
Abstract
Background:
Antenatal care (ANC) is a preventive obstetric health-care program aimed at optimizing maternal fetal outcome through regular monitoring of pregnancy. Even if World Health Organization recommends a minimum of 4 ANC visits for normal pregnancy, existing evidence from developing countries including Ethiopia indicates there are few women who utilize it due to different reasons. The purpose of this article is to identify determinants significantly influencing the ANC visit utilization of child-bearing mothers in the Kaffa, Sheka, and Bench-Maji zones of Southern Nation Nationalities and Peoples Region, Ethiopia.
Methods:
A total of 1715 child-bearing mothers were selected. Several count models such as Poisson, negative binomial, zero-inflated Poisson, zero-inflated negative binomial, hurdle Poisson, and hurdle negative binomial regression models were fitted to select the model which best fits the data. The parameters were estimated by maximum likelihood. Measures of goodness of fit were based on the Rootogram.
Results:
The data were found zeros (8.1%); the variance (3.794), which is less than its mean (3.91). Hurdle Poisson regression model was found to be better fitted with the data given. Variables are selected by backward selection method, through the analysis, zones, residence, age at first pregnancy, source of information, knowledge during danger sin, willingness, time of visit, and satisfaction, which were major predictors of ANC service utilization. The estimated odds that the number of ANC visits those child-bearing mothers made (mothers who lived in urban) are 3.52 times more likely than mothers who lived in rural keeping others variables constant and the like.
Conclusion:
Based on our findings, a lot of effort needs to be made by health offices to create awareness, maternal health-care programs should be expanded and intensified in rural areas, improve women’s knowledge and awareness about the risk factor of late visit, the necessary investigations and follow-up throughout the antenatal period to promote regular attendance for ANC, and fulfill the client’s satisfaction.
Introduction
Background
Antenatal care (ANC) is a care provided by skilled health personnel to a pregnant woman throughout her pregnancy. 1 The primary aim of ANC is to promote and protect the health of women and their unborn babies during pregnancy so as to achieve at the end of a pregnancy a healthy mother and a healthy baby. Currently, it is regarded as a basic component of maternal health care on which the life of mothers and babies depends. 2 It is a key strategy for reducing maternal morbidity and mortality directly through detection and treatment of pregnancy-related illness or indirectly through detection of women at risk of complications of delivery and ensuring that they deliver in a suitably equipped facility. 3 Developing countries have low ANC coverage and there is a wide gap of ANC between mothers in developed and developing countries. In developed countries, 97% of women make at least 1 ANC visit. In developing countries, coverage of at least 1 ANC visit is low, that is, 69% in sub-Saharan Africa. 4 Complications of pregnancy and childbirth are the leading causes of disability and death among mothers in the reproductive age (15-49) groups in developing countries. 5 Ethiopia is also one of the countries with the highest maternal mortality ratios in the world. 6 In Ethiopia, an estimated 2.9 million women give birth every year. Of these, approximately 25 000 women and girls die each year and more than 500 000 suffer from complications including obstetric fistula. 7 As emphasized in the 2005 Ethiopian Demographic and Health Survey (EDHS), one explanation for poor health outcomes among women in Ethiopia was the non-use of modern health-care services. 8 Ethiopia has probably one of the highest and unacceptably high maternal mortality with 676 per 100 000 live births. 6 The high number of maternal deaths in some areas of the world reflects inequities in access to health services and highlights the gap between rich and poor. Almost all maternal deaths (99%) occur in developing countries. More than half of these deaths occur in sub-Saharan Africa and almost one-third occur in South Asia. More than half of the maternal deaths occur in fragile and humanitarian settings. The maternal mortality ratio in developing countries in 2015 is 239 per 100 000 live births versus 12 per 100 000 live births in developed countries. There are large disparities between countries, but also within countries, and between those women living in rural versus urban areas. 9
The quality of ANC is dependent on the qualifications of health providers and the number and frequency of ANC visits. 1 Adverse pregnancy outcomes can be minimized or avoided altogether if ANC is received early in the pregnancy and continued through delivery. The World Health Organization (WHO) and United Nations Children’s Fund recommend that a woman without complications should have at least 4 antenatal visits, the first of which should take place during the first trimester. Antenatal care represents a significant opportunity to reach a large number of pregnant women. 10
Ethiopia has strongly agreed. Reducing maternal health complication is directly or indirectly assured if and only if the child-bearing mother takes ANC service or visited doctor as well as health-care providers. Furthermore, the prevalence of the number of ANC service utilization of child-bearing women is absolutely low in developing countries. Regular antenatal visits are necessary to establish confidence between the woman and her health-care provider, to individualize health promotion messages, and to identify and manage any maternal complications or risk factors associated with child-bearing mothers.
There are many studies on the field of maternal care in which researchers often examined the effects of covariates on patients using logistic regression 11 models, but this model cannot account for the number of care a mother visited. Hence, such data can be more explored using Poisson, negative binomial (NB), zero inflated, and hurdle negative binomial (HNB) models. Because of counting, common data analysis procedures can be adopted directly. Therefore, to our best knowledge, there is a limited work in this line. With recognizing the underlying factors associated with the number of antenatal care visit utilization of child bearing mothers in three zones (Kaffa, Sheka and Bench-Maji zones) were attempted to study. In turn with the above veracity, the study attempted to turn up with possible clarification and commendation after having clear thought upon the state of affairs by giving owing emphasis to answer the following research questions: What is the prevalence of ANC visit utilization of child-bearing mothers in study area? What are the determinants significantly influencing ANC visit utilizations of child-bearing mothers in study area? Which statistical model is appropriately predicting well the number of ANC visit utilization of child-bearing mothers?
This study will help the stakeholders to reduce maternal and infant mortality and clarifying the main determinant factors that significantly affect the number of ANC visit utilization of child-bearing mothers. In general, the results of this study will give information to concerned bodies in setting policies, strategies, and further investigation for ANC visit utilization. The limitations of the current study were recalling bias during data collection; and nutritional and economic factors were not included.
Methods
Study Area, Source, Design and Sampling
The study was conducted in Kaffa, Sheka, and Bench-Maji zones. The southwest part of Ethiopia is a region in the country that contains one of the counties remaining moist Afromontane forest. Particularly, Sheka, Kaffa, and Bench-Maji zones are known for their natural forests with 60%, 20%, and 15% of forest cover, respectively. 12 Sheka zone is one of the few areas with high forest cover in Ethiopia. Due to the high level of dependency on forest resources, the local communities have developed traditional management practices based on religious taboos and customary practices. 13 The different relief features of the zone are the results of the geological episodes of the tertiary period and the subsequent geomorphic processes. The relief of Kaffa is generally characterized by a highly dissected rugged highlands in northern part and central majority and undulating lowlands in southern part. 14
The source of the data was primary data. A cross-sectional study design was carried out. The study population was all child-bearing mothers who had a birth in the 5 years preceding the survey in Kaffa, Sheka, and Bench-Maji zones. Kaffa zone has 10 woredas and 1 city administration, Sheka has 3 woredas and 1 city administration, and Bench-Maji zone has 10 woredas and 1 city administration. In this study, the dependent variable was the number of ANC visit utilization of child-bearing mothers. Sociodemographic and environmental characteristics were considered as the most important determinants of the number of ANC visit utilization. There is heterogeneity among the population living between rural and urban area, hence we are obliged to use stratification. Populations within woredas (districts) were clustered as first-stage clusters. Therefore, by using simple random sampling method, urban and rural woredas were selected from each zone.
Sample Size Determination
The sample size was calculated using a single-population proportion formula using the following parameters: confidence level, margin of error, and expected prevalence of the ANC visit of child-bearing mothers. Thus, considering P = .41 and deff = 1.66, the sample size for this study becomes
Statistical Models
Poisson Model
The natural stochastic model for counts is a Poisson point process for the occurrence of the event of interest. This implies a Poisson distribution for the number of occurrences of the event, with density
Negative Binomial Model
The NB regression model is a generalization of the Poisson regression model that allows for overdispersion by introducing unobserved heterogeneity term for observation i. Observations are assumed to differ randomly in a manner that is not fully accounted for by the observed covariates. In the NB model,
Zero-Inflated Models
The main motivation for zero-inflated count models is that real-life data frequently display overdispersion and excess zeros.
17,18
Zero-inflated count models provide a way of modeling the excess zeros in addition to allowing for overdispersion. For observation i, process 1 is chosen with probability
The probability of
When the probability
Hurdle Models
A hurdle model has the following parts: one zero hurdle part which models a right-censored outcome variable indicating mothers not visited (Y = 0) or mothers visited ANC (Y = 1, where all values larger than 0 are censored, that is, are fixed at 1), and one truncated count part that models the amount of ANC for those who visited ANC (for those with Y > 0). The hurdle model is flexible and can handle both under- and overdispersion problem. Hurdle model can be expressed:

yi
is the value of the dependent variable for the ith mother, i = 1,…, N, zi
is a vector of length J denoting the number of predictor variables in the zero part,
Results
Sociodemographic and Associated Factors of ANC
A total of 1715 child-bearing mothers who have a live birth in the last 5 years preceding the survey were interviewed from 3 zones (Kaffa, Sheka, and Bench-Maji), as shown in Table 1. One hundred thirty-nine (8.1%) of the child-bearing mothers had not received ANC service during their last pregnancy, while 1576 (91.9%) of the child-bearing mothers had received at least 1 time ANC service. In total, 1143 (66.6%) of child-bearing mothers had received 4 and more times ANC service, whereas 572 (33.4%) had visited less than 4 times during their last pregnancy. The average ANC visit utilization of child-bearing mothers in the 5 previous years of Kaffa, Sheka, and Bench-Maji zones were 3.91, 4.9, and 3.31, respectively. Averagely, Sheka zone child-bearing mothers were visited more than Kaffa and Bench-Maji zones.
Average Antenatal Care Visit Utilization of Child-Bearing Mothers.

Four hundred fifty-two (26.4%) child-bearing mothers were below the age of 20 years at first pregnancy and ANC was 3.96 averagely. The first pregnancy age of the most child-bearing mothers (766 [47.7%]) was between 20 and 24 years, with the average ANC of 3.9. Here, there were increasing variations (2.594) at first pregnancy attending ANC with an average of 3.53. However, most of the mothers were served ANC at the age between 25 and 29 years were 290 (16.9%), with the average 4.09, which are relatively better as compared to other age group of child-bearing mothers at first pregnancy. Nine hundred seventy-six (56.91%) respondents were rural women attending ANC 3.53 in average, whereas 739 (43.09%) were attending ANC 4.42 in average. For this, most of the mothers who live in urban were more prevalent of receiving ANC than those who live in rural. The one who may justify the reason is that there might be lack of health facility in rural area. However, 299 (17.43%) respondents were aborted, whereas 82.57% were not. This showed that there might be several WHO guidelines. Nine hundred sixty-five (56.27%) of the respondents were not knowledgeable about ANC for reducing the pregnancy complexity. Five hundred eighty-nine (34.34%) respondents or child-bearing mothers with their birth interval between 2 and 3 years inclusively received ANC 3.12 in average and more prevalent. Those mothers with the birth interval above 5 years have received ANC 4.83 in average which is greater.
In total, 1251 (72.94%) of the respondents or child-bearing mothers have been getting information about ANC from health profession and took ANC with 3.88 in average. A total of 1001 (70.03%) mothers were served ANC timely with the average 4.54. One thousand two hundred sixty-six (73.99%) child-bearing mothers come far from the service which was greater than 5 km and attending ANC with an average of 3.91. Of 1715 child-bearing mothers who received ANC visit, 390 (22.74%) were not satisfied with the service and attending ANC with the average of 2.69.
Table 2 reveals that 8.1% of the child-bearing mothers were not received ANC visit. The number of child-bearing mothers who attended 4 visits was 36.7%. The number of child-bearing mothers who attended ANC below 4 visits was 33.4%; and 4 and above visits were 66.6%; 91.9% of pregnant women have at least 1 ANC visit, and the majorities (66.6%) of women presenting any ANC have at least 4 visits.
Antenatal Care Visit Utilization of Child-Bearing Mothers in Study Area.
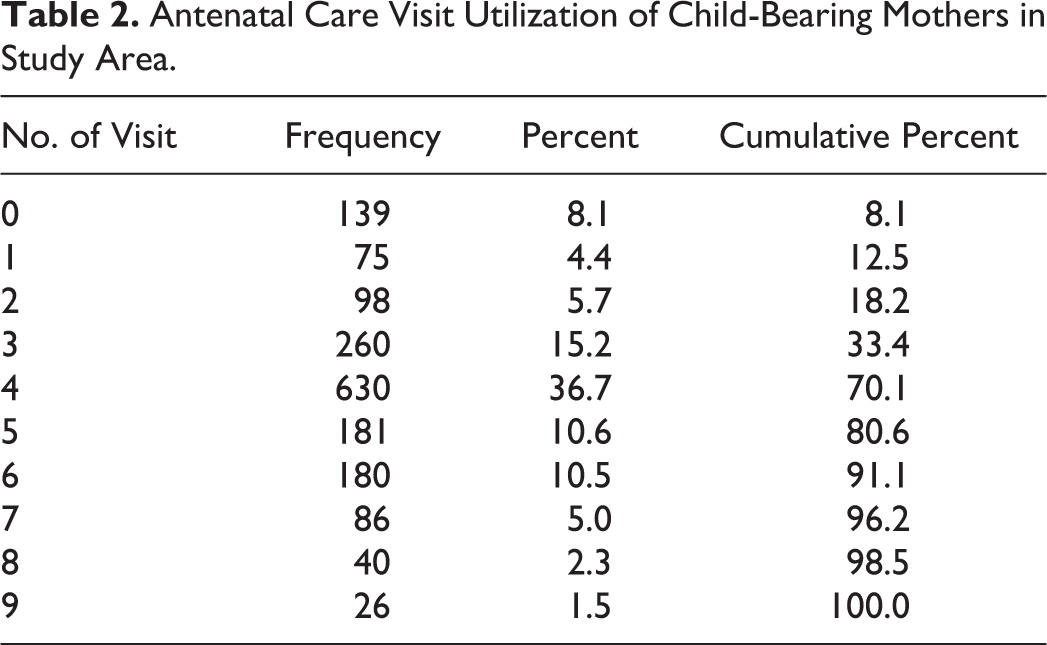
The maximum and the minimum visits were 9 and 0, respectively, and the usual Poisson regression model would underestimate the data since the mean (3.9137) is greater than variance (3.794; no zero inflation data). For this, the NB model also is not recommended to model the data. Thus, the data may be accommodated by further extension of Poisson regression models.
Model Selection and Associated Factors of ANC
The count data models compared using Akaike information criterion (AIC). To incorporate all variables into the model-building workflow for count data regression models, their model information would be used to complement standard techniques such as information criteria (AIC). Using a basic model for the number of ANC visit data (eg, Poisson vs NB models) and/or extra zeros (e.g., hurdle or zero-inflation) are relevant issues in the data at hand. The models upon which the variables are based should use a reasonable first selection of regressors (a standard specification from the literature or a model involving all potentially relevant variables). In much literature reviewed that the models with smallest AIC value is the better one and therefore, hurdle Poisson regression model (Table 3) is responsible for model or account for this data. However, the AIC value for hurdle Poisson and HNB model are nearly the same and needs to be compared using Vuong z-statistic. The hurdle Poisson model, the HNB model, and the nonsignificant Vuong statistic (0.6593, P > .05) indicated that the hurdle Poisson model and the HNB model showed comparable fit. However, the HNB model contains 2 parameters and more flexible than HP model; the theta for HNB is very large. It indicates that the conditional variance of NB model approaches to the Poisson model which shows that there is no overdispersion in the data. Thus, the final model using backward elimination method of the last step associated with smallest AIC value and the parametric estimates of selected variables for the model is given in Table 4. The odds ratio for child-bearing mothers in Bench-Maji zone equals exp(−2.630) = 0.072 (adjusted for the other variables), which implies that those mothers in Bench-Maji zone are 0.072 times less likely to visit than those mothers in Kaffa zone (Table 4). In other words, the odds of the number of visit are significantly higher for mothers in Kaffa zone. However, Sheka zone contributes significantly to amount of visit; from count part, we find that the adjusted rate ratio for Sheka zone is exp(0.235) = 1.265. Although zone contributes to the number of visit, this predictor plays no significant role in modeling the number of not visit (zero part). The odds ratio for child-bearing mothers in urban area equals exp(1.258) = 3.518 (adjusted for the other variables), which implies that those mothers in urban are 3.518 times more likely visited than those mothers in rural area. In other words, the odds of the mothers not visited are significantly higher in rural area. Although residence contributes to the number of visit, this predictor plays no significant role in modeling the number of visit (count part).
Model Comparison Using Akaike Information Criteria.

The Hurdle Poisson Model for ANC Visit for the Selected Variables.

a P < .001.
b P < .05.
c P < .01.
The odds ratio for child-bearing mothers not volunteering equals exp(−1.689) = 0.185 (adjusted for the other variables), which implies that those mothers who do not volunteer are 0.815 times less likely visited than those who volunteer. The odds of the number of visited are significantly higher for child-bearing mothers who volunteer. The odds ratio for child-bearing mothers not satisfied equals exp(−1.401) = 0.246 (adjusted for the other variables), which implies that those mothers not satisfied are 0.246 times less likely to visit ANC than those mothers satisfied during visit. The odds of the ANC visit are significantly higher for child-bearing mothers satisfied during pregnancy. Although satisfaction of mothers contributes to the number of visit, this predictor plays no significant role in modeling the number of visit (count part). The odds ratio for child-bearing mothers whose age of first pregnancy between 20 and 24 years equals exp(−0.95) = 0.387 (adjusted for the other variables), which implies that those mothers whose age of first pregnancy between 20 and 24 years are 0.387 times less likely to visit ANC than those mothers whose age is less than 20 years. The odds ratio for child-bearing mothers whose age of first pregnancy between 25 and 29 years equals exp(−1.398) = 0.247 (adjusted for the other variables), which implies that those mothers whose age of first pregnancy between 25 and 29 years are 0.247 times less likely to visit ANC than those mothers whose age is less than 20 years. The odds ratio for child-bearing mothers whose age of first pregnancy between 30 and 34 years equals exp(−1.489) = 0.226 (adjusted for the other variables), which implies that those mothers whose age of first pregnancy between 30 and 34 are 0.226 times less likely to visit ANC than those mothers whose age is less than 20 years. The odds ratio for child-bearing mothers whose age of first pregnancy ≥35 years equals exp(−3.003) = 0.049 (adjusted for the other variables), which implies that those mothers whose age of first pregnancy is ≥35 are 0.049 times less likely to visit ANC than those mothers whose age is less than 20 years. The odds ratio of the ANC visit is significantly higher for child-bearing mothers whose age of pregnancy is less than 20 years of age. The rate ratio for child-bearing mothers not knowledgeable about danger sign during pregnancy equals exp(−0.172) = 0.841 (adjusted for the other variables), which implies that those mothers not knowledgeable were 0.841 times less likely visited than those mothers knowledgeable about danger sign during pregnancy. Although danger sign contributes to the number of visit, this predictor plays no significant role in modeling the number of visits (zero part). The rate ratio for child-bearing mothers come from distance ≥5 km equals exp (−0.071) = 0.931 (adjusted for the other variables), which implies that those mothers come from distance ≥5 km are 0.931 times less likely to visit than those mothers come from nearby. The rate of the ANC visit is significantly higher for child-bearing mothers who come from nearby. Although distance from service contributes to the number of visit, this predictor plays no significant role in modeling the number of visit (zero part).
Clearly, the model underestimates the probability of zero counts and the mean of zero-inflated models solves the problem of excess zeroes, predicting that 5% of the women’s will not visit ANC, which is less than the observed value of 8.1%. It probably tells us no more excess zero counts being predicted in the model. So the model predicting 95% of the child-bearing mothers will visit ANC at least once, which is greater than the observed value of 91.9%.
For a Poisson distribution, we see general much poor agreement between the expected and observed counts, with the 0 and 4 counts are underpredicted while counts between 1 and 3 and large are overpredicted (Figure 1). Also, for a NB distribution, we see a much poorer fit, the 4 to 7 counts are underpredicted whilst some low counts are overpredicted. The Rootogram for the hurdle Poisson and HNB shows much better agreement than the other models. Departures from expected counts are much smaller and count model is much better fitted. Some small deviations from the observed data remain but that is to be expected (Figure 1).
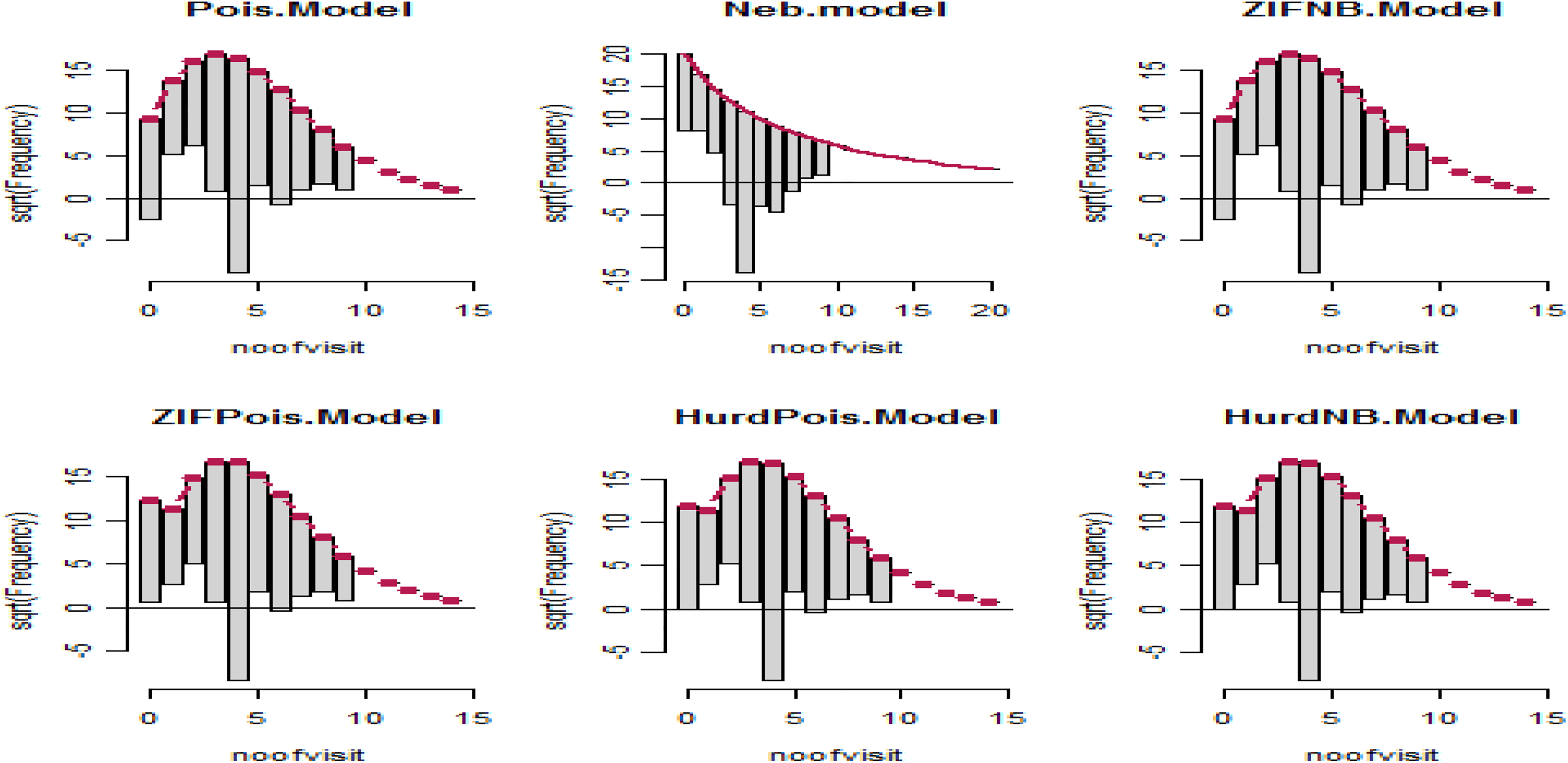
Hanging Rootograms for count regression models of antenatal care visit utilization.
Discussion
Antenatal care service visits could be a relevant metric to quantify efficiency of maternal care utilization. This study focused on statistical modeling of ANC visit utilizations, model used as Poisson regression, and its extension like zero-inflated and hurdle modeling approach to estimate parameters of demographic and socioeconomic and environmental-related factors. World Health Organization recommends a minimum of 4 ANC visits initiated during their pregnancy periods.
In the current study, from 1715 women who gave birth at least once within the last 5 years before the survey were interviewed from 3 zones (Kaffa, Sheka, and Bench-Maji). The child-bearing mothers who attend ANC below 4 visits were 33.4% and who attend above 4 visits were 66.6%; 91.9% of pregnant women have at least 1 ANC visit, and the majorities (66.6%) of women bearing child have at least 4 visits, but in the study done in Goba woreda, Ethiopia, 20 478 (85.1%) of them had ANC visit during their last pregnancy. Majority of study participants, 396 (82.8%), made less than 4 ANC visits during their last recent pregnancy. In a study conducted 21 in Ethiopia, 48.5% of mothers had at least 1 visit, which is much less than the current study. The current study is lower than the study conducted in developed countries, 97% of women make at least 1 ANC visit; however, it is much more high as compared to the study conducted in developing countries with coverage of at least 1 ANC visit; that 69% in sub-Saharan Africa 22 and as observed in 2005 EDHS, only 28% of mothers received ANC from a health professional for their most recent birth. 8,23 A study conducted in southern Ethiopia in 2003 showed that the proportion of women who received ANC for their most recent birth in the 6 years preceding the survey was 26.1%, which is much less than the current study.
This study revealed that means of information, transportation status, knowledge about danger sign, satisfaction, residence, and age at first pregnancy were significantly associated factors of ANC visit utilization. This study is consistently supported by study conducted 24 in Kenya which demonstrated that an increase in distance to the nearest health-care facilities was associated with fewer antenatal visits. Distance to the health facility is inversely associated with ANC utilization. 25 Sociodemographic factors including age at first pregnancy appeared to influence the use of maternity care services utilization. 26 Several studies conducted in different countries on demographic and sociocultural factors influencing the use of maternal health-care services have shown that factors like maternal age, number of living children, education, place of residence, occupation, religion, and ethnicity are significantly associated with the use of ANC. 27
The current study showed that the age at first pregnancy is significantly influencing the utilization of ANC, and it is supported by the study on maternal age which has been shown to be both negatively and positively influenced by utilization of ANC in general. The study also showed that the attendance was higher for pregnant women whose age at first pregnancy was below 20 years. It is supported by a nationally representative sample survey in Ethiopia; receipt of maternity care was found to vary by age, and other sociodemographic factors 2 and the study on teenage mothers were more likely to start utilizing ANC services earlier than their older counterparts. 28 However, other studies conducted in Turkey demonstrated that teenage mothers were statistically less likely to use ANC services 29 and utilization of ANC services among teenage mothers remains significantly poor in Malindi sub-county. Immense efforts should be directed toward creation of awareness about ANC and its importance in the communities and implementation of innovative programs targeting pregnant teenage girls to encourage them to seek ANC services. 30
The current study showed that the place of residence has also been shown to influence ANC utilization; women in urban areas were more likely to use ANC than rural women. The reason for the high level of utilization of maternal health services among urban women compared with their rural counterparts is easily understood. This study is consistently supported by Kwast and Liff, 31 as in most sub-Saharan countries, urban women in Ethiopia tend to benefit from increased knowledge and access to maternal health services compared with their rural counterparts. This is because, health facilities are more accessible in urban areas and the various health promotion programs that use urban-focused mass media work to the advantage of urban residents and explain the close connection between urban residence and use of maternal health services. Moreover, rural women are more readily influenced by traditional practices that are contrary to modern health care. On other hand, the study is not consistent with Ecuador 32 and Nepal, 33 also study by Navaneetham and Dharmalingam 34 in India found that women in urban areas of Karnataka were less likely to receive ANC than those living in rural areas. The study findings show the actual rural setting of ANC services’ attendance and utilization. Much sensitization has to be done specifically in these rural areas to empower pregnant women and their husbands as to improve ANC attendance and utilization. 35 The current study showed that the knowledge of child-bearing mothers about danger sign during pregnancy for ANC is low. This study is consistently supported by Kwast and Liff, 31 in their study of maternal mortality in Addis Ababa, which showed that women who did not receive maternity care have limited knowledge of maternity care services. The study is consistently supported by studies that have shown that adequate knowledge of ANC has a positive and statistically significant effect on ANC use. 32,36 The study conducted by Ndyomugyenyi 37 in Uganda indicated that pregnant women with inadequate knowledge of maternal and child health were less likely to utilize ANC than those mothers who have knowledge about danger sign. There may be factors on the demand side like the women’s empowerment, financial support of the husband, knowledge of ANC visits in the context of timing, frequency, and the expectations of ANC visits which might be mediating the effects through the factors found associated in this study. Irrespective of the knowledge about the precise mechanism of action, policy makers could focus on improving women’s empowerment, improving women’s education, reducing wealth inequity, and facilitating improved utilization of ANC through modifications on the supply side factors such as geographic location and focus on hard-to-reach women. 38
The current study showed that the number of visit is significantly higher for child-bearing mothers visited timely. The study is consistent with the study by WHO and UNICEF, 39 in which ANC contributes to good pregnancy outcomes and often times benefits of ANC are dependent on the timing and quality of the care provided. Regular ANC is necessary to establish confidence between the woman and her health-care provider, to individualize health promotion messages, and to identify and manage any maternal complications or risk factors, 40 which is consistent with the current study. The main reasons for nonattendance at ANC clinic were related to being in good health and poor quality of service. It was also observed that nonattendance was higher for those with unplanned pregnancy, low knowledge of unhealthy pregnancy, and those whose husband or partner’s attitude to ANC attendance was negative. In conclusion, the study revealed that sociodemographic factors were found to be barriers to utilization of ANC services and the overall ANC utilization is higher 88.9%. 41
Conclusion
In the last parsimonious statistical model and the backward variable selection method, zone, residence, age at first pregnancy, source of information, willingness, timely visit, satisfaction, and iron foliate were major predictors of ANC service utilization. The ANC offers tremendous opportunities to reach a large number of women and communities with effective clinical and health promotion interventions. Mothers in Benchi-Maji zone, rural area, source of information(traditional delivers), not willingness, not satisfied, not timely visit, age of first pregnancyyears, not aware during pregnancy, distance women's may not benefit from ANC services or may drop out due to access barriers and low quality services. In this study, it was found that hurdle Poisson regression models were better fitted the data than NB, ZINB, HNB, ZIP, and Poisson. This may be due to the low or high variability of the number of ANC visits. Hurdle Poisson regression model was better fitted the data, which is characterized by both under- and overdispersion problem. Based on our findings, a significant change needs to be instituted by health offices to create awareness; maternal health-care programs should be expanded and intensified in rural areas; improve knowledge of women and awareness about the risk factor for late visit, the necessary investigations and follow-up throughout the antenatal period to promote regular attendance for ANC; and fulfill the client’s satisfaction.
Footnotes
Authors’ Note
Local administration of the wards helped us unlimited contribution. Respondents gave us a valuable response for the betterment of the study. Ethical clearance and approval were obtained from Mizan-Tepi University. Permission letter was obtained from district health office. Participants were informed whether their participations are voluntary. Oral informed consent obtained from participants. Confidentiality and anonymity were ensured. Springer Nature remains neutral with regard to jurisdictional claims in published papers and institutional affiliations.
Acknowledgments
All who contributed for data collection are duly acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was fully funded by Mizan-Tepi University. However, they have no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.