
Abstract
Aim:
The present research aimed to determine the relation between metabolic syndrome (MetS) and thyroid volume and nodule prevalence among Turkish population patients.
Methods:
This retrospective cohort study was carried on 850 patients between the ages of 20 and 65 who visited the diabetic, endocrinology, and general surgery outpatient clinics in the Mega Medipol and Medipol Hospital between January 2014 and December 2017. This study included sociodemographic information, body mass index (BMI), diabetes mellitus (DM), systolic (SBP) and diastolic (DBP) blood pressures, and clinical biochemistry results such as serum triglyceride, total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein (LDL) cholesterol, hemoglobin A1c (HbA1c), fasting blood glucose levels, thyroid-stimulating hormone (TSH), T3, T4, and other MetS parameters. Thyroid fine needle aspiration biopsy was suggested to patients whose thyroid nodules were greater than 1.00 cm. The definition and diagnostic of MetS used as proposed by the National Cholesterol Education Program—Third Adult Treatment Panel.
Results:
There were statistically significant differences between patients with thyroid nodules and those without regarding age, gender, BMI, physical activity, cigarette smoking, shisha smoking, family history of diabetes, hypertension, and thyroid. Meanwhile, statistically significant differences were found between with and without MetS for calcium (P = .028), magnesium (P < .001), potassium (P < .001), fasting blood glucose (P = .047), HbA1c (P < .001), HDL (P < .001), LDL (P < .001), albumin (P = .008), bilirubin (P = .002), triglyceride (P = .011), SBP (P = .001) and DBP (P = .011), TSH (P = .005), T3 (P < .001), and T4 (P < .001). Furthermore, there were statistically significant differences between participants with and without thyroid nodules for calcium (P < .001), magnesium (P < .001), potassium (P < .001), fasting blood glucose (P = .010), HbA1c (P = .019), HDL (P < .001), LDL (P = .012), albumin (P = .002), bilirubin (P < .001), triglyceride (P < .001), SBP (P < .001) and DBP (P = .004), TSH (P = .015), T3 (P < .001), and T4 (P < .001). Multivariate stepwise logistic regression analysis used for independent predictors for the presence of thyroid nodules which TSH (P < .001), family history of thyroid and DM (P < .001), age in years (P = .025), DBP and SBP (P < .001), BMI (P = .014), HDL-C (P = .034), and waist circumference (in cm; P = .044) were considered at higher risk as a predictors of thyroid with patients with MetS.
Conclusion:
The results of the current study confirm a strong positive association between MetS and thyroid nodules risk among patients with MetS. This study suggest that the patients with MetS can be considered as a marker to have moderately increased risk of future thyroid nodules and cancer. Meanwhile, MetS, obesity, and hyperglycemia could be a qualifiable and modifiable risk factor for thyroid nodules. The regularly glycemic control may be the most important treatment for the reduction of incidence or the prevention of thyroid.
Introduction
Metabolic syndrome (MetS) and type 2 diabetes mellitus (T2DM) are the main threats to the 21st century and impress the health and economic status of most countries. 1 Metabolic syndrome leads to an increase in the risk of cardiovascular disease 2–3 and thyroid 4 –6 in long term. They are the primary reason of mortality and morbidity in most high-income and developing countries. 3 Lifestyle factors, sleep duration, physical activity, regular exercise, and healthy-balanced diet are essential components in the prevention of MetS. 3
Overall, in the last 3 decades, the incidence and prevalence of thyroid cancer, in other words papillary histotype, has indicated a stable rise around the world. 5 –8 Metabolic syndrome is a clustering of medical conditions that reflects overweight, obesity, sedentary lifestyles, stress, hypertension, hyperglycemia, and dyslipidemia, 3,8,9 which they are not independent of one another and that they may share underlying causes and mechanisms. 8 In several studies, MetS is considered as a risk factor for cardiovascular disease and thyroid. 10 –13 Positive associations between MetS and thyroid nodules have been reported by several authors. 10,13 The present research aimed to determine the relation between MetS and thyroid volume and nodule prevalence among Turkish population patients.
Participants and Methods
This retrospective study was performed on participants between the ages of 20 and 60 who visited the diabetes, endocrinology, thyroid surgery, and outpatient clinics in the Mega Medipol International School of Medicine Hospital and Medipol Hospital from January 2014 to December 2017. The current sample size was based on the detected as 850 case series registered with diagnosed MetS and thyroid nodule to be included to meet specific objectives. The Institutional Review Board (IRB) ethical approval for the present study was taken from the Medipol International School of Medicine, Istanbul Medipol University, and patients gave informed written consent before starting.
Laboratory Measurements
Patients were considered to have DM if they have a history of DM and were currently taking any oral medications for diabetes. According to the World Health Organization (WHO) and International Diabetes Federation (IDF), DM is defined when fasting venous blood glucose concentration is equal or higher than 7.0 mmol/L and/or postprandial blood glucose concentration is higher than 11.1 mmol/L. 1,9 A glucometer was used to measure fasting blood glucose of all patients. Oral glucose tolerance test was carried out only if blood sugar was less than 7 mmol/L. The inclusion criteria comprised of diagnosis of T2DM in conformity with international standards by WHO and IDF. 1,9
The definition and diagnostic of MetS used as proposed by the National Cholesterol Education Program–Third Adult Treatment Panel guidelines 1,9,14 : (1) a participant has the MetS of waist circumference higher than 94 cm in men and 80 cm in women; (2) level of fasting glucose level has to be higher than 100 mg/dL (5.6 mmol/L) or a participant must have been previously diagnosed with impaired fasting glucose; (3) level of blood pressure has to be higher than 130/85 mm Hg or a participant was cured for hypertension; (4) level of triglyceride must have been measured to be higher than 150 mg/dL (1.7 mmol/L); (5) level of high-density lipoprotein cholesterol (HDL-C) must be less than 40 mg/dL (1.03 mmol/L) in men and 50 mg/dL (1.29 mmol/L) in women or participant was cured for low HDL.
Thyroid Evaluation
A thyroid nodule is a lump that occurs from the abnormal growth of thyroid cells, located at the base of the neck, and produces the hormones thyroxine and triiodothyronine. 15 A 10-MHz linear probe (Logiq 5 Pro, GE Medical Systems, Wisconsin) was used by same physician (C.C.B.) for thyroid ultrasonography. Thyroid fine needle aspiration biopsy was suggested to patients whose thyroid nodules were higher than 1.00 cm.
Questionnaire, Physical Examination, and Measurements
This study included several parameters such as sociodemographic characteristics, lifestyle habits, and biochemical test results. Patients were classified as physically active if they walked or cycled for more than 30 minutes per day.
The data were analyzed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, version 22.0; IBM Corp, Armonk, New York). The significance of differences between mean values of 2 continuous variables was determined by Student t test for normal distribution data and by Mann-Whitney U test for not normal distribution data. Chi-square test tested the differences in proportions of categorical variables between 2 or more groups. Multivariate logistic regression analysis using the forward inclusion and backward deletion method was used to assess the relationship between dependent and independent variables and to adjust for potential confounders and orders the importance of risk factors (determinants) to predict the factors for the presence of thyroid nodules. The cutoff value for determining significance was chosen as 0.05.
Results
Table 1 presents the comparison of sociodemographic and clinical characteristics of the metabolic variables and presence of thyroid nodules in participants. There were statistically significant differences between patients with and without thyroid nodules regarding age, gender, body mass index (BMI), physical activity, cigarette smoking, shisha smoking, family history of diabetes, hypertension, and thyroid.
Comparison of Sociodemographic and Clinical Characteristics of the Metabolic Variables and Presence of Thyroid Nodules in Participants.a

Abbreviations: BMI, body mass index; CI, confidence interval; DM, diabetes mellitus.
a N = 850.
Table 2 shows the clinical biochemistry baseline value among MetS participants and presence of thyroid nodules in participants with and without metabolic syndrome. Statistically significant differences were found between with and without MetS for calcium (P = .028), magnesium (P < .001), potassium (P < .001), fasting blood glucose (P = .047), hemoglobin A1c (HbA1c; P < .001), HDL (P < .001), low-density lipoprotein (LDL) (P < .001), albumin (P = .008), bilirubin (P = .002), triglyceride (P = .011), systolic blood pressure (SBP; P = .001) and diastolic blood pressure (DBP; P = .011), thyroid-stimulating hormone (TSH; P = .005), T3 (P < .001), and T4 (P < .001).
Clinical Biochemistry Baseline Value Among Metabolic Variables Participants and Presence of Thyroid Nodules in Participants.a,b
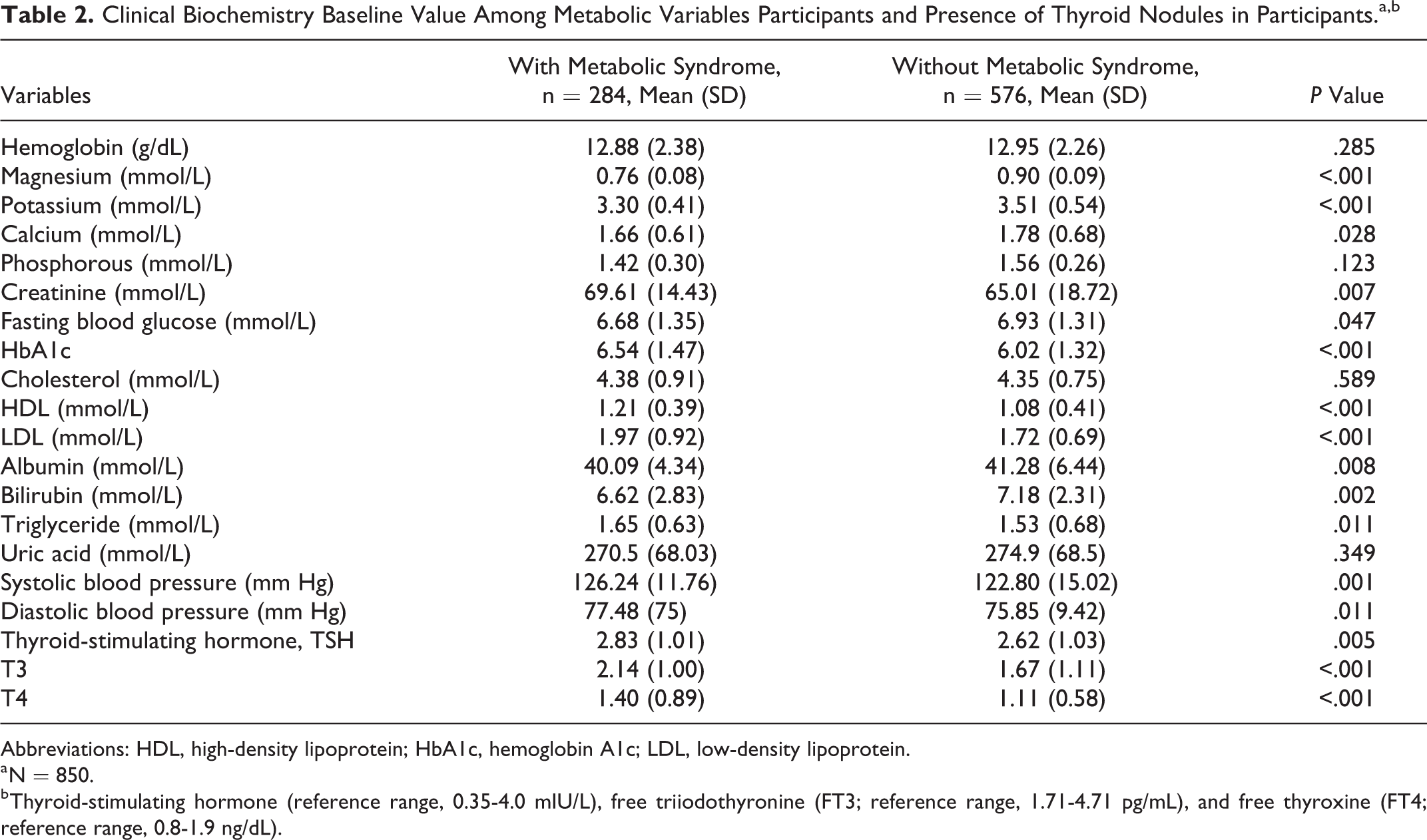
Abbreviations: HDL, high-density lipoprotein; HbA1c, hemoglobin A1c; LDL, low-density lipoprotein.
a N = 850.
b Thyroid-stimulating hormone (reference range, 0.35-4.0 mIU/L), free triiodothyronine (FT3; reference range, 1.71-4.71 pg/mL), and free thyroxine (FT4; reference range, 0.8-1.9 ng/dL).
Table 3 presents the clinical biochemistry baseline value among MetS participants with thyroid and without thyroid nodules. There were statistically significant differences between participants with and without thyroid nodules for calcium (P < .001), magnesium (P < .001), potassium (P < .001), fasting blood glucose (P = .010), HbA1c (P = .019), HDL (P < .001), LDL (P = .012), albumin (P = .002), bilirubin (P < .001), triglyceride (P < .001), SBP (P < .001) and DBP (P = .004), TSH (P = .015), T3 (P < .001), and T4 (P < .001).
Clinical Biochemistry Baseline Value Among Metabolic Syndrome Participants With Thyroid and Without Thyroid Nodules.a

Abbreviations: HDL, high-density lipoprotein; HbA1c, hemoglobin A1c; LDL, low-density lipoprotein.
a N = 850.
Table 4 indicates multivariate stepwise logistic regression analysis of independent predictors for the presence of thyroid nodules. Thyroid-stimulating hormone (mIU/L; P < .001), family history of thyroid and DM (P < .001), age (in years; P = .025), DBP (mm Hg; P < .001), SBP (mm Hg; P < .001), BMI (P = .014), HDL-C (P = .034), and waist circumference (cm; P = .044) were considered at higher risk as predictors of thyroid for patients with MetS.
Multivariate Stepwise Logistic Regression Analysis of Independent Predictors for the Presence of Thyroid Nodules.
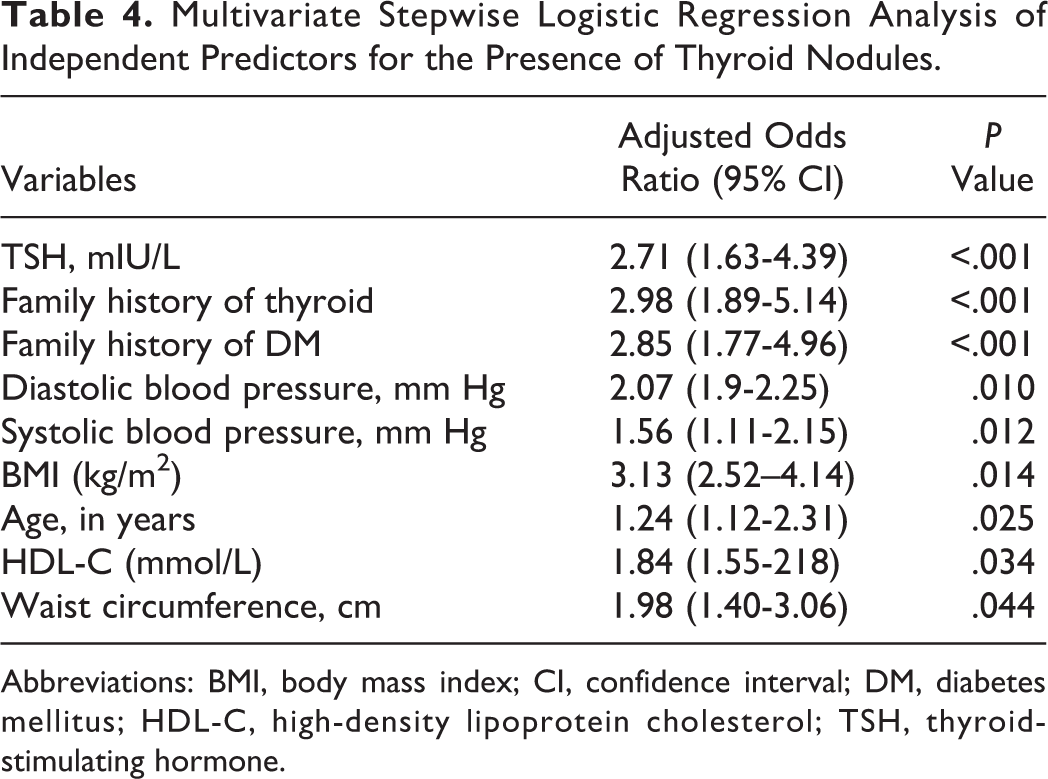
Abbreviations: BMI, body mass index; CI, confidence interval; DM, diabetes mellitus; HDL-C, high-density lipoprotein cholesterol; TSH, thyroid-stimulating hormone.
Discussion
This study determined the relationship between the presence of thyroid nodules and the components of MetS in healthy Turkish population with no evidence of iodine insufficiency. Although Turkey have moderately iodine-deficient area, 16 the present study demonstrates that people with MetS had a higher prevalence of thyroid nodules. The current results revealed strong correlation between thyroid nodules and MetS elements, which may have important implications for the diagnosis and treatment of thyroid-related diseases, those results are consistent with the Korean study 4 and pervious reported study in Turkey. 16 Furthermore, MetS is usually recognized as a complication and risk for thyroid. Therefore, effective control of MetS is essential to reduce the incidence of thyroid in the middle age-group and may affect the quality of life. The elements of MetS lead to increase thyroid volume and nodule. These are consistent with the results of Ayturk et al 12 and Korean study 4 that pointed out the insulin level as a predictor of thyroid volume increase. Further, the participants with MetS also had a higher prevalence of thyroid nodules larger than 1 cm, consistent with a previous study showing a positive association between insulin resistance and thyroid nodule size. 4,10
Furthermore, several studies reported that thyroid volume is related to a variety of risk factors such as iodine deficiency and supply, BMI, age, gender, smoking status, genetic factors, impaired fasting glucose, and DM. 4,12,17 –19 Additionally, a study has investigated the role of environmental and lifestyle factors. 6 In a few recent studies, thyroid cancer risk factors including iodine deficiency, environmental, genetic, family history of DM and hypertension, and lifestyle factors. 6,8,10,13,17,20 The current study is confirmative with the documented literature determining the association between metabolic disorders characterized by insulin resistance and the risk of thyroid cancer with the underlying results. 8,17,20 More recently, a few studies 4,8,21 which have assessed how thyroid functions related to MetS prevalence in large populations have revealed strong correlations between thyroid, and obesity, T2DM, and MetS. These results are confirmative with the current study.
Limitations and Strength of Study
Our study has several strengths but also some weaknesses. Firstly, the sample might be partially biased due to the retrospective cohort study. Secondly, we did not have data on the frequency of thyroid examinations in our study population. Thirdly, there was no cytological or histological results for each nodule. The greatest strengths of this study are the very large sample of participants and the large data set of risk factor variables such as TSH, T3, T4, body weight, physical activity, smoking cigarette, diet, BMI, family history of diabetes, hypertension, and thyroid.
Conclusion
The results of the current study confirm a strong positive association between MetS and thyroid nodules risk among patients with MetS. This study suggest that the patients with MetS can be considered as a marker to have moderately increased risk of future thyroid nodules and cancer. Meanwhile, MetS, obesity, and hyperglycemia could be a qualifiable and modifiable risk factor for thyroid nodules. The regularly glycemic control may be the most important treatment for the reduction in the incidence or prevention of thyroid. Therefore, it may lead to improve the quality of life in patients.
Footnotes
Authors’ Note
A.B., M.Ö., and Y.Ö. designed and supervised the study and were involved in data collection, statistical analysis, and the writing of the paper. C.C.B. was involved in data collection, interpretation of data, and writing the manuscript. All authors approved the final version.
Acknowledgments
The authors would like to thank the Istanbul Medipol University for their support and ethical approval (Research Protocol and IRB# 10840098-604.01.01-E.8421).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Istanbul Medipol University, International School of Medicine.