
Abstract
Introduction
Over 80% of trauma related deaths in children occur in low income and middle-income countries including Ethiopia. Trauma affects several aspects of child life and is still a major concern. Despite the Ethiopian federal ministry of health (FMoH) conducting away different trials, there was an increased burden and high projection of pediatric trauma. In Ethiopia, There is insufficient evidence about the mechanisms, patterns and outcomes of pediatric trauma including this study area, Therefore this study aimed to assess the mechanisms, patterns, and outcomes of pediatric trauma in Agaro General Hospital, Southwest Ethiopia, 2021.
Methods and Materials
This cross-sectional study was study conducted on randomly selected 405pediatric patients who visited the Agaro General Hospital between 1/1/2018 and 30/8/2021. Data were extracted from each medical chart using a structured checklist. Data were entered into Epi-data 4.4.2.1for cleaning and analyzed using SPSS version 24. Tables, charts, and text are used to report the results.
Results
A total of 405 patients were included in the study. This study revealed that majority 271 (66.9%) of injured children were males. Most 188 (46.4%) of the traumas were occurred on the street. Fall down injury were the most common 151(37.3%) cause of trauma, followed by road traffic accidents 98 (24.2%). Trauma caused by falls accounted for 43.7% and 34.4% % of all traumas in the 5–12 year and the <5 year age groups respectively. Most 126 (31.1%) of the subjects were exposed to head and face trauma. Majority 256 (63.2%) of children were discharged with improvement, while12 (3.0%) of them have died.
Conclusions
Pediatric trauma remains a major public health concern. Most of trauma occurred among boys and falldown injury was the most frequent trauma, and the majority of the subjects were exposed to head and face trauma. Therefore, children should receive safety precautions, more supervision, and identification of specific risk factors for these injuries, and should be prohibited from risky practices by concerned bodies including families and traffic officers.
Introduction
Trauma is defined as any physical damage to the body resulting from abrupt exposure to forces exceeding the tolerance level, or a lack of warmth or oxygen. 1 Although trauma is a major public health problem worldwide in both developed and developing countries across all age groups, 2 children in developing countries are especially vulnerable to injury because of challenging living conditions, lack of safe play areas and absence of childcare options. 3 Children are predisposed to trauma owing their inability to understand the cause and effect of the different mechanisms of injuries and develop many severe complications. 4
The pattern of injuries varies according to different age groups in different countries with various causes such as, road traffic accidents(RTA), 5 burns, 6 falling down.4,7,8 The lower age groups (0–4 years) had a higher risk of mortality than the older age groups. 9 Worldwide approximately one million children under the age of 18 years are estimated to die annually due to trauma; with more than 2000 children per day. 10 Over 80% of the injury, deaths in children occur in low and middle-income countries (LMIC).11,12 Childhood Injuries contribute to 5.4% (265,000–348,000) of childhood deaths per year worldwide. 12
Severe trauma outcomes create a high emotional and economic burden on the family, society, and the world as a whole related to high admission prevalence in hospital and serious medical and surgical intervention required.9,13 The economic crisis that occurs due to trauma is continues after discharge from the hospital due to the long term effects of complications throughout life.14,15 The mortality of children with trauma varies depending on the number of body organs affected and the complications of the injuries. 9
In Ethiopia, in 2015, injuries resulted in 25,000 deaths among children aged 0–14 years. This figure is more than two times higher than that of the global burden of disease projects. 16 Projection of pediatric trauma in Ethiopia in 2015also showed a higher incidence of mortality until 2030 with the annual mortality caused by injuries projected to increase from 26,463, 27,807, and 30,364 in 2015, 2020, and 2030 respectively. 17
The foremost causes of trauma related problems in LMICs are related to somany issues including:absence of a good pre-hospital and a formal triage system, 18 inadequate staffing levels coupled with huge patient loads in emergency department management, and lack of basic surgical services. 19 To solve these problems, the world health organization, recommends the establishment of first-responder training programs in LMICs 20 and Emergency Triage, Assessment, and Treatment plus (ETAT + ) training. 21
The Ethiopian federal ministry of health (FMoH) has also been working to reduce the burden of pediatric trauma by implementing ETAT + strategies 22 and the Ethiopian health sector program provides great attention to injuries and violence prevention. 23 Despite the above mentioned programs and trials there are still numerous children with trauma problem in Ethiopia. Eventhough there are few studies on trauma of children in Addis Ababa and Hawwassa, Ethiopia5,24 mechanisms, patterns, and outcomes of trauma are varied among different age groups, place-to-place and time-to time due to different characteristics. Again, as far as our knowledge there is no sufficient information in this study area since time. Considering that definite pattern and mechanism of trauma is necessary for formulating policy and instituting preventive measures. Therefore, this study aimed to assess mechanism, patterns, and outcomes of pediatric trauma at Agaro general Hospital in Southwest Ethiopia, 2021.
Methods and Materials
Study Design, Area, and Period
This cross-sectinal was conducted in Agaro general hospital found in Jimma Zone of the Oromia Region south-western Ethiopia. Agaro general hospital is located in the Jimma Zone of the Oromia Region, at 397 km from Addis Ababa capital city of Ethiopia. It provides, dental, ophthalmic, medical, surgical, gynecology, obstetrics and pediatrics service. In the emergency department of Agaro general hospital 680, pediatric trauma was visited from 1/ 1/2018 to 30/8/2021. This study was conducted from 1/9/2021 to 23/10/2021.
Population, eligibility criteria
All injured children aged under 18 years who visited the emergency department of Agaro General Hospital were the source population. Medical chart of all injured children aged under 18 years old who visited in the emergency department at Agaro General Hospital from 1/ 1/2018 to 30/8/2021 E.C were study population. All pediatric trauma cases registered from 1/ 1/2018 to 30/8/2021 at Agaro General Hospital emergency department were included in this study. Pediatric trauma cases within complete registered variable information were excluded from the study.
Sample size determination
A single population proportion formula was used to calculate the sample size by considering the following statistical assumptions, Z = 95% (1.96), d = Margin of error = 5%, P = 39.8% (0.398), taking the prevalence of childhood road traffic trauma among children visiting the emergency department of AaBET Hospital, Addis Ababa, Ethiopia.
24

Sampling Techniques and Procedure
All traumatic children visited at Agaro General Hospital emergency departments between 1/ 1/2018 to 30/8/2021 were recruited as target population using the admission registration book. Then, sampling frame was prepared after a sequential number was assigned for each children with trauma. A sample among such children were selected from the sampling frame using a simple random sampling technique by using the computer random number generating system in Excel to select a required number of study participant's. Their medical record number was used to extract the medical charts of the selected participants from the card room. During the data collection, when randomly selected charts were missing major variables or card was lost, the charts were replaced with new, randomly selected, ones, from the remaining cards of the sampling frame, finally, a total planned 405 charts were included in the analysis.
Study Variables
The variables included were socio-demographic variables (age, sex, and place of residence), Pattern-related variables(Arrival time to the emergency department, pre-hospital care, intent, mechanism and nature of injury, place of occurrence, vehicles involved in RTA, anatomic sites of body injury), mechanism-related variables and pediatric trauma outcome-related variables (duration of hospital stay and pediatric trauma outcome status).
Operational Definitions
Data Collection Tool and Procedure
The checklist was adapted from previously conducted research in Addis Ababa 24 and modified from the related literature to address the objective of the study. Data collectors were trained in the data collection process for one day. Finally, data were extracted from each medical chart using a structured checklist by two BSc nurses and supervised by an MSc nurse. The checklist consisted of information emphasizing socio-demographic variables, Patterns and mechanism related variables and Pediatric trauma outcome-related variables. During the data collection process of each questionnaire was checked daily by the principal investigators for completeness and accuracy of the information collected.
Data Quality Control
In order to ensure quality of data, A pretest was conducted on 5% 21 of the total sample size of the study before actual data collection period at Jimma medical center. Based on the pretest result wording, language consistency and edition were made. Principal investigator and supervisor were checking daily the completeness of the filled tool.
Data Processing, Analysis, and Presentation
The row data after collection has been processed(edited, coded, classified and tabulated
Ethical Consideration
Permission Letter was obtained from the research committee of Mizan-Tepi University College of health science, department of nursing. A formal letter was submitted to Agaro general Hospital executive officer and concerned bodies to obtain their co-operation. Then, data were collected after consent of cooperation was obtained from hospital administrator focal person to use the secondary data for this study. Because of the anonymous and retrospective nature of the study, the need for informed consent was waived.
Results
In this study, from January/ 1/2018 to 30/8/2021, aproximatly 680 patients under 18 years of age visited at Agaro general hospitals. Of these, 405 pediatric trauma medical charts were reviewed based on the required samples making a response rate of 100%.
Socio-Demographic Characteristics
Among a total of 405 study participants, 271 (66.9%) of injured children were male. The majority 167 (41.2%) of children age group of five to twelve years were more affected by trauma and their mean age was found to be 9.26 ± 4.95. Likewise, the majority 315 (77.8%) of the trauma cases that happened was in children who came from urban areas (Table 1).
Socio- Demographic Characteristics of Injured Children Visited at Agarogeneral Hospital, from September 1/1/2018 to 30/8/2021 (N = 405).

Pattern and Mechanism of Traumatic Characteristics
Majority of child trauma causes were falldawn 151 (37.3%) followed by road traffic accidents 98 (24.2%) and animal bite 72 (17.8%). Most of the traumas were occurred on the street or road 188 (46.4%) followed by at home 149 (36.8%). Concerning to place of road traffic accidents, most of the traumas 57 (58.2%) were occurred among street walkers. Among the traumas caused by RTA, motor bicycle trauma accounted the highest portion 51 (52%) followed by car trauma 33 (33.7%). Regarding the location of trauma face and head trauma were the major 126 (31.1%) anatomical locationthat trauma was occurred followed by 124 (30.6%) abdomen and pelvic trauma. Most children were traumatized as single body trauma that accounting for 336 (83.0%) of the total trauma (Table 2).
Pattern and Mechanism Characteristics of Traumatic Children Visited at Agaro General Hospital Emergency Department from 1/1/2018 to 30/8/2021(N = 405).

Natural event: environmental degradation, volcanic eruption, flooding, climate change.
Patterns of Regional Injuries Divided into age Group and Outcome status
Abdominal and pelvic trauma were frequent in the 5–12 year age group children, accounting for 38.7% of trauma. Similarly head and face injuries were common among 5–12 year age group victims, accounting for 42.7% of trauma. Abdominal and pelvic traumas were leading causes of all mortalities in the hospital 12 (9.7%). Children with chest and thoracic injuries were have a higher proportion 50% of admission rate in the hospital (Table 3).
Characteristics of Pediatric Patients with Regional Injuries Divided into age Group (Years)and Outcome status Visited at the Emergency Department of Agaro General Hospital Between 1/ 1/2018 to 30/8/2021 (N = 405).

Patterns of Cause of Injury Divided into age Group
Trauma caused by falls was the most frequent in the 5–12 years old and the <5 years old age groups, accounting for 43.7% and 34.4% % of all traumas respectively. Road traffic accidents were the most common cause of trauma among 13–18 years age groups children accounting for 40.8%. An animal bite was the third most common commonly trauma accounting for 50.0% and 33.3% of traumas in the age group of 13–18 and 5–12 years old respectively (Table 4).
Characteristics of Pediatric Patients with the Cause of Injury Divided into age Groups (Years) Visited at the Emergency Department of Agaro General Hospital Between 1/1/2018 to 30/8/2021 (N = 405).

Outcome status-Related Characteristics
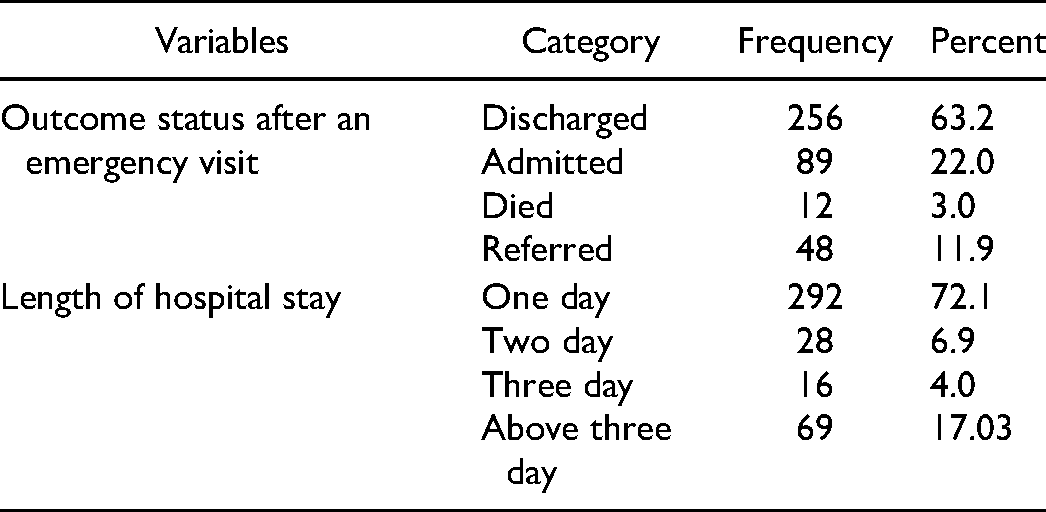
After triage in the emergency department, a majority 256 (63.2%) of children were discharged with improvement and 12 (3.0%) of the traumatic children were died. Regarding hospital stay, 292 (72.1%) of the children were stayed in the hospital for one day (Table 5).
Out come status-Related Characteristics of Children with Trauma Visited at Agaro General Hospital among Emergency Department from 1/1/2018 to 30/8/2021(N = 405).
Outcomes of Pediatric Trauma Patients Based on age Groups (Years)
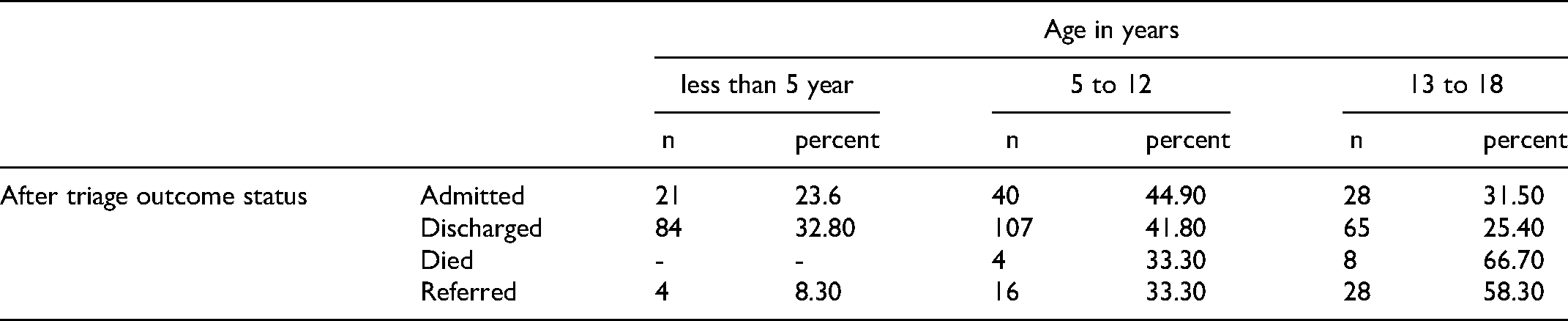
In-hospital mortality was 66.7% and 33.3% in the 13–18 year and the 5–12 years age groups respectively. From overall admission in the hospital. Majorty 40 (44.90%) of admitted children were in the age group 5–12 years old (Table 6).
Characteristics of Traumatic Pediatric Patients with Outcome Statusdivided into age Groups at Emergency Department of Agaro General Hospital Visited Between 1/1/2018 to 30/8/2021 (N = 405).
Discussion
Pediatric trauma is the most common and life- threatening injury in children and is public health problem. Mechanism, pattern and outcome of trauma vary from place-to-place with different characteristics. Therefore, this study aimed to assess the patterns, the mechanisms and outcomes of pediatric trauma at Agaro general Hospital in Southwest Ethiopia, 2021.
In this study, a large proportion (66.9%) of male children were the most affected by trauma. A study conducted in united kingdom 8 and Kenya 7 was almost similar to this finding, where the proportion of male with trauma was 64.3% and 65.3% respectively. The possible reason for this may be differences in play time behavior between genders, as well as higher activity levels, greater freedom to play alone, and increased involvement in risky sports among males. The other possible reason can be males usually display more conflict and fighting with their colleaques which may increase trauma in males and the socialization process leads males, from the time they are little boys, to engage in more behavioral risks and Lifestyle as well as masculine socialization than females, and to be supervised less by someone who might protect them from risk. 25
Regarding body regions affected in this study, most 126 (31.1%) of the subjects were exposed to head and face trauma, studies from united kingdom, 8 Denmark 26 and Australia 9 had documented similar findings. This may be due to the fact that most lower age children had alarger head as compared with other body parts and also had weaker neck ligaments and spine musculature, which leads to more head and face trauma.
Moreover, this study revealed that falldown injury was the most common cause of injury 151 (37.3%), which was supported by other studies conducted in Kenya (46%) 7 and the united kingdom. 8 A possible reason for this could be a lack of safety measures for unsupervised children, such as a lack of protection pads for children riding bikes, window guards, and building regulations, which lead to falling trauma. Another possible reason may be that most of our study participants were in the age group 5–12, so this age is the time they need any trial beyond their level including riding a bicycle.
Furthermore, this study's findings showed that the second most common cause of injury was RTA 98 (24.2%), which is lower than other studies conducted in Addis Ababa AaBET Hospital, where RTAs accounted (40%). 24 This difference might be due to the higher traffic burden in Addis Ababa, which is the capital city of Ethiopia. In this study, most injuries occurred on streets/roads 188 (46.4%). Thisis in line with a study conducted in Addis Ababa, 24 around (42.4%) of children's injuries were occurring on the streets. This could be a reflection of children often being allowed to play on local streets as in our study more 41.2% number of children were in the age group of 5 to 12 years. The other possible reason for this may be that age group needs trial of different risky activities such as playing various types of physical activity related games and trying different creative ideas.
In this study regarding to the trauma caused by RTA, motor bicycle trauma accounts the highest portion 51 (52%), which is supported by studies conducted in Japan 4 and united kingdom, 8 where almost a third of the children were exposed to motor vehicle collisions. The possible justification may be that since most care givers/parents use motor bicycle and seat their child in their back without seatbelt to send and return back from school due to economical inadquecy to use safe cars for their child.
In this study 5–12 year age group children were frequently traumatized with A and pelvic trauma, accounting of 38.7% of trauma. A possible reason may be that this study showed road traffic accident was common and thus studies show that abdominal and pelvis injury mostly associated with RTAs, 27 and which might be supported by an evidence that approximately 15% of the overall trauma injuries affect the abdominal area. 28
Moreover, in this study children who had abdominal and pelvic traumas were leading of all mortalities in the hospital 12 (9.7%). This might be because the abdomen holds various sensitive organs such as the kidney, spleen and liver internally thus, sensitive organ injuries usually lead to mortality in children.
This study also found in-hospital mortality of children related to trauma after the emergency visit was 12 (3.0%). Our finding was higher than that study conducted in Addis Ababa AaBET Hospital (0.2%). 24 A possible reason for this significant discrepancy could be the difference in service provision, since AaBET Hospital is a referral hospital. However, our study mortality was lower than the study conducted in Japan at 3.9% 4 and Australia 11.1%. 9 A possible reason for this difference might be the age limit of the study participants.
Strength and Limitation of the Study
This study has certain limitations. First of all, owing to the retrospective nature of the study, the data were collected from secondary sources and some important characteristics that could found in the patient medical chart may be missed. The second limitation is, patients with lost cards and incomplete records were excluded which may cause underestimation of the results. In spite of these limitations, the results of this study make certain contributions to current literature in certain aspects and better understanding on pediatric trauma cases to facilitate better management of this vulnerable population. This study was investigated for the frst time about pediatric trauma patients in southwet part of Ethiopia.
Implication of the Study
Currently, some trials attempted with the aim of preventing pediatric trauma and its severe outcomes in Ethiopia.22,23 However, the current study's findings indicated that the pediatric trauma related burden and mortality is high. This highlights the fact that children with trauma are at a higher risk of developing different complications and disabilities. Thus, Ethiopian government needs to strengthen existing trials and strategies to decrease the proportion of different traumas in children by preventing common mechanisms of trauma. In addition to governmental organizations, Other non-governmental organizations should focus on truama reduction intervention programs to control the prevalence of different traumas in children and other disabilities. Additional attention should be given to children with different common modes of traumas including fall down, RTA and animal bite. Children with face, head, abdomen and pelvic trauma should also strictly followed and managed early to prevent longterm disbality. Health education should be given for those parents who had children with trauma and also for mothers who had children aged from five to twelve for primary prevention of trauma. Different concerned bodies at different health institutions including clinicians should be encouraged to minimize the risk of different trauma.
Conclussions and Recommendation
Pediatric trauma remains a major public health concern. This study indicates the majority of trauma cases were boys than girls. Falls, road traffic accidents, and animal bites are the leading causes of pediatric trauma. Falls predominates in younger children, while RTAs predominate in older children. Abdominal trauma was associated with hospital admission. Therefore, proven preventive measures such as sit belt and bike helmets should be recommended by health professionals.
Footnotes
Acknowledgements
Mizan-Tepi University College of health science, department of nursing is acknowledged for providing this opportunity to conduct this study. Our thanks also go to Agaro General Hospital pediatric staff and the card extractors. It is also our pleasure to thank the data collectors and supervisors.
Authors’ Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Permission Letter was obtained from the research committee of Mizan-Tepi University College of health science, department of nursing. A formal letter was submitted to Agaro general Hospital executive officer and concerned bodies to obtain their co-operation. Because of the anonymous and retrospective nature of the study, the need for informed consent was waived and therefore no written consent from the child or parent was required. To keep the confidentiality names and medical record numbers of the participant were not registered in the data collection tool. Generally, the study was performed per the Declaration of Helsinki.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to Participate
All regulatory requirements were met and because of the anonymous and retrospective nature of the study, no written consent from the patient or parent was required.
Availability of Data and Materials
The raw data file could be provided for research purposes only, upon request via e-mail of the corresponding author