
Abstract
Introduction:
An integrated health and social care program for patients with heart failure (HF) was implemented at the Friuli-Venezia Giulia deployment site as part of the SmartCare European project. The objective of this study was to validate 2 different decision modeling techniques used to perform the economic evaluation.
Methods:
Data were collected during the SmartCare project which enrolled 108 patients with HF and followed for more than 6 months. The techniques used were Markov and discrete event simulation models. In both cases, a cost-effectiveness analysis and a budget impact analysis were carried out. The former was used to assign priority to the intervention and the latter to assess its sustainability. Analyses were conducted from the perspective of the Regional Health Authority.
Results:
Results were similar with both types of model. Cost-effectiveness analysis found no significant differences in quality of life, but the intervention generated significant cost savings, becoming the dominant option. Data extrapolation showed no benefits in terms of mortality or hospital admissions, but budget impact analysis also predicted annual savings, as a significant number of in-hospital days were avoided. In budget analysis, both models predicted early, increasing and cumulative annual savings.
Discussion:
The integrated program was dominant as it provided better outcomes and lower total costs, and thus, decision-makers should prioritize it. Besides, the work demonstrates the capacity of decision modeling to become a complementary tool in managing integrated health and social care models.
Introduction
Within the SmartCare project, an integrated health and social care program for patients with heart failure (HF) was deployed in Friuli-Venezia Giulia (FVG). 1 Modeling in pharmacoeconomics is based on standard techniques that have been extensively described. 2 The application of this approach to integrated care is still, however, in an early phase. To undertake the economic evaluation of the integrated intervention, 2 different ways to represent the natural history of HF were tested. First, a 4-state Markov model was built to represent the intervention carried out in the FVG region and to foresee its impact. 3 Secondly, seeking to validate an alternative modeling approach, a discrete event simulation (DES) model was also built to again reproduce the intervention undertaken. 4,5
The objective of this study was to carry out the economic evaluation of an integrated health and social care program for HF through 2 different modeling techniques at the FVG deployment site, comparing the results of the 2 techniques.
Method
Two modeling approaches were applied to represent the natural history of patients with HF. 6 –10 Data concerning this population for the years 2012 to 2015 were compared with data collected during the project and adjusted to better represent the trends observed in population aging, HF prevalence, management, and outcomes. The economic evaluation of the program was performed using Markov and DES model approaches. In both cases, 2 different but complementary analyses from the perspective of the Regional Health Authority of FVG comparing the SmartCare intervention to usual care services were carried out, 11 –13 a cost-effectiveness analysis (CEA) on a 5-year time horizon and a budget impact analysis (BIA) over 10 years. While CEA was expected to help prioritize interventions, BIA was perceived as useful in assessing their sustainability, a major concern for budget holders. 14
The target population of the SmartCare project was patients older than 65 years, with moderate to severe HF, diabetes mellitus or chronic obstructive pulmonary disease, and social needs. All patients gave written informed consent before inclusion. The SmartCare approach in FVG was based on a full integration of information communication technology (ICT)-supported interaction between health-care and social care providers and also with care recipients, caregivers, and the third sector to promote more active involvement by all these players. 1
Cost-Effectiveness Analysis
During the SmartCare project, 108 patients with HF have been enrolled and followed in the FVG pilot for more than 6 months. Data collected are presented in the Supplemental Material. As no differences have been found in quality of life (QoL) between the 2 groups, the worst case scenario was adopted for the integrated care group, that is integrated care had no impact on QoL. Estimates of utilities and assumptions concerning decline in QoL with age as well as after each hospital admission have been made based on data from Gohler et al. 15 Unit costs were provided by the representatives of the region. Data for the population projections were obtained from the Italian National Institute for Statistics. Transition probabilities, utilities, and unit costs used for the analyses are listed in Table 1. All estimates were in euros (€), and the primary outcome measure was the incremental cost–utility ratio, that is, the incremental cost per quality-adjusted life year (€/QALY). For the Markov approach, model building and analysis were performed with TreeAge Pro Healthcare software supported by Microsoft Excel modules, while for the DES approach, a microsimulation model was built using Arena software, a simulation tool from Rockwell Automation.
Parameters Used in the Study With Their Value and Source.
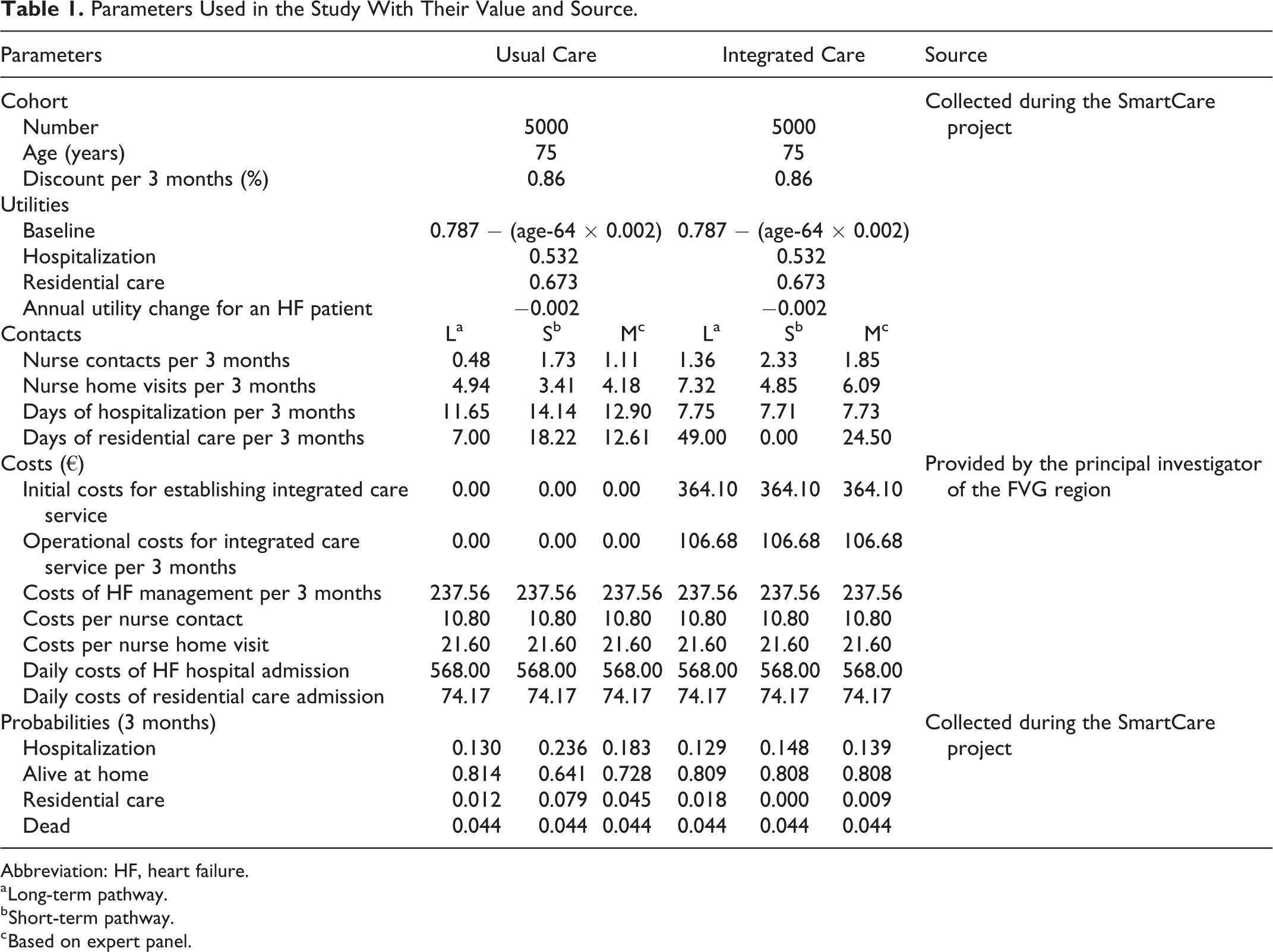
Abbreviation: HF, heart failure.
a Long-term pathway.
b Short-term pathway.
c Based on expert panel.
Both approaches were used to reproduce the traditional and the integrated care systems of FVG and both considered the same 4 states: alive at home, hospitalization, residential care, and dead. Transition probabilities between states were also the same. As far as the use of different resources are concerned, data for long-term pathways were used for the alive at home state, data for short-term pathways for the hospitalization state, and data for a mean of long- and short-term pathways for the residential care state. Figures in the Supplemental Material outline the conceptual model used in each approach. Patients enter into the models after a hospital admission and start with the short-term pathway transition probabilities. The age at which patients enter the models was set at 75 years. The reference year was 2016 and the basic time horizon 5 years. A 3-month cycle length was adopted, which corresponds to the short-term pathway duration. Future costs and benefits were discounted at 3.5% per year in the base scenario. The utility in the dead state was 0, and for the other health state utilities, an annual reduction of 0.002 was applied. In each state, the costs of HF management, contacts with nurse, and nurse home visits were summed for each cycle. Daily in-hospital costs multiplied by the length of stay were also added for each cycle for the hospitalization and the residential care states. Only one admission to hospital or residential care was considered per cycle. The cost of the disease for the integrated care system was obtained in the same way as for traditional care but with 2 differences. First, at the beginning, the initial cost of establishing the integrated care service was added once. Second, the operational cost for the integrated care service was added for each cycle.
Budget Impact Analysis
The objective of BIA was to assess the financial consequences of developing the ICT-enabled integrated care program and its sustainability in the short and medium term. 16 –18 For the Markov model approach, the BIA was performed in Microsoft Excel following the structure of the costing templates produced by the British National Institute for Health and Care Excellence in accordance with official guidelines. 13 For the DES approach, the BIA was developed from the microsimulation model using Arena. It was assumed that there was a gradual evenly distributed uptake of ICT-enabled integrated care over this period, with an annual increase of 10% for the first 6 years and then 5% until year 10. Based on data from the Regional Health Authority and the capital city of the region, the prevalence of HF was estimated at 0.96%. An annual increase of 0.0256% was applied to take into account that the population of patients with HF is likely to grow because of aging of the general population. 19 Further, only 50% of this population was eligible for ICT-enabled integrated care.
For both approaches, the conceptual models and states used in the BIA were the same and worked in the same way as in the CEA. Unit costs were also the same as those used in the CEA and the financial streams for each budget period were presented as undiscounted costs. 17 Both models considered the impact of hospitalizations for any cause in the budget impact calculations. 7 They did not include the impact of integrated care on productivity, social services, and other costs outside health-care. 17 Resource consumption and costs in both scenarios were projected 10 years into the future, taking into account the effect of population aging. The difference in the total cost between the 2 scenarios represented the budget impact associated with the introduction of ICT-enabled integrated care. Costs were disaggregated per year.
Results
For the CEA, Table 2 shows the results obtained with the Markov model in the first row and those obtained with the microsimulation model in the second row. As can be seen, the results were similar with both types of model. Both approaches showed that in terms of QoL, there were no significant differences attributable to integrated care services, with only a slight improvement. However, the integrated care model generated significant cost savings, about €6000 per patient according to the Markov model and about €4000 per patient according to the DES model.
Cost-Effectiveness Analysis Results Using Markov Model and Discrete Event Simulation Model.

Abbreviations: DES, discrete event simulation; QALY, quality-adjusted life year.
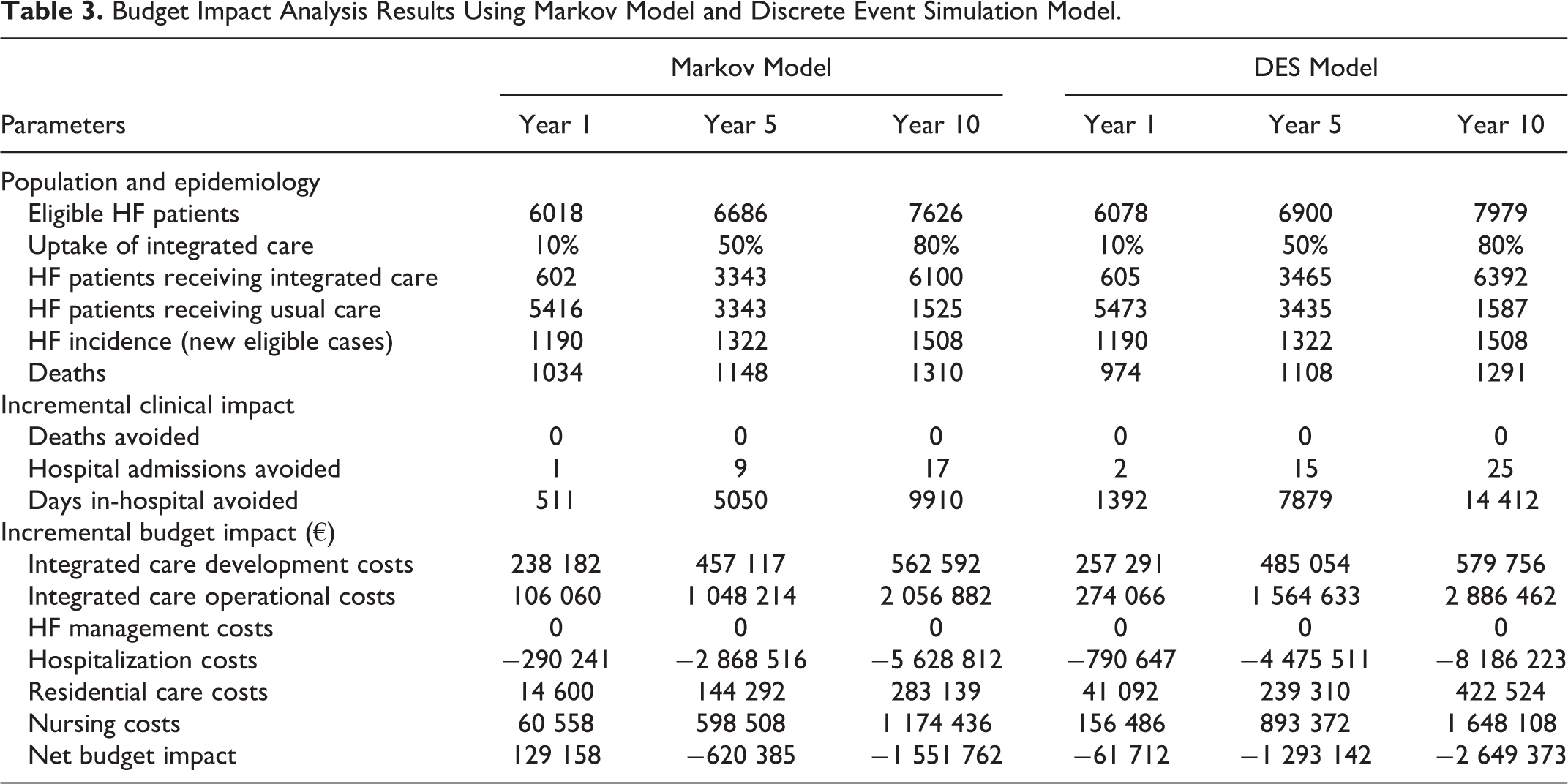
Table 3 shows the net BIA results of the Markov and DES models. Although the budget was calculated for 10 years, only the first, fifth, and tenth years of the follow-up are presented in the table. As in the previous analysis, the results are similar and follow the same trend from year to year, but this time, the cost savings obtained with DES model are higher. Both studies showed that, within a population of about 1.2 million, around 3500 patients would receive ICT-enabled integrated care services over a time horizon of 5 years. In the fifth year, integrated care and usual care would have the same share of care recipients. The results of the 2 models also showed no benefit in terms of mortality and only a slight benefit in terms of hospital admission. Nevertheless, a significant number of days in hospital were avoided due to the integrated care services. Therefore, both models predicted early, increasing and cumulative annual savings starting from the first year with the DES model and from the second year with the Markov model. Savings in the last year were over €2.6 million for the first case and €1.5 million for the second.
Budget Impact Analysis Results Using Markov Model and Discrete Event Simulation Model.
Discussion
This work demonstrates the capacity of decision modeling to become a complementary tool in managing integrated health and social care models. 20 In the literature, there are few examples of integrated organizational model evaluations aimed at the HF management. 21 –23 The new technologies introduced, the multiple actors connected, and the need to change the behaviors of professionals involved made the implementation of the integrated model of HF in FVG a complex intervention. In this context, the CEA was useful to estimate the increase in effectiveness in terms of costs and the BIA to represent the burden of HF management and the impact of the intervention. Both were completed with complementary approaches, adopting either the Markov or the DES model, and obtained the same results when they applied the same parameters. The combined application of simulation methods enabled symbiotic realization of the strengths of each of the techniques, while reducing their limitations. In this way, the results obtained with the DES model have acted as a cross-validation for the results previously obtained with the Markov model.
The CEA demonstrated that the integrated program is dominant as it provided better outcomes and lower total costs and, thus, decision-makers should prioritize it. 24 For their part, most regions in Europe have included a request for the BIA as part of the evidence base to support reimbursement. 14 Extrapolation of expenditure should include the objectives set by the expert group, in order that managers can evaluate the intervention systematically. Comparing the actual resource consumption with the expected values over time allows an evaluation of the deviation between the goals determined for the BIA and the reality at each stage. If the results measured coincide with the objectives over time, this will suggest that work is progressing in the right direction. Otherwise, the deployment and/or the intervention should be reconsidered. 21,23 In this study, the BIA shows the potential of the integrated care model to reduce days in hospital and how this benefit increases over time. Although the ICT-enabled integrated care was associated with a significant investment for the development of the service (ICT infrastructure, staff training, etc) and even more significant operational costs, these costs were outweighed by the savings generated by significantly reducing days in hospital. These savings also outweighed the increasing cost of residential and primary care.
From the view point of the health-care system, the integration of home telemonitoring within an organized care system is critical for the success of an HF program. Telemonitoring should be an addition, not an alternative, to the classical model of integrated care, allowing the sharing of patient information and facilitating, intensifying, and personalizing disease management through proactive and effective multidisciplinary intervention, provided by experienced care providers. As a limitation of the economic evaluation, we should note that this study did not analyse the hurdles to scaling up of the intervention to the whole region, 25,26 which means overcoming the challenge of applying it at multiple points of care. 26 This is bound to entail challenges related to change management, which need to be addressed with the help of appropriate coaching and knowing that resistance of professionals to change has been indicated by the SmartCare deployment sites as the major obstacle to organizational innovation and as the area where external support is most needed.
Supplemental Material
Supplementary_File - Economic Evaluation of an Integrated Health and Social Care Program for Heart Failure Through 2 Different Modeling Techniques
Supplementary_File for Economic Evaluation of an Integrated Health and Social Care Program for Heart Failure Through 2 Different Modeling Techniques by Igor Larrañaga, Panos Stafylas, Ane Fullaondo, Gian Matteo Apuzzo, Javier Mar, and on behalf of the SmartCare Modeling Group in Health Services Research and Managerial Epidemiology
Footnotes
Acknowledgments
SmartCare modelling group (Partner: Members): Osakidetza-Basque Health Service, Spain: Javier Mar, Igor Larrañaga, Myriam Soto-Gordoa. Health Information Management, Belgium: Marco D’Angelantonio, Panagiotis Stafylas, Stavros Chatzopoulos. Kronikgune, Spain: Esteban de Manuel, Ane Fullaondo. University Hospital and Health Services of Trieste, Italy: Gian Matteo Apuzzo, Andrea Di Lenarda, Donatella Radini.
Author Contributions
I.L. designed the study with the assistance of J.M. and P.S. I.L. built up the microsimulation model and wrote the initial draft with the assistance of J.M. I.L. and J.M. wrote the methodological and results sections. P.S., A.F., and G.M.A. participated in the design, reviewed all the clinical and epidemiological data, and drafted the introduction and conclusions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is partially funded under the ICT Policy Support Programme (ICT PSP), grant agreement number 325158. Nevertheless, this work reflects only the author’s views and that the Union is not liable for any use that might be made of information contained therein.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.