
Abstract
Background:
Women are left out of the conversation on contraceptive use due to a variety of reasons. One of the reasons women have reported for their nonuse of family planning method is that they do not decide to use or not to use it. This study aimed to assess the women’s decision-making on contraceptive use and identify its associated factors.
Methods:
Data for this study were extracted from the national representative 2016 Ethiopian Demographic and Health Survey. Data were collected using 2-stage cluster design, in which enumeration areas forming the first stage and households making the second stage. The analysis was done using multinomial logistic regression using STATA software version 14.
Results:
The study revealed that one-fourth (24.3%) 95% CI (23.7%-25.1%) decision was made by women. The multinomial analysis demonstrated women’s decision-making on contraceptive use was influenced by the age of women 15 to 19 years (adjusted odd ratio [AOR] = 0.327, 95% CI: 0.175-0.613), 20 to 24 years (AOR = 0.510, 95% CI: 0.390-0.666), and 25 to 29 (AOR = 0.557 95% CI: 0.460-0.675); place of residence (urban; AOR = 1.637, 95% CI: 1.331-2.015) and region in which the women dwell and husbands education; occupation of both woman and her husband; and number of children ever born were the factors significantly associated with the outcome variable.
Conclusions:
Women’s decision-making on contraceptive utilization was low. It was influenced by age, place of residence and region, education, occupation, and number of children ever born.
Background
Unintended pregnancy is a well-established public health concern with a high link among sexually active women. 1 Globally, an estimated 40% of women report unintended pregnancies. 2 Modern contraceptives remain and effective means to prevent unintended pregnancy. Although there is a wide range of contraceptive options available, statistics indicate low usage of the contraceptive method increases the problem of unintended pregnancy. The prevalence of contraceptive use is low in sub-Saharan Africa, including Ethiopia. 3
Women are left out of the conversation on contraceptive use due to a variety of reasons. 4 Even though many women want to avoid pregnancy, they are not utilizing any contraceptive method. 5 One of the reasons women have reported for their nonuse of family planning method is that they do not decide to use or not to use it. 4 The reason for not decide on the use of contraceptive use is due to cultural discrimination, lack of education, and other factors. 6 The other important issues associated with contraceptive use are a woman’s decision-making power within the household. 7 Evidence showed that women who have decision-making power are more likely to use than those who do not. 8 Women who have active involvement in domestic decision-making can control their fertility through accepting of modern contraception. 9
In Ethiopia, since recent times the government took many interventions to modernize many subcultures by allowing women to receive higher education, actively engage in the labor force, marry at greater than 18 years, choose their partners, and live apart from extended families. 10 This may help to reduce control of partner over couples and their decisions and also associated with greater female decision-making power in some settings. 11
In the health communication literature, the study has found that many women prefer shared decision-making, in which both the provider and the patient contribute to the choice of medical treatments. 8 There are variations in preferences, however, with some women preferring to make decisions autonomously and others to make decisions for them. 7 Furthermore, there appears to be individual variation in decision-making preferences depending on the specific health care decision. Studies have suggested that decision-making power improves service utilization outcomes. 4,7
There is a paucity of information concerning the role of women by themselves on a woman’s current contraceptive use or her future intentions of family planning uptake in the country. Therefore, this study aimed to study the magnitude of women’s decision on contraceptive utilization and its predictors among reproductive age women in Ethiopia based on the Ethiopian Demographic and Health Survey (EDHS) data. Hence, the current study will provide up-to-date evidence for policymakers and other stakeholders working on family planning in Ethiopia and similar setting to solve problems related to the women’s decision-making power based on evidence.
Methods
Study Design and Setting
Ethiopia is a country on the horn of Africa, the largest and most populous in the region. The capital city is Addis Ababa, located almost in the center of the country. According to the Central Statistical Agency 2007 census result, 12 the country has a total population of 106 million; with a sex ratio of 1.04:1. Administratively, Ethiopia is divided into 9 geographical regions and 2 cities administration. The 2016 EDHS was a population-based cross-sectional study conducted from January 18, 2016, to June 27, 2016, across the country. 13 Ethiopia has a 3-tier health care delivery system. The first level is a primary level comprising a district hospital, health centers, and their satellite health posts. The second level in the tier is a general hospital and the third is a specialized hospital, both exclusively focusing on curative health services.
Data Source
The study used data from the 2016 Ethiopian demographic health survey of women age 15 to 49 years. In this study, the data set was obtained from the Demographic Health Survey (DHS) database at http://dhsprogram.com/data/. The DHS program office gave an authorization letter to access the 2016 EDHS, which is the fourth comprehensive survey.
Population and Sampling Procedures
All women aged 15 to 49 years were the study population. First, each region was stratified into urban and rural, which yielded 21 sampling strata. The 2016 EDHS sample was selected in 2 stages. In the first stage, a total of 645 clusters (202 in urban and 443 in rural) were selected randomly and allocated proportionally to the household size from the sampling strata and in the second stage, 28 households per cluster were selected using systematic random sampling. Representative samples of 18 008 households were selected in 2016 EDHS. For an individual interview, 16 583 eligible women were identified from the interviewed household. Interviews were completed with 15 683 women, yielding a response rate of 95% CI. In this study, 9435 eligible women aged 15 to 49 delivered within 5 years preceding to 2016 survey under 643 clusters were included. 13
Study Variables
The dependent variable was women’s decision on contraceptive use, while independent variables were age (year), residence (rural or urban), region, wealth index ($) occupation, and education of husbands and women as well as number of children ever born. The dependent variable has 3 responses (mainly respondent, jointly, and husband/partner).
Data Analysis
Data analysis was carried out using STATA version 14; descriptive statistics were used to provide sample characteristics including sociodemographic characteristics, interaction with the health system, and median access. Bivariate analysis was used to assess the individual relationship of each explanatory variable with women’s decision on contraceptive use, while multivariate analysis was used to assess relationships while controlling for other explanatory variables. In multinomial logistic regression, jointly decision was considered as reference, and mainly respondent and husband/partner were 2 categories. The overall categorical variables with a P value of <.25 at the binomial analysis were included in the final model of the multinomial logistic regression model in which odds ratios with 95% CIs were estimated to identify the independent variables of women’s decision-making. P values less than .05 were used to declare statistical significance. All analysis was done on weighted data.
Results
Sociodemographic Characteristics of the Respondents
Of this, 2357 (25%) of the women were between the age of 40 and above years and 84 (0.9%) were in the age group of 15 to 19. Almost three-quarters (74.2%) of study participants were living in the rural part of Ethiopia, and 2061 (21.8%), 1754 (18.6%), and 1396 (14.8%) of the study participants were from Southern Nations, Nationalities, and Peoples’ Region, Amhara, and Oromia regions, respectively. More than half (55.9%) of the respondent’s husband occupations were an agricultural employee. About a quarter (25.8%) and 4222 (44.7%) of the study participants were agricultural employees and unemployed, respectively. About three-fifth (60%) of the study participants didn’t have formal education, while more than one-fourth (28.2%) of them were completed primary school (Table 1).
Characteristics of Women of 15 to 59 Years in Ethiopia (2016E_DHS).

Abbreviation: SNNPR, Southern Nations, Nationalities, and Peoples’ Region.
Women’s Access to Media
According to the study, 8485 (89.9%), 687 (6.3%), and 263 (2.8%) of the participants were not reading newspaper/magazine, read less than once a week, and read at least once a week, respectively. About two-thirds (66.4%) study participants didn’t listen to the radio, and 1628 (17.3%) and 1543 (16.4%) were listening less than once a week and at least a week, respectively, whereas more than two-third of the study participants didn’t watch television and 1833 (19.4%) and 1105 (11.7%) were watching television at least once a week and less than once a week, respectively.
Women’s Decision on Contraceptive Use in Ethiopia
The finding revealed only 2293 (24.3%) (95% CI: 23.7%, 25.1%) decision of contraceptive use was by women, and about 70% of the women decided to use contraceptive jointly with her husbands (Figure 1).
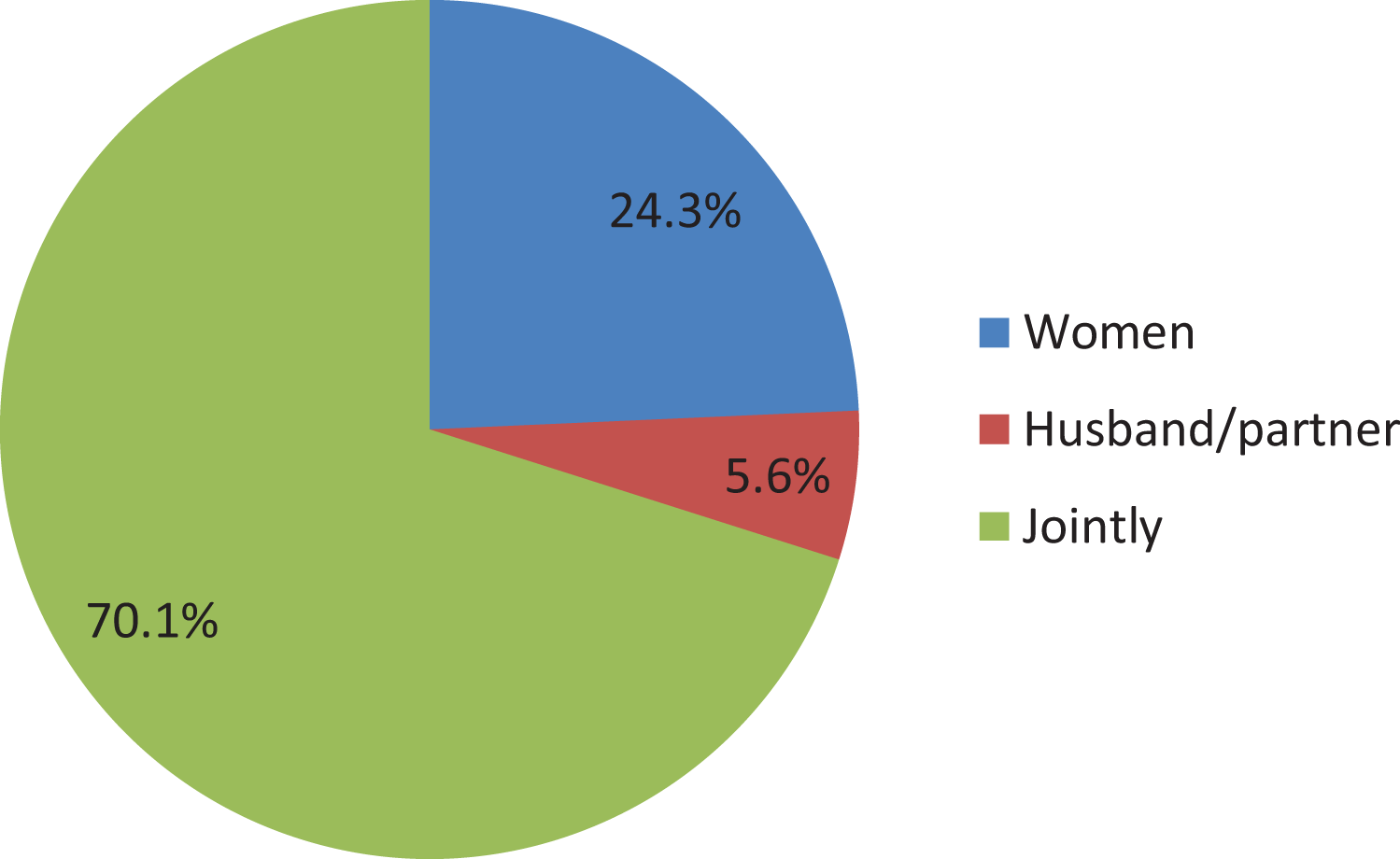
Distribution of women’s decision on contraceptive use in Ethiopia (2016E_DHS).
Factors Associated With Women’s Decisions on Contraceptive Use
By controlling other variables constant, women aged 15 to 19 years were 67.3% less likely to decide by themselves than jointly as compared to those women above 40 years (adjusted odd ratio [AOR] = 0.327, 95% CI: 0.175-0.613). Women who belong in the age group of 20 to 24 and 25 to 29 years were 49% and 44.3% less likely to decide on contraceptive use by themselves than jointly as compared to women aged above 40 years (AOR = 0.510, 95% CI: 0.390-0.666) and 25 to 29 (AOR = 0.557 95% CI: 0.460-0.675), respectively. Conversely, these women were 2.6 and 3.3 times more likely to decide by a husband than jointly as compared to women whose age above 40 years (AOR = 2.604, 95% CI: 1.576-4.302) and (AOR = 3.300,95% CI: 2.328-4.678), respectively.
Women who reside in urban were 1.64 times more likely to decide by themselves than jointly as compared to women from rural areas (AOR = 1.637, 95% CI: 1.331-2.015). Similarly, women who were from urban were 1.55 times more likely to decide by husbands than jointly as compared to women from a rural area (AOR = 1.55, 95% CI: 1.050-2.302).
Women who were from Oromia and Benishangul Gumuz region were 22% and 33.5% less likely to decide on contraceptive utilization by themselves than jointly as compared to women from Addis Ababa (AOR = 0.765, 95% CI: 0.590-0.991) and (AOR = 0.665, 95% CI: 0.494-0.897), respectively. Conversely, women who were from Harari regional state were 2.39 times more likely to decide by themselves than jointly as compared to women from Addis Ababa (AOR = 2.396, 95% CI: 1.826-3.144). Also, women who were residing in Amhara were 72.1% less likely to decide by their husband than jointly as compared to women from Addis Ababa (AOR = 0.279, 95% CI: 0.146-0.533). Similarly, women who were from the Benishangul and Harari region were 1.925 and 2.165 times more likely to decide by their husband than jointly as compared to women from Addis Ababa, respectively.
Women who were not working and unskilled workers were 1.266 and 1.386 times more likely to decide by women themselves than jointly as compared to women who are agricultural employees (AOR = 1.266, 95% CI: 1.019-1.574) and (AOR = 1.386, 95% CI: 1.067-1.801), respectively. Similarly, women whose husband were not working, work as a professional/technical/managerial, and engaged on services were 2.077, 2.363, and 3.228 times more likely to decide by husbands than jointly as compared to women who are an agricultural employee (AOR = 2.077, 95% CI: 1.494-2.887), (AOR = 2.363, 95% CI: 1.441-3.877), and (AOR = 3.228, 95% CI: 2.194-4.749), respectively. Women whose husband had no formal education and secondary education were 1.355 and 1.392 times more likely to decide by themselves than jointly as compared to women whose husband had higher education (AOR = 1.355, 95% CI: 1.033-1.777) and (AOR = 1.392, 95% CI: 1.080-1.794), respectively.
Women who had children less than 3 were 1.554 times more likely to decide by themselves than jointly as compared to women who had greater than 5 children (AOR = 1.554, 95% CI: 1.256-1.921). Similarly, those women who had children less than 3 and 3 to 5 children were 58.3% and 50% less likely to decide by their husbands than jointly as compared to those women who had greater than 5 children (AOR = 0.417, 95% CI: 0.279-0.417) and (AOR = 0.499, 95% CI: 0.386-0.645), respectively.
Regarding the wealth index, those women who were from poorer households were 1.542 times more likely to decide by themselves than jointly as compared to women from richest households (AOR = 1.542, 95% CI: 1.240-1.916).
Women who had higher and above education were 46.7% less likely to decide by themselves than jointly as compared to women who had no formal education (AOR = 0.533, 95% CI: 0.367-0.774). Similarly, those women who had secondary and primary education were 27.8% and 22.5% less likely to decide by themselves than jointly as compared to women who had no formal education (AOR = 0.722, 95% CI: 0.563-0.926) and (AOR = 0.775, 95% CI: 0.677-0.888), respectively. Women who had higher and above education were 2.941 times more likely to decide by their husband than jointly as compared to women who had no education (AOR = 2.941, 95% CI: 1.455-5.943).
Women who were not working had 1.377 times more likely to decide by themselves than jointly as compared to women who were working as agricultural employees (AOR = 1.377, 95% CI: 1.197-1.586). Again those women who work as clerical, sales, and service were 2.89, 1.30, and 1.78 times more likely decide by themselves than jointly as compared to those women who work as agricultural employees (AOR = 2.890, 95% CI: 1.644-5.082), (AOR = 1.300, 95% CI: 1.085-1.558), and (AOR = 1.778, 95% CI: 1.243-2.544), respectively. Women who engaged in skilled and unskilled manual work were 1.59 and 1.57 times more likely decide by themselves to utilize contraceptive than jointly as compared to those women who were working as agricultural employees (AOR = 1.588, 95% CI: 1.246-2.024) and (AOR = 1.574, 95% CI: 1.033-2.397), respectively. Concerning the accessibility to media, those women who read newspaper or magazine less than once a week were 51.9% less likely decide by their husbands than jointly as compared to women who did not read newspaper or magazine at all (AOR = 0.481, 95% CI: 0.272-0.851; Table 2).
Multinomial Analysis Between Modern Contraceptive Use and Various Background Characteristics.

Abbreviations: AOR, adjusted odd ratio; SNNPR, Southern Nations, Nationalities, and Peoples’ Region.
a= reference variable.
Discussion
This study identified that only 24.3% of women decide on contraceptive use by themselves. The result is almost in line with the study done in the Gedeo zone of southern nation nationalities and people of Ethiopia 14 and Mozambique. 4 The joint decision of the current finding was relatively higher than the study done in South Africa and Bangladesh, in which about 45% and 61% of women decide on the matter of contraceptive use jointly with their husbands or partners, respectively. 6,15 The possible explanation for the difference might be due to differences in socioeconomic differences between the countries, for example, in South Africa the majority of women decide by themselves. This may be because of the South African women were more educated than our study area.
Our finding revealed that age, place of residence, region, husband’s education, and occupation; total children ever born; and women’s education and occupation were significantly associated with the outcome variable.
Age negatively associated with women’s decision-making. Those women aged 15 to 29 years were less likely (P ≤ .001) to decide by themselves than jointly as compared to women aged above 40 years. Similarly, those women in the age-group of 20 to 34 were more likely to decide by their husbands than jointly as compared to women whose age above 40 years. The result clearly showed the decision-making power vested in the hands of their partners/husbands. This result is in line with the study done in Mozambique in which the decision-making power of women affected by their ages. 4
Residing in urban or in rural influences the decision-making of women. Those women who live in urban were more likely to decide by themselves than jointly as compared to women living in a rural area. The possible reason might be women who reside in urban were more educated, have information and awareness about the contraceptive compared to those women resided in rural areas. The result is in line with other studies conducted in the country and Mozambique. 4,14
Women who have no work and who were employed on unskilled work were more likely to decide by themselves. This result seems odd but the possible reason might be those women worry about their life since they have no regular income so that they decide by themselves. The result is similar to the study done in South Africa in which the women’s decision-making influenced by their current occupation. 15
Women whose husbands had no formal education or secondary education were more likely to decide by themselves as compared to women whose husbands had higher education. The result is similar to previous studies. The education status of women or husbands were the factors that affect the decision-making of women. 4,10,15 Similarly, those women who have less than 5 children were less likely to decide by their husbands than jointly as compared to those women who have greater than 5 children. The result indicated that women who have a lower number of children have more deciding power than those who have more than 5 children. The result is similar to a study done in the Gedeo zone in which having too many children affect women’s decision-making. 14 Women who had higher and above education were less likely to decide by themselves than jointly as compared to women who had no formal education. Similarly, those women who had secondary and primary education were also less likely to decide by themselves. On the contrary, women who had higher education and above were more likely to decide by their husband, this finding is in line with the study done in the Gedeo zone of Ethiopia, Mozambique, and South Africa. 4,14,15 Concerning the accessibility to media, those women who read newspapers or magazines less than once a week were less likely to decide by their husbands than jointly as compared to women who did not read newspapers or magazines at all. Reading newspaper and magazine improves the knowledge of women on contraceptive. 10
Conclusion
In conclusion, the finding revealed that the women’s decision-making on contraceptive utilization was low compared to the expected reality of women’s decision on her reproductive issue. But the majority of women decide jointly with their husbands or partners. Women’s decision on contraceptive use was influenced by many factors such as age of women, place of residence and region in which the women dwell, women and husbands education, occupation of both woman and her husband, and number of children were significantly associated with women’s decision for contraceptive use. Hence, policymakers and health managers should pay special attention to empower women to decide on their matters including contraceptive use. Moreover, due emphasis should be given about empowering women by all stakeholders including governmental and nongovernmental organizations during their plan and implementation.
Footnotes
Authors’ Note
All Z.K.E., T.F.D., and B.A.M. involved in conception of the idea, analysis, interpretation, and drafting of the manuscript. The data sets used and/or analyzed were available from the corresponding author on reasonable request. All authors have read and approved the submission of the manuscript. This study was conducted on secondary data from 2016 Demographic Health Survey. The DHS data were used only for the purpose of statistical reporting and analysis. All DHS data should be treated as confidential, and no effort should be made to identify any household or individual respondent interviewed in the survey. The consent is available at: ![]() .
.
Acknowledgments
The authors would like to thank Demographic Health Survey program office for the provision of the needed data for this study and Jimma University for providing of internet.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.