
Abstract
Purpose:
Disabled individuals younger than 65 years are entitled to Medicare coverage through the Social Security Disability Insurance (DI) program, but only if they have completed a 2-year waiting period. This is the first study that uses longitudinal panel data, the Health and Retirement Study, and examines whether and to what extent the health and economic status are affected among disability beneficiaries who are uninsured during the Medicare waiting period.
Methods:
In a quasiexperiment research design, using a difference-in-difference (diff-in-diff) estimator, we compare changes in health and economic outcomes pre-/postentering the DI program for disability beneficiaries with alternative public health insurance and those without.
Results:
The adjusted diff-in-diff estimates suggest that disability beneficiaries who are uninsured during the waiting period, compared to those who are insured, are 13.6 percentage point more likely to report poor health, 6.3 percentage point less likely to be in excellent health, declare more difficulties in activities of daily living, and 30% higher medical expenditures from out of pocket.
Conclusions:
The findings highlight punitive health and economic effects of the Medicare waiting period for uninsured disability beneficiaries. We also discuss the implications of the findings for the Affordable Care Act reform.
Keywords
Introduction
Medicare is a federally administered social insurance program in the United States that guarantees access to health insurance for individuals aged 65 and older and younger individuals with disabilities who have worked and contributed to the system. In 2013, while disability beneficiaries comprise 16.8% of the total Medicare population, they account for more than 20% of the total program expenditures. In the last decade, the growth of Medicare enrollment from disability beneficiaries has greatly outpaced the overall growth of Medicare program. For example, using data from the Chronic Condition Data Warehouse Medicare 5% sample from Centers for Medicare and Medicaid Services, we estimate that from the year 2003 to 2012, the growth of disabled beneficiaries (37%) is much faster than the growth of the aged beneficiaries (21%). As baby boomers age, they are reaching an age of increased likelihood to developing disabilities, which makes it more important to understand the disability beneficiaries under Medicare. However, younger Medicare beneficiaries with work disabilities have received far less research attention and policy consideration than elderly Medicare beneficiaries. This article contributes to the thin literature on Medicare disability beneficiaries.
The disabled individuals receive Medicare coverage through the Social Security Disability Insurance (DI) program, a primary public transfer program that provides both partial earnings replacement and Medicare coverage to workers who lost earnings capacity due to severe and long-term disabilities. The Social Security definition of disability refers to severe health limitations that prevent individuals from engaging in any substantial gainful activities and are expected to last at least 12 months. As of December 2013, the DI program provides cash benefits and Medicare coverage to nearly 11 million American workers and their eligible dependents. 1 Most DI beneficiaries are required to complete a 5-month waiting period before they are entitled to cash benefits and an additional 24-month waiting period before they are entitled to Medicare coverage (the 2-year Medicare waiting period is waived for those with amyotrophic lateral sclerosis and those with end-stage renal disease). There has been considerable concern that the 2-year Medicare waiting period causes significant hardship to new DI beneficiaries who lack alternative health insurance coverage and needed health care access to address their health problems. Evidence shows that more than 20% of DI beneficiaries have no health insurance coverage at all during the Medicare waiting period. 2,3 Around 1.8 million DI beneficiaries were in the waiting period for Medicare coverage in 2008. 4 Congress has noted the problems with the 2-year waiting period in the Ticket to Work and Work Incentives Improvement Act of 1999. Other political effort devoted to changing this policy includes the Ending the Medicare Disability Waiting Period Act of 2007, sponsored by Senator Jeff Bingaman and Rep. Gene Green, which proposes to phase out Medicare’s 2-year waiting period over a 10-year span and grant more exceptions to people with life-threatening health conditions. Studies based on focus groups and interviews with disabled individuals have shown that many of the uninsured lack needed health care to stabilize their health conditions and their situations get worse during the waiting period. 5 –8 Yet formal analyses have been rare that identify and quantify any detrimental effect that the 2-year waiting period has imposed on disabled individuals. A handful of previous studies about the Medicare waiting period have primarily focused on estimating the fiscal impact of eliminating the 2-year waiting period, which is certainly useful for budgetary consideration of policy changes. 2,3,9 A demonstration project (the Accelerated Benefits [AB] Demonstration) conducted by the Social Security Administration (SSA) in 2011 provides evidence about effects on health care utilization and estimates the fiscal costs once uninsured DI beneficiaries are provided with health-care package during the 2-year waiting period. 10 However, the project does not evaluate the impact of health care access on health outcomes for the uninsured disability beneficiaries during the waiting period probably due to the constraint of the project design such as the narrow time window of the follow-up survey (6 months), which makes it difficult to observe any changes in health outcomes. Although the demonstration project provides evidence on some important aspects of providing accelerated health care access to disability beneficiaries, it faces challenges that are endemic to many policy demonstration projects. As the SSA acknowledges, the AB Demonstration project is not able to estimate any potential-induced entry effects, which would occur if the accelerated health insurance coverage offered to newly awarded DI beneficiaries would make the DI program more attractive and induce more applicants to the DI program. 10 It is also possible that individuals who expect no health insurance coverage during the Medicare waiting period are less likely to apply for DI. 11 Our study utilizes longitudinal panel data that span over nearly 20 years and allow us to observe disabled workers for a longer period of time and more likely to capture changes in their health and economic status.
A lot of research effort has been devoted to examining the impact of Medicare on health outcomes. 12 –17 These studies have primarily focused on the Medicare impact on elderly beneficiaries rather than disabled beneficiaries. In general, they find that Medicare has no discernible effect on health. These studies are helpful for understanding an average effect of Medicare on health outcomes among the elderly patients. In the meantime, they may have masked Medicare effects on certain subgroups of the population, for example, individuals with poor health. In other words, it is possible that Medicare has differential effect on the health distribution. Workers younger than 65 who have severe and long-term health impairments and lose earning capacity may qualify for the Social Security disability benefits through the DI program. They receive Medicare coverage 2 years after their entitlement to DI benefits. They are likely more ill and worse off financially on average compared to the elderly beneficiaries who survive age 65 and are entitled to Medicare then. Although Medicare may not show significantly positive health effects for the elderly beneficiaries for their chronic health conditions, as shown in previous literature, it may help improve the health status or at least prevent the health from deteriorating for the disabled beneficiaries for their severe health problems. There is some evidence that for the severely ill patients, acquiring Medicare coverage has significant and positive effects on self-reported health, with the largest gains in health improvement among the groups that experience the largest gains in insurance coverage. 18 In this article, we focus on a group of individuals with poor health. They qualify for disability benefits and Medicare entitlement through the DI program, which adopts the strictest definition of disability compared to the criteria used in most other disability programs in the nation, as well as compared to the disability definition used in disability programs in other developed countries.
Another relevant strand of literature is that about the DI program. Research effort in the past about the DI program has mainly focused on understanding the effects of the cash benefits offered by the program. Little analysis has been conducted to understanding the effects of the important in-kind benefit, Medicare coverage, provided by the DI program. The fact that Medicare is a federally administered program and its eligibilities are the same for all individuals, limits the extent to which variation in Medicare coverage can be used to identify the effects of Medicare coverage on individuals in the DI program. The Medicare waiting period creates a health insurance gap for some disability beneficiaries, while others have alternative health insurance (mostly Medicaid) in that period. It provides an opportunity for us to exploit variation in health insurance coverage and identify its effects on disabled individuals.
This article is the first to take advantage of the longitudinal Health and Retirement Study (HRS) and estimate health and economic effects of the Medicare waiting period for disabled individuals. A previous study has used the same data source to study the health effects of Medicare enrollment at age 65 on the near-elderly uninsured. 17 In this article, we explore whether and to what extent the Medicare waiting period impacts health and economic status of the DI beneficiaries who are uninsured while waiting for Medicare to become available. In a quasiexperiment research design, using a difference-in-difference (diff-in-diff) estimator, we compare changes in health and economic outcomes pre-/postentering the DI program for the beneficiaries with alternative health insurance and those without during the Medicare waiting period. The adjusted diff-in-diff estimates suggest that the disability beneficiaries who are uninsured during the waiting, compared to those who are insured, are 13.6 percentage point more likely to report poor health, 6.3 percentage point less likely to be in excellent health, declare more difficulties in activities of daily living (ADL), and about 30% higher medical expenditures from out of pocket. The findings suggest punitive health and economic effects of the Medicare waiting period for the uninsured disability beneficiaries.
The structure of this article is as follows: The first section introduces the research question. Data and the research strategy are explained in the second section. Estimation results are presented in the third section. The last section concludes.
Data and Research Design
Data
The study uses 10 available waves of the HRS, which cover the 1992 to 2010 period, with some interviews conducted in 2011. The HRS is a biennial national representative survey and it interviews individuals born between 1931 and 1941 and their spouses, as well as additional cohorts that have been added in recent waves of the study. The data provide extensive information on health status, employment history, wealth, income, family structure, and government program participation and transfers for a total of 30 672 respondents.
For our analysis, it is crucial to accurately line up the dates pre-/post-DI program for disability beneficiaries and identify the Medicare waiting period. Disability dates are quite complex. One is entitled to DI benefits 5 months after he becomes technically disabled according to the Social Security definition of disability assuming he has become DI insured by accumulating enough work credits. He is entitled to Medicare coverage 24 months after his entitlement to DI benefits. To identify the Medicare waiting period, we must determine the date 1 is entitled to DI benefits, which could be before the receipt of the first DI paycheck. In other words, some beneficiaries become entitled to DI benefits retroactively. This is because it can sometimes take many months or even years before a DI application is approved. The processing times are even longer for claims that are initially denied and then subsequently allowed during the appeal process. Also, those who are eventually allowed benefits might not file a disability claim immediately following the disability onset. Hence, by the time DI beneficiaries are notified that their claim has been allowed, some have completed all or part of the Medicare waiting period. 19 Linking the HRS files to the Social Security Master Beneficiary Record File, we are able to identify the official date of disability onset. The Master Beneficiary Record match rate is about 85%. The linkage of HRS and Master Beneficiary Files is restricted and available from the University Michigan HRS for researchers who meet the criteria for access to confidential data. Knowing the date of disability onset, we can count 5 months from that date to determine the date for DI entitlement, which is when the Medicare waiting period starts. The waiting period ends 29 months after the date of disability onset.
In the HRS, respondents are observed at points in time that are approximately 2 years apart. That is, a 2-year passing is between the adjacent interview waves in the HRS. Comparing the interview dates with the DI entitlement date, we designate the wave right prior to the DI entitlement the pre-DI period and the wave right after the DI entitlement the post-DI period. We exclude in the sample the respondents for whom we do not observe their pre-DI period and those for whom we do not observe the post-DI period. So we include in the sample the individuals who are awarded DI benefits, for whom we can observe both the wave before and the wave after their DI entry (waves identified based on the interview date and the DI entitlement date if available), and for whom we can determine whether they have public health insurance coverage in the wave after DI entry. After applying all the sample restrictions, we are left with a sample of 465 respondents. In the 2-period model aka equation (1), each respondent is observed twice in the wave before entering DI and the wave after. In our analysis, we also expand the specification beyond the 2-period pre-/postcomparison to allow multiple pre- and postperiods aka equation (2), given the fact that the health effects may not become apparent in a narrow time frame. In the multiperiod model, each respondent contribute up to 4 observations in the waves pre-DI entry and up to 4 observations in the waves post-DI entry. The multiperiod sample consists of 2206 observations contributed by 465 respondents.
Our goal is to identify the effects of being uninsured during the Medicare waiting period for the newly entitled disability beneficiaries. We distinguish the following 2 groups in our analysis: the newly entitled DI beneficiaries who do not have any health insurance coverage before Medicare becomes available (23% of the sample) and the newly entitled DI beneficiaries who have access to alternative public health insurance (primarily Medicaid) immediately after entering the DI program (77% of the sample). The former group includes the individuals who lose their health insurance after entering the DI program (14%) and the individuals who already lose health insurance prior to the DI entry (9%). Among the latter, the majority lose the coverage when they leave jobs the wave before. When we drop this latter group from our study sample, the diff-in-diff estimates became slightly larger in magnitude and stayed statistically significant. The DI beneficiaries with health insurance in the waiting period include the individuals who gain access to public health insurance once entering the DI program (57%) and the individuals who get their public health insurance from before entering the DI program (19%). As we will show later, the 2 groups appear comparable in a large array of socioeconomic characteristics and health variables at the baseline period. The DI beneficiaries who have low income and assets may concurrently receive Supplemental Security Income (SSI) benefits. 14%-16% of DI beneficiaries also participate in the SSI program. 23 Most of the DI-SSI concurrent beneficiaries gain immediate access to Medicaid coverage because of their entitlement to SSI benefits. The 2 public disability transfer programs are administered by the SSA and follow the same criteria for determining disability severity. Hence, the beneficiaries under the 2 programs are comparable at the baseline in terms of their disability/health status, a key variable in our analysis.
Table 1 presents preperiod descriptive statistics for the sample of newly entitled DI beneficiaries without health insurance coverage and those with alternative public health insurance upon entering the DI program. All statistics are measured as of the wave prior to the DI entitlement. The 2 groups look similar in general although differences still exist. The mean ages are nearly identical (57.0 vs 56.9). The disability beneficiaries with alternative public health insurance during Medicare waiting period include more women, fewer blacks, and more married. They appear a bit less healthy than those beneficiaries with health insurance in the waiting period. The former report more health conditions and more difficulties in ADLs and instrumental activities of daily living. They are more likely to declare fair or poor health. They utilize more health-care services. The major differences between the 2 groups lie in some of the financial variables. The disability beneficiaries with insurance in the waiting period, compared to those without insurance in the waiting period, on average earns 40% less from work before entering the DI program. However, the former receives nonlabor income (most likely government transfers) that is 4.5 times the amount received by the latter. These differentials are not surprising as the uninsured beneficiaries consist of disabled individuals who receive DI benefits only (rather than DI-SSI concurrently) and who are most likely workers with longer worker histories and higher labor earnings compared to the insured disabled individuals who are concurrently receiving the SSI benefits that are means tested.
Sample Means/Proportions as of the Wave Prior to DI Entry for the DI Beneficiaries With and Without Health Insurance in the Waiting Period.a

Abbreviations: ADL, activities of daily living; BMI, body mass index; DI, Disability Insurance; IADL, instrumental activities of daily living; prev, previous; unemp ins and workers’ comp, unemployment insurance and workers’ compensation.
aNet worth is the sum of assets (primary residence, other real estate, vehicles, businesses, IRAs, stocks, bonds, checking accounts, CDs, and other assets) less liabilities (mortgages, other home loans, and other debt). Major health conditions include (1) high blood pressure or hypertension; (2) diabetes or high blood sugar; (3) cancer or a malignant tumor or any kind except skin cancer; (4) chronic lung disease except asthma such as chronic bronchitis or emphysema; (5) heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems; (6) stroke or transient ischemic attack; (7) emotional, nervous, or psychiatric problems; and (8) arthritis or rheumatism. All dollar amounts are in the dollar of 2009.
What is worth noting is that half of the disability beneficiaries have an annual household total income of less than US$30 000. It suggests that many beneficiaries could benefit from the recently passed health-care reform, the Affordable Care Act (ACA), which makes health insurance more affordable by providing subsidies for families with income below 400% of the federal poverty line to purchase insurance through new health insurance exchanges. We will discuss this aspect further in the last section of this article.
Quasiexperimental Design
The underlying theoretical framework for our research design is a health production function in the 1972 Grossman model. 20 The model views health as a durable capital stock. Individuals inherit an initial amount of this stock that depreciates with age and can be increased by investment. Changes in health stock over time are determined by increased health stock less health depreciation. Health stock is produced by health inputs such as medical care, health knowledge, lifestyle, environment, and so on. So in our reduced-form estimation about health changes over time (pre-/post-DI), we control for changes in medical care (health insurance coverage and health-care utilization), changes in health knowledge (proxied by years of schooling, an efficiency parameter in the Grossman health production function), changes in wealth and income, and other socioeconomic variables as proxy for other factors that may affect health outcomes and hard to measure empirically such as lifestyle.
In a quasiexperiment research design, we use a diff-in-diff estimator, where the first difference is between outcome variables before and after entering the DI program and the second difference is between the disability beneficiaries with health insurance and those without health insurance in the waiting period. Taking advantage of the panel data, we take the within-person change in outcome variables before and after entering the DI program. This is desirable as it guarantees comparability of the groups in the pre- and postperiods, controlling for any compositional changes due to attrition or sampling variation.
One identifying assumption in diff-in-diff models is that other unobserved time-varying processes would have similarly impacted the 2 comparison groups. The preperiod differences in some measures between the groups in Table 1 suggest a potential vulnerability on this front. 21 We address this by testing for differential changes in a number of potential confounders, including health measures, financial variables, and health service utilization. We then present in addition to unadjusted diff-in-diff estimates, the estimates that account for within-person changes in these and other relevant variables.
Let ΔYijt
denote the change in health and economic outcomes for individual i in group j = 1, 0 (DI beneficiaries with and without insurance in the waiting period) between time t and t − 2 (2 years between waves in HRS). ΔXijt
is the change in individual characteristics between time t and t − 2. Dj
is an indicator for being a DI beneficiary with insurance in the waiting period. 
In this 2-period pre–post model, the coefficient β is the diff-in-diff estimate of the effect of being insured during the Medicare waiting and α captures a linear time trend in Yijt
. We also expand the specification beyond the simple 2-period pre-/postcomparison to allow multiple pre- and postperiods, given the fact that the health effects may not become apparent in a narrow time frame. Taking into account the fact that the shape of the time profile could be different for the DI beneficiaries with and without insurance in the waiting period, we interact a flexible function of t with the group indicator Dj
in order to allow the slopes of the time profile to differ before and after DI entry and across groups.
We model f(t) as a sequence of dummy variables for each period t. If we set the reference period to the first postperiod, then the coefficient β continues to be the diff-in-diff estimate.
An attraction of the first-differenced model shown in equations (1) and (2) is that permanent unobservable differences between the 2 comparison groups are differenced out. This is desirable in light of some preexisting differences between the 2 groups shown in Table 1. However, the existence of some preperiod differences also suggests that time-varying processes may differentially impact the 2 groups. For example, health shocks might differentially impact the insured DI recipients in the waiting period given their poorer initial health.
One way of testing for the presence of confounders is to estimate models like those in equations (1) and (2) for each potential confounder. This is similar in spirit to the test offered in a previous study in the context of regression discontinuity designs. 22 Table 3 shows diff-in-diff estimates based on equation (1) for 25 potential confounders, including financial variables, health measures, and health-care utilization measures. The estimation sample has 1 first-differenced observation per respondent. Statistically significant estimates are evidence that the insured DI beneficiaries experienced differential pre-/post-DI changes in a given variable. There is little evidence of differential impacts for pre-/post-DI changes in most of the variables tested, with the exception of a couple of financial variables such as capital income and income from unemployment insurance and workers’ compensation (both statistically significant at 10% level). To control for these important time-varying processes, we include these variables in first differences in the vector ΔXijt in equations (1) and (2).
Results
In Table 2, We first present unadjusted diff-in-diff estimates of β on several health outcome measures (self-reported poor health, self-reported excellent health, and summary of functional limitations in ADL) and out-of-pocket medical expenditures, and then in Table 4 we turn to diff-in-diff estimates adjusted by a large array of socioeconomic variables.
Unadjusted Estimates of Health and Economic Outcomes Before and After Entering the DI Program for the DI Beneficiaries With and Without Health Insurance in the Waiting Period.a

Abbreviations: ADL, activities of daily living; DI, Disability Insurance.
aColumn 3 is column 2 minus column 1. Column 4 is mean within-individual after-minus-before change in the outcome variable. Standard errors are in parentheses.
The new disability beneficiaries with access to public health insurance are 2.5 percentage points less likely to report poor health, compared to before entering DI, while we observe an increase of 12.1 percentage points in poor health reporting from the new disability recipients who are uninsured. The unadjusted diff-in-diff estimate of β, that is, the effect of being insured in the waiting period, on this health measure is −0.145, indicating a 14.5 percentage point drop in reporting poor health after entering the DI program among those with alternative public health insurance relative to those without. This unconditional effect is statistically significant and the calculations using across group changes and using within-person changes provide similar results (Table 2, panel 1).
The rate of reporting excellent health dropped right after the DI entry for both the DI beneficiaries with and without health insurance in the waiting period. The proportion reporting excellent health decreased by about half (from 3.6% to 1.7%) for the new DI awardees with access to public health insurance, while that proportion declined much more dramatically from 8.3% to less than 1% for the uninsured disability beneficiaries during the Medicare waiting period. The unadjusted diff-in-diff estimate of the effect of having health insurance in the waiting period on this health measure is 0.055 and statistically significant, indicating a 5.5 percentage point larger drop in reporting excellent health after entering the DI program among those without alternative public health insurance relative to those with insurance (Table 2, panel 2).
Respondents in the HRS were asked whether they have any difficulty with ADL, such as dressing, bathing, walking across a room, eating, getting in and out of bed, and using the toilet. The total number of ADLs where respondents report any difficulty was close to 1 on average for those insured DI beneficiaries before entering DI and dropped 8% after entering DI. In contrast, the DI beneficiaries who are uninsured in the waiting period reported a remarkable increase of about 90% more difficulties in ADLs when they are uninsured and waiting for the entitlement to Medicare. The diff-in-diff estimate on this health measure (−0.456) indicates a statistically significant (unadjusted) effect on reducing functional limitations of having alternative health insurance during Medicare waiting period (Table 2, panel 3).
The above diff-in-diff estimates on health outcomes indicate that the health status improves or at least does not deteriorate as much for the insured DI beneficiaries in the wave post-DI compared to the pre-DI period. The effect is somewhat surprising: the insured DI beneficiaries consist of mainly SSI recipients who, due to the means-tested nature of the program, are in worse health to begin with (compared to the uninsured DI beneficiaries) because of likely lower investment in health through their life, but they see more improvement (or less deterioration) in their health in the waiting period. This evidence likely suggests the positive effect of having alternative health insurance for DI beneficiaries in the waiting period. As shown earlier in Table 3, except the different health insurance coverage, there is no differential change pre-/post-DI between the 2 groups other than in a few financial variables. The worsening of the few financial variables for the insured beneficiaries post-DI is likely to have negative or at least nonpositive impact on their health. But we observe overall advantageous health changes among them compared to the uninsured DI beneficiaries. The evidence likely underscores the important role played by having access to health insurance in positively affecting health outcomes during the Medicare waiting period. Given the fact that these disabled workers are usually forced to drop out of the labor force due to the onset of severe work limitation, they not only lose labor earnings but also likely lose employer provided health insurance. For these workers who have catastrophic health problems, health insurance coverage would be valuable. The 2-year Medicare waiting period creates additional barrier for the disabled workers who do not have alternative health insurance coverage during the transition period. The evidence we show may suggest negative health effects of discontinuity in health insurance coverage for individuals with serious health impairments. The punitive effect of the lack of health insurance or access to health care would likely be even larger when we account for the disabled beneficiaries who die while waiting for Medicare entitlement. About 2% of the sample dies after entering the DI program and before being entitled to Medicare. This effect needs further investigation when a larger sample for the disabled beneficiaries becomes available.
Tests for Differential Pre-/Postchanges in Potential Confounders for DI Beneficiaries With and Without Health Insurance in the Waiting Period.a
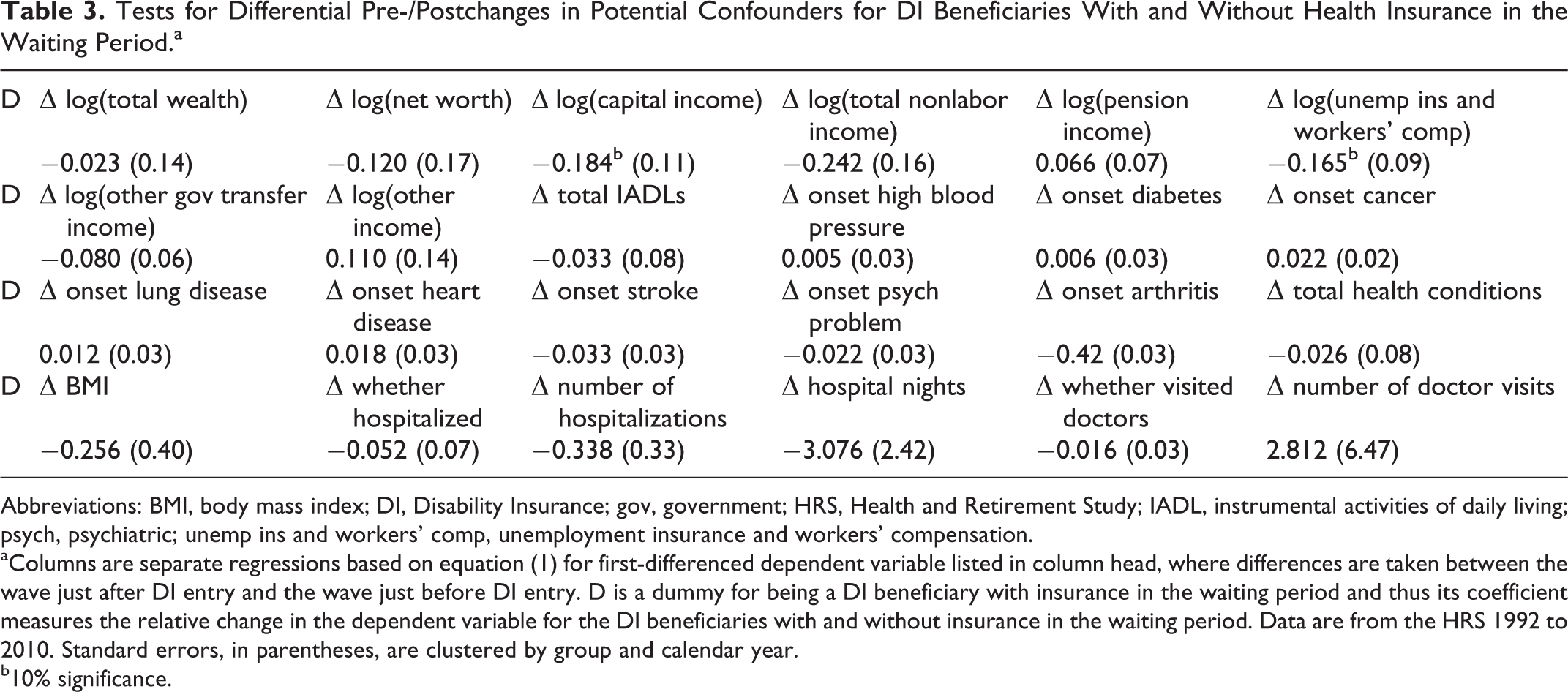
Abbreviations: BMI, body mass index; DI, Disability Insurance; gov, government; HRS, Health and Retirement Study; IADL, instrumental activities of daily living; psych, psychiatric; unemp ins and workers’ comp, unemployment insurance and workers’ compensation.
aColumns are separate regressions based on equation (1) for first-differenced dependent variable listed in column head, where differences are taken between the wave just after DI entry and the wave just before DI entry. D is a dummy for being a DI beneficiary with insurance in the waiting period and thus its coefficient measures the relative change in the dependent variable for the DI beneficiaries with and without insurance in the waiting period. Data are from the HRS 1992 to 2010. Standard errors, in parentheses, are clustered by group and calendar year.
b10% significance.
We also examine the effect on the out-of-pocket medical expenditures of the Medicare waiting period. The medical expenditures in Table 2 (panel 4) are in the form of the natural log. We see an increase of about 16% in the out-of-pocket medical expenses for those who are uninsured while they wait for Medicare to become available, while the DI beneficiaries who have alternative insurance during Medicare waiting period lower their out-of-pocket medical expenditures by about 14%. The diff-in-diff estimate of the insurance effect is −0.30, indicating a 30% decrease in out-of-pocket medical expenditures after entering the DI program for those with alternative public health insurance relative to those without.
In addition, we test the effect of being insured during the Medicare waiting period on some other health outcome measure such as self-reported work limitation and the effect on the employment rate. We find the effects statistically significant and with a sign consistent with the hypothesis. However, these unadjusted effects are either primarily driven by the preexisting difference between the 2 groups (Table A1, panel 1) or mainly attributable to the changes in 1 group (the uninsured DI beneficiaries; Table A1, panel 2).
Table 4 presents several OLS specifications of equation (1), which contrasts pre-/post-DI changes in health and economic outcomes for the DI beneficiaries with and without insurance in the waiting period. The estimation sample has 1 first-differenced observation per respondent. To illustrate the impact of controlling for the potential confounders shown in Table 3, we enter the ΔXijt variables sequentially in groups. Column 1 shows the unadjusted diff-in-diff estimate of β from Table 2 for reference. In column 2, we add first-differenced demographic variables (household size and an indicator for being married). Neither of the additional controls have statistically significant effect on any of the outcomes. In column 3, we add first-differenced financial variables (total wealth, net worth, capital income, total nonlabor income, private pension income, income from unemployment insurance and workers’ compensation, other government transfer income, and other income). The diff-in-diff estimate of β declines slightly in magnitude for the 3 health outcome measures while it goes up a bit in magnitude for the out-of-pocket medical expenditures. Among the financial control variables, statistically significant are only the effect of the total wealth on health reporting and the effect of the government transfer income on the out-of-pocket expenditures, indicating that more wealth is associated with more reports of excellent health and less reports of poor health, and receiving government transfer income here is likely associated with receiving Medicaid coverage and then lowering self-paid medical expenses. In column 4, we add an extensive set of first-differenced health controls that are listed in Tables 1 and 4. Again, the diff-in-diff estimates of β do not change much for all the outcome measures. Among the health control variables, the effects of the onset of cancer, lung disease, heart disease, or high blood pressure on self-reported health status are statistically significant. The onset of high blood pressure or psychiatric problems is shown to have a statistically significant effect on reporting ADLs difficulties. The onset of high blood pressure, cancer, or stroke has a statistically significant effect on the out-of-pocket medical expenditures. In column 5, we use multiple pre- and postperiods as shown in equation (2), and the estimates of β are not very different. In all these first-differenced specifications, we calculate the standard errors allowing for arbitrary correlation in the outcome measures within each of the 2 comparison groups in a given year. For the 2-period models shown in columns 1 to 4, we use calendar years and obtain 20 group-calendar year clusters. In the multiperiod model shown in column 5, we cluster by group and time period relative to DI entry, which gives 16 clusters (=8 periods × 2 groups).
Adjusted Estimates of Health and Economic Outcomes Before and After Entering DI Program for the DI Beneficiaries With and Without Health Insurance in the Waiting Period.a

Abbreviations: ADL, activities of daily living; DI, Disability Insurance.
aColumns 1 to 4 are separate regressions based on equation (1) for first-differenced dependent variable, where differences are taken between the wave just after DI entry and the wave just before DI entry. Column 5 is based on equation (2) for first-differenced dependent variable, where wave-to-wave differences are taken across 4 waves prior to DI entry and 4 waves after DI entry. D is a dummy for being a DI beneficiary with health insurance in the waiting period. Data are from the HRS 1992 to 2010. Demographic variables include household size and an indicator of being married. Wealth variable refers to net worth. Income variables include capital income, total nonlabor income, private pension income, income from unemployment insurance and workers’ compensation, other government transfer income, and other income. Health variables include all health variable listed in Table 1. We include in the estimation an indicator for missing any health information and an indicator for missing any financial information. Standard errors (in parentheses) for 2-period models shown in columns 1 to 4 are clustered by group and calendar year (20 clusters), while standard errors for multiperiod model in column 5 are clustered by group and time period relative to DI entry (16 clusters).
b5% significance.
c1% significance.
d10% significance.
Conclusion
The DI beneficiaries are primarily workers who lose earnings capacity due to severe health limitations. Many lose employer provided health insurance when they are struck by catastrophic health shock and have to leave their jobs. The 2-year waiting period for Medicare access creates a health insurance gap and great hardship for them when they are having both negative health shocks and financial shocks and when they need affordable health insurance package more than ever. Eliminating the Medicare waiting period for disabled workers has been discussed among policy makers and researchers. Existing studies on the issue have mainly focused on the fiscal impact of the policy. This study is the first to use a longitudinal panel data set, examine a rich set of controls, and analyze the health and economic consequences of the waiting period for uninsured disability beneficiaries.
We take advantage of the longitudinal HRS, which covers the period 1992 to 2010 and provides rich information on health status, employment history, wealth, income, family structure, and government program participation and transfers. Linking the HRS files with the Social Security Master Beneficiary Record File, we are able to accurately line up the timing of pre-/post-DI entitlement, which is crucial for our study. In the quasiexperimental research design, we use a diff-in-diff estimator, where the first difference is between the health and economic outcome variables before and after a respondent is entitled to DI benefits, and the second difference is between the newly entitled DI beneficiaries with access to alternative public health insurance and those being uninsured while waiting for Medicare. The adjusted diff-in-diff estimates imply a 13.6 percentage point drop in the proportion reporting poor health, a 6.3 percentage point rise in the proportion reporting excellent health, a drop of total ADL limitations, and a 30.5% decline in out-of-pocket medical expenditures among the DI beneficiaries with health insurance access relative to those without while waiting for the Medicare entitlement. The findings highlight adverse health and economic effects of the lack of health insurance in the Medicare waiting period for the uninsured disability beneficiaries.
The study has its limitations and we should take caution when we interpret the results. First, in this study, we hope to estimate the effects of having immediate Medicare coverage for the newly awarded DI beneficiaries without the 2-year waiting period, that is, the counterfactual effects for DI beneficiaries if we eliminate the waiting period. To that end, we examine a group of newly awarded DI beneficiaries who have alternative public health insurance (mainly Medicaid) in the waiting period and study the changes in their health and economic outcomes. One assumption for applying this research design is that Medicaid and Medicare are similar coverage, for example, with similar health care services and similar financing arrangements for individuals. But if Medicaid has different effects than Medicare for DI beneficiaries, our estimation using Medicaid insured beneficiaries as a counterfactual would likely produce biased results for the Medicare effects on DI beneficiaries.
Second, the 2 comparison groups, the DI beneficiaries with and without health insurance in the Medicare waiting period, are similar on demographic variables but do not look quite the same in terms of health status at the baseline (the wave prior to DI entry). The insured DI beneficiaries appear sicker than the uninsured beneficiaries just before entering the DI program. To make the 2 groups more comparable at the baseline, we could possibly apply propensity score matching procedures. This, however, would be difficult to implement, given the small sample size in the study. With the differences between the 2 groups at the baseline, there may be alternative interpretations of the results. For example, the health of the insured DI beneficiaries does not deteriorate as much or even improve compared to the uninsured DI beneficiaries because the former group’s initial poorer health may reflect transitory negative shocks, or because the latter group’s health may be already on an accelerating downhill trajectory. But these hypotheses are hard to test empirically.
Third, the 2-year spacing between the HRS waves is not ideal although the HRS is the best available data set for this research. With the 2-year gap between interview waves, it is possible that some of the post-DI observations will have become entitled to Medicare coverage, even among the designated “uninsured” group. However, this data limitation unlikely undermines our results and even possibly strengthens our findings. If the “uninsured” group was clear of those observations who were actually insured with Medicare, the differential effects in the health and economic outcomes between the insured and uninsured DI beneficiaries would have been even larger than what we estimated.
The recently passed ACA does not directly address the Medicare 2-year waiting period associated with the DI program. The act does make some changes to help relieve the problems of this health insurance gap. For example, many DI beneficiaries can now join a “high-risk insurance pool” that were created under the ACA and receive immediate insurance coverage while they continue to wait for Medicare benefits to become available. In addition, starting in 2014 disabled individuals in this waiting period will have access to expanded insurance options through state-based insurance exchanges and expanded Medicaid eligibility. Although these new options would not completely solve the problems associated with the Medicare waiting period, based on the evidence provided in this article, these policy changes will likely provide at least temporary relief for many affected individuals with disabilities. Of course long-term effects of these policy changes in the ACA for disability beneficiaries will take time to observe. For example, it is possible that expanded insurance coverage possibilities for disability beneficiaries makes the Medicare waiting period less of a deterrence and make DI more attractive and thus induced more applications to the DI program. On the other hand, more accessible health insurance options in general under the ACA will possibly make the DI program less appealing to some disabled individuals for whom the main driver to apply to DI under the status quo is to get Medicare coverage. To understand the impact of the ACA reforms on the DI program, these are interesting and important aspects to study, especially as the relevant data become available with time passing.
Footnotes
Appendix A
Unadjusted Estimates of Health and Employment Outcomes Before and After Entering DI Program for the DI Beneficiaries With and Without Health Insurance in the Waiting Period.

| Wave Before Entering DI | Wave After Entering DI | Across Group Change | Within-Person Change | |
|---|---|---|---|---|
| Rate of reporting work limitation | ||||
| Insured DI beneficiaries in waiting | 0.728 | 0.970 | 0.242 | 0.255 |
| Uninsured DI beneficiaries in waiting | 0.519 | 0.980 | 0.461 | 0.495 |
| Diff-in-diff estimate of insurance effect | −0.219 (0.05) | −0.240 (0.05) | ||
| Rate of employment | ||||
| Insured DI beneficiaries in waiting | 0.279 | 0.028 | −0.251 | −0.251 |
| Uninsured DI beneficiaries in waiting | 0.509 | 0.037 | −0.472 | −0.467 |
| Diff-in-diff estimate of insurance effect | 0.221 (0.05) | 0.217 (0.05) | ||
Abbreviations: DI, Disability Insurance.
Note: Column 3 is Column 2 minus Column 1. Column 4 is mean within-individual after-minus-before change in the outcome variable. Standard errors are in parentheses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.