understanding of the pandemic’s effect on the delivery channels for psychiatric services and how post-pandemic ambulatory service and pharmacy utilization results contribute to utilization of high-cost services and clinical outcomes.
Finally, our results indicated an increase in both the number of claims and total days’ supply filled for antidepressant and antipsychotic prescription medications. The United Kingdom’s National Health Service reported similar findings, noting a 3.9% increase in prescription antidepressants between April 1 and September 30, 2020. 23 In this study population, an increase in the proportion of individuals with MDD receiving ADTs was noted and included increases in both 30-day and 90-day supply prescriptions. In contrast, in a Canadian study of community-based pharmacies, Uthayakumar et al, 24 reported an initial decline followed by a rapid return to pre-pandemic antidepressant dispensing rates.
Strengths and Limitations
The primary strength of the study is the generalizability to the U.S. population of individuals with MDD. Results are derived from a large, real-world sample of more than 1.3 million adults with MDD who sought healthcare services, a population with diverse demographic characteristics, who reside in urban and rural communities, and are insured by public and private insurers.
This study is subject to the limitations of administrative claims data: coding errors that include under-coding, over-coding, not coding at the highest level of specificity, and unbundling. Pharmacy claims only include prescriptions purchased but may not include all medications that were prescribed or consumed. Further, the rapid introduction of reimbursement for telehealth services likely led to challenges with accurate coding. Of more importance, administrative data provide no insights into why changes in utilization occurred. Changes in utilization may be associated with loss of health insurance coverage, 25 state and local policies restricting movement, 26 concerns about infection risk, 27 and disruptions to mental health services. 28
Conclusions
Individuals who entered the pandemic with MDD realized an immediate increase in psychiatry visits and psychotherapy sessions, associated with a rapid transition to telehealth-delivered services. There was no evidence of an interruption in medication use. These promising outpatient results were offset by evidence of a challenge with acute care services, specifically a sustained reduction in partial-day hospitalizations and increase in psychiatric hospitalizations.
Footnotes
Acknowledgments
The authors wish to acknowledge the administrative support of Margaret L. Stinstrom in the preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs. Bhattacharjee, Rothman, and Kulkarni are employees of Otsuka Pharmaceutical Development & Commercialization, Inc who funded the study. Ms. Felicia Forma was a former employee of Otsuka Pharmaceutical Development & Commercialization, Inc. Drs. Liberman, Ruetsch, and Ms. Rui are employees of Health Analytics, LLC which was funded to conduct the study.
Disclosures
Drs. Bhattacharjee, Rothman, and Kulkarni are employees of Otsuka Pharmaceutical Development & Commercialization, Inc who funded the study. Ms. Felicia Forma was a former employee of Otsuka Pharmaceutical Development & Commercialization, Inc. Drs. Liberman, Ruetsch, and Ms. Rui are employees of Health Analytics, LLC which was funded to conduct the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Otsuka Pharmaceutical Development & Commercialization, Inc,