
Abstract
Background:
Chronic noncancer pain (CNCP) and chronic opioid therapy (COT) commonly coexist with comorbid depression and anxiety. We investigated the prevalence of depression and anxiety and their correlates at the time of controlled substance agreement (CSA) enrollment among patients with CNCP and a history of depression or anxiety on COT.
Methods:
Retrospective analysis of 1066 patients in a Midwest primary care practice enrolled in CSAs for COT between May 9, 2013, and August 15, 2016. Patients with self-reported symptoms or a clinical history of depression or anxiety were screened at CSA enrollment using the Patient Health Questionnaire–9 item scale and the Generalized Anxiety Disorder–7 item scale.
Results:
The percentage of patients screening positive for depression and anxiety at CSA enrollment was 15.4% and 14.4%, respectively. Patients screening positive for depression or anxiety were more likely to be younger, unmarried, unemployed, and live alone compared to patients not screening positive. Patients screening positive for depression or anxiety were more likely to smoke cigarettes and report concern from friends or relatives regarding alcohol consumption. Compared to patients screening negative, patients screening positive for depression had higher odds of receiving opioid doses of ≥50 morphine milligram equivalents per day (adjusted odds ratio: 1.62; 95% confidence interval: 1.01-2.58).
Conclusion:
Anxiety and depression are prevalent at enrollment in CSAs among patients receiving COT. Future research is needed to determine whether recognition of anxiety and depression leads to improved management and outcomes for this population.
Keywords
Introduction
Chronic noncancer pain (CNCP) is a prevalent and complex clinical problem. 1 Over 25 million patients experience daily CNCP, 2 and pain represents one of the most common indications for which patients visit their doctors annually. 3 Chronic opioid therapy (COT), defined as opioid use greater than 90 days 4 has increasingly been utilized to manage CNCP, but evidence for long-term efficacy is limited. 5 Chronic opioid therapy is associated with health risks including abuse and overdose. 6 The increasing availability of opioids and associated risks necessitate understanding the characteristics of patients receiving COT for CNCP. 7
Mental health conditions such as major depressive disorder (MDD) and anxiety are prevalent among patients with CNCP. 1,6 -11 Among patients with CNCP, the historical prevalence of depression has been reported to range from 5.9% to 46% in primary care clinics. 12 Both MDD and CNCP are closely related such that increasing severity of one commonly correlates with increasing severity of the other. 13 Patients with CNCP and concomitant MDD have a greater likelihood of using opioids at higher doses and for longer durations with an increased risk of abuse. 6 An estimated 35% of patients with chronic pain have an anxiety disorder. 14 Patients with anxiety disorder report greater interference from pain 15 and worse scores in health-related quality of life. 16 Management of patients with CNCP and concomitant mental health disorders can be challenging, especially if the underlying mental health condition is underrecognized. 13
Controlled substance agreements (CSAs) are a guideline-recommended, risk mitigation tool outlining the treatment parameters for COT and facilitating early identification of risks. 17,18 Presence of a mood or anxiety disorder should be assessed in patients prescribed COT. 19 Although lifetime prevalence of MDD or anxiety among patients on COT has been reported, 1,8 the prevalence and clinical correlates of concurrent depression or anxiety among patients on COT at the time of CSA enrollment are unknown.
We conducted a retrospective study of patients in a Midwest multispecialty primary care practice enrolled in CSAs for COT. Among patients self-reporting a history of depression or anxiety, we assessed presence of depression and anxiety, demographic characteristics, opioid dosing, and efficacy of pain management.
Methods
Study Setting
Mayo Clinic Midwest (MCM) is a medical center in Southeastern Minnesota. Employee and Community Health is a multisite, primary care practice of MCM located in Olmsted County, Minnesota. Employee and Community Health provides care to approximately 152 000 patients by clinicians in pediatrics, family medicine, and internal medicine. The institutional review board of Mayo Clinic reviewed and approved this research. Informed consent was not required.
Study Population
Patients with CNCP on COT were eligible for study inclusion if they previously provided authorization to access their medical record and completed depression and/or anxiety screening at CSA enrollment between May 9, 2013, and August 15, 2016. Patients self-reporting any symptoms or clinical diagnosis of depression and/or anxiety completed the Patient Health Questionnaire–9-item scale (PHQ-9) to screen for depression 20 and the Generalized Anxiety Disorder–7-item scale (GAD-7) to screen for anxiety disorders, respectively. 21 Patients were considered depression “screen-positive” if their PHQ-9 score was ≥10. Patients were considered anxiety “screen-positive” if their their GAD-7 score was ≥10. Patients who did not pick up their first prescription following CSA enrollment were excluded.
Controlled Substance Agreement Enrollment
Controlled substance agreement enrollment is recommended by institutional guidelines if patients are expected to be on a Drug Enforcement Agency (DEA) schedule II, III, or IV medication for ≥3 months. Patients enrolled in hospice, nursing homes, palliative care, or group homes are exempt. Provider discretion is allowed for patients receiving <10 pills per month. Upon CSA enrollment, nursing staff review CSA treatment parameters. The CSA specifies receipt of prescriptions from a single provider, restrictions on dose changes without approval, urine drug screening, and prescription renewal process. The Minnesota Prescription Drug Monitoring Program is queried to review prescribed DEA schedule medications.
Data Collection
Controlled substance agreement
Data collected at CSA enrollment were entered into a separate, secure clinical database and included patient demographics, primary indication for COT, and PHQ-9 and GAD-7 results.
Administrative data
Data were obtained from patient-provided information and billing data obtained annually and include race, educational status, employment status, relationship status, alcohol use, and tobacco use. Age-weighted Charlson Comorbidity Index 22 -24 (CCI) scores served as a measure of comorbidity burden. The CCI was calculated using an institutional protocol and administrative billing data 1 year prior to the date of CSA enrollment.
Electronic Health Record (EHR) data
Opioid prescription data were converted into morphine milligram equivalents per day (MME/day). Total opioid dose per day was calculated by multiplying the maximum prescribed doses per day by the amount of opioid per dose. Estimated MME/day was calculated by multiplying total opioid dose per day by a morphine equivalent conversion factor. 4,25
Statistical Analyses
Distribution of patient demographic characteristics, opioid therapy indication, comorbidities, opioids, and pain scores was compared between patients with depression and anxiety. Frequencies and proportions were calculated for categorical variables, and associations were assessed with χ2 test for independence. If χ2 test assumptions were violated (cell sizes <5), the Fisher exact test was used. Mean and standard deviation, median and interquartile range, and mode were calculated for continuous variables. Each continuous variable was assessed for normality using histogram plots, measures of skewedness and kurtosis, and the Shapiro-Wilk test for normality. Associations were assessed by comparing variable means using the 2-sample t test when the continuous variable was normally distributed. Pooled t statistics are provided where the folded F equality of variance estimates were equal (P > .05) and Satterthwaite t statistics where variances were unequal (P ≤ .05). Wilcoxon 2-sample tests were employed for non-normally distributed variables. All data management and statistical analyses were performed using Statistical Analysis Software version 9.3 (Cary, North Carolina), and significance was assumed when P ≤ .05.
We evaluated the association between positive screening for anxiety and for depression independently by deploying unadjusted and adjusted logistic regression models against the outcome of receiving an opioid dose of ≥50 MME/day. We included factors in the adjusted model which proved to be significant when independently modeled against the outcome. We reported odds ratios (ORs) and associated 95% confidence intervals (CIs).
Results
We identified 1066 eligible patients. Among these, 785 (73.6%) patients completed a PHQ-9 and 578 (54.2%) completed a GAD-7 upon enrollment (Table 1). Compared to screen-negative patients, patients who screened positive for depression or anxiety were younger, unmarried, not employed, and more likely to live alone.
Demographic Characteristics of Patients Completing a PHQ-9 or GAD-7 at CSA Enrollment.

Abbreviations: CSA, controlled substance agreement; GAD-7, Generalized Anxiety Disorder–7-item scale; IQR, interquartile range; PHQ-9, Patient Health Questionnaire–9-item scale; SD, standard deviation.
Patients screening positive for depression were more likely to report a need to cut down on alcohol consumption (Table 2). Patients screening positive for depression and anxiety were more likely to report that relatives or friends expressed worry or complain about their alcohol intake and more likely to report cigarette smoking.
Indication for Chronic Opioid Therapy, Charlson Comorbidity Index, and Substance Use Assessment.

Abbreviations: IQR, interquartile range; SD, standard deviation.
Patients screening positive for anxiety received higher mean MME/day (Table 3). Although patients screening positive for depression were more likely to report difficulty with pain, the scores for current pain, average pain over the past week, and worst pain over the past week were all higher for patients with positive depression or anxiety screens.
Prescribed Opioids and Pain Assessment.
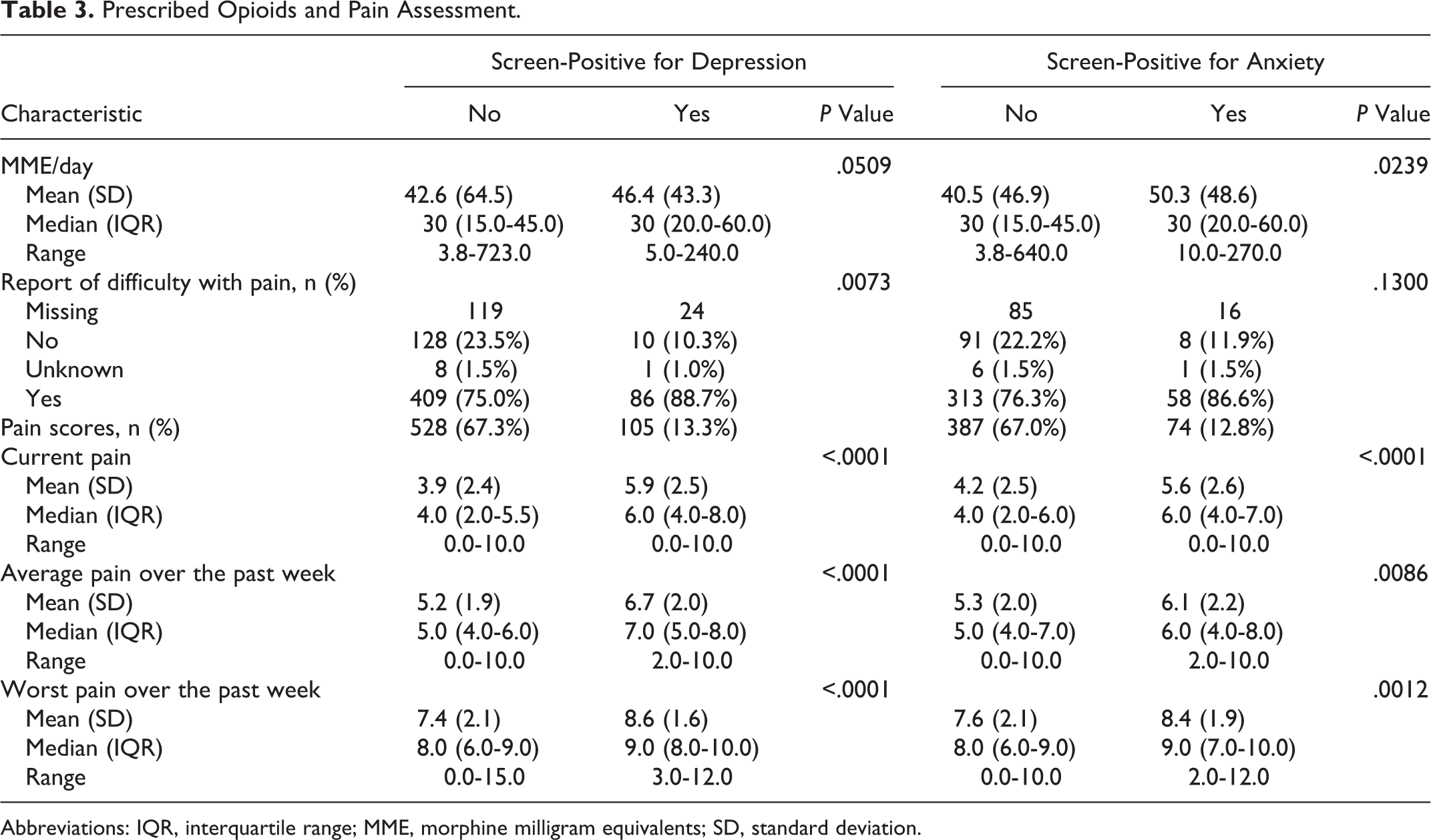
Abbreviations: IQR, interquartile range; MME, morphine milligram equivalents; SD, standard deviation.
In the uncontrolled models, patients who were screen-positive for anxiety and depression had increased odds of having an opioid prescription ≥50 MME/day (OR: 1.85; 95% CI: 1.13-3.05; OR: 1.80; 95% CI: 1.18 to 2.71, respectively). Within the anxiety model when controlling for marital status, smoking status, and age, this observed effect disappeared. However, patients who were screen-positive for depression had higher odds of receiving opioids ≥50 MME/day after controlling for marital status, smoking status, and age (adjusted OR: 1.62; 95% CI: 1.01-2.58).
Discussion
Among patients completing a PHQ-9 or GAD-7 at CSA enrollment, we observed rates of 15.4% and 14.4% for screen-positive depression and anxiety, respectively. This is consistent with previous literature which has observed rates of major depression ranging from 5.9% to 46% among patients with chronic pain in primary care. 12 Previous studies have suggested that an estimated 35% of patients with chronic pain have an anxiety disorder, 14 but this estimate was based upon a past year diagnosis. In contrast, we assessed the point prevalence of anxiety at CSA enrollment.
We observed that patients screening positive for depression or anxiety at CSA enrollment were less likely to be married. Our data are consistent with previous research regarding the interrelation of chronic pain, mental health conditions, and marital status. 26 -29 Although we did not collect information on the quality of marital relationships in our cohort, such data may be helpful to assess the potential relationships between the quality of the relationships and the use of opioids for the management of chronic pain.
Tobacco or alcohol abuse is frequently comorbid among patients with depression and anxiety. 30 -32 The relationship between depression and smoking in patients with chronic pain receiving opioids is complex. 33 We observed that patients who were screen-positive for depression or anxiety were more likely to smoke. Alcohol is the most common concomitant drug involved in opioid overdose, 34 and alcohol use among patients on COT can increase the risk of opioid misuse. 18,35 Our findings suggest a possible risk of concurrent alcohol misuse among patients screening positive for depression or anxiety.
Patients who screened positive for anxiety received greater mean MME/day than screen-negative patients. However, both cohorts consistently reported higher mean pain scores compared to screen-negative patients. This is consistent with published literature reporting that patients with current or past mental health disorders are more likely to receive opioids at higher doses and for longer durations. 7,10 Emerging evidence also suggests that COT may be a risk factor for precipitating incident or recurrent depression in CNCP patients. 6,10 The effect of anxiety, through catastrophizing a maladaptive cognitive style exaggerating threat of pain, increases the risk of opioid misuse independent of depression and may be a coping strategy among CNCP patients. 9 Given mortality risks associated with opioid use ≥50 MME/day and our observation that patients with depression are more likely to receive doses in this range, our findings support mental health screening in patients on COT to identify individuals at heightened risk for opioid adverse events.
Strengths of this study include analysis of a large cohort of patients with a history of depression or anxiety on CSAs for COT in a large, primary care practice. Our study also provides insight on the prevalence of patients screen-positive for anxiety and depression at the time of CSA enrollment. Patients in our sample were screened for depression or anxiety with validated clinical instruments.
Limitations of this study include generalizability to other communities, given the low percentage of minority patients. Inferences regarding the prevalence of positive screens for depression or anxiety in this population are limited as data were obtained only from patients who completed a PHQ-9 or GAD-7 at CSA enrollment. Additionally, no data were collected regarding antidepressant use or other treatments for depression or anxiety, which can affect opioid use, dosing, and perceptions of pain. 13 We observed a positive GAD-7 to be 14.4% in our population, which we agree is lower than what has been reported. 14 However, our ascertainment of anxiety was a point prevalence estimate upon CSA enrollment, while previous studies have reported higher rates based upon on a 12-month history of anxiety.
Primary care providers manage chronic pain and are most often the prescribers of COT. 36 -38 Controlled substance agreements are intended to mitigate risk associated with COT and are increasingly recommended as part of a comprehensive management strategy in CNCP patients. 17,18 Our findings suggest that in patients with a history of depression or anxiety, screening positive for depression or anxiety at CSA enrollment is associated with sociodemographic characteristics and behavioral factors that may further increase risk. Further research is needed to determine whether recognition of depression, anxiety, or other factors associated with COT risks at the time of CSA enrollment leads to improved management and outcomes for this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L.M.P. has received funding from GSK outside the current work. This work was supported by the resources of the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery.