
Abstract
The COVID-19 pandemic revealed what educators, policymakers, and researchers have long known—namely, that learning opportunities and outcomes are intimately intertwined with other aspects of children’s and families’ lives. The list of social forces outside the education sector that can affect learning is endless and includes economic experiences that are inequitably distributed, such as housing security (Gallagher et al., 2020), income (Hoynes & Rothstein, 2019), and wealth (Pfeffer, 2018), as well as social experiences, such as interpersonal and structural racism, (dis)ability, and xenophobia (Anderson-Nathe, 2020; DeMatthews, 2020). Now, it is time to lock in this learning among policymakers, practitioners, and researchers. We posit that the concept of “social determinants of learning” can serve as a powerful reframing tool for promoting educational equity, similar to the conceptual shift and policy impact we have seen in public health as “social determinants of health” has become an accepted and eventually essential concept.
Keywords
Social Determinants of Health: Definition and Impacts on Research, Policy, and Practice
Social determinants of health (SDOH) are social and structural factors outside the human body, often beyond the health sector’s traditional reach, that can affect health (Berkman et al., 2014; Honjo, 2004; Yates-Doerr, 2020). SDOH include structural forces, such as racism, misogyny, or classism (separately and/or intersectionally), that in turn have partially shaped systems (e.g., government agencies) and access to resources, such as housing or food (Yates-Doerr, 2020). For example, the U.S. Centers for Disease Control and Prevention (CDC) describes social determinants as including the social and community context, economic stability, neighborhood and built environment, education access and quality, and health care access and quality (CDC, 2021); the World Health Organization (WHO) also highlights social inclusion, nondiscrimination, and structural conflict (WHO, 2022).
SDOH are often of interest because of their implications for health equity. Health equity can be conceptualized as a fair and just opportunity to be healthy and a commitment to social justice in health (Braveman et al., 2011, 2017). Similarly, health inequities can be conceptualized as inequalities in health outcomes that could be prevented but, unjustly, have not been (Marmot & Allen, 2014). Social epidemiology, which formally studies how social factors affect health, emerged in the middle of the 20th century (Krieger, 2001) and has grown substantially in more recent decades (Berkman et al, 2014). The SDOH framework has been a key component of this growth. Although barely 30 articles in PubMed (the primary repository of health-related research in the United States) mentioned SDOH before 2000 and a total of ~540 articles on the topic appeared in the 2000s, references to SDOH have increased exponentially since 2010, growing from 100+ articles per year in the early part of the decade to more than 4,100 articles in 2022 alone.
Reframing health as driven by social determinants that are constructed and perpetuated outside the individual human body has enabled substantial shifts in medical and public health research, policy, and practice. We highlight two important changes that we believe are equally applicable to education: (1) the shift from focusing on individual choices and biological differences as being responsible for health outcomes to a focus on collective behaviors and structural forces as shaping health and (2) an embrace of structural interventions outside the health sector (e.g., environmental, housing, and economic policies) to improve health outcomes.
SDOH make a key theoretical contribution that social conditions are fundamental causes of disease (Link & Phelan, 1995)—that is, they are root causes that will always lead to poorer health outcomes for historically and currently marginalized groups of people, for myriad health outcomes that may also vary over time (Link et al., 2008; Phelan et al., 2004, 2010). For example, although COVID-19 only recently emerged as a disease, who got COVID-19 was socially patterned from the start (Bibbins-Domingo, 2020). Link and Phelan’s fundamental causes of disease theory offers a conceptual understanding of why SDOH persist: Their theory emphasizes the role of structural forces in affecting health outcomes rather than individual-level biological differences or behavioral choices. For example, people from lower socioeconomic positions had a higher risk of contracting COVID-19 for reasons that included their disproportionate representation in lower-wage jobs that required in-person work and for which personal protective equipment was sometimes limited; economic vulnerability that prevented them from leaving jobs that were hazardous to their health; and greater likelihood of living in high-density housing in which it was impossible to isolate from other household members (Avanceña et al., 2021; Wolfe et al., 2021). In addition to socioeconomic inequities in health, racial disparities in health have been widespread and persistent over time. An SDOH framework argues that this inequity is due to exposure to racism—which can be changed (Bailey et al., 2017)—rather than any allegedly “racial” biological differences (Krieger, 2011). This framework thus reveals that people need not be doomed to continue to experience socially patterned health inequities over generations; interventions can mitigate the current social patterning of health (Syme, 2008).
More recent development in public health work to address SDOH has involved studying and implementing interventions beyond the health sector that could address SDOH. Examples include studies of the impacts of the earned income tax credit on child health and well-being (Hamad & Rehkopf, 2016), arguments for education programs and policies to be considered as public health interventions (Cohen & Syme, 2013), health interventions in the form of providing housing (Taylor et al., 2016), and criminal legal system reform (Duarte et al., 2020). During the COVID-19 pandemic, community-based organizations that were focused beyond the health sector, such as affordable housing and immigrant rights organizations, increasingly conceptualized their work as addressing SDOH (Cohen et al., 2022). For example, eviction moratoria have been used as a strategy to promote public health by ensuring that more people—particularly, people from lower socioeconomic positions who were otherwise at risk for eviction due to job loss during the pandemic or other economic constraints—were able to protect their health (Sandoval-Olascoaga et al., 2021). In another example, safe and supportive schools and increased access to education have been identified as strategies for improving adolescent health (Viner et al., 2012).
Social Determinants of Learning: Definition and Proposed Impacts on Research, Policy, and Practice
Building on these insights from the health sector, we believe that consistent terminology and conceptual framing around the social determinants of learning (SDOL) could prove to be powerful tools for educators, policymakers, and researchers who care about improving learning and achieving learning equity. We define SDOL as “social and structural factors outside the individual learner, often beyond the traditional reach of teachers and schools, that can affect learning.” This definition fleshes out what is implied but not explicitly stated in Levinson et al. (2021); it also aligns with the two other extant articles on SDOL (Felter et al., 2021; Sanderson et al., 2021) while providing a conceptualization that goes beyond those two articles’ application of the concept only to higher education in health professions. As with health, SDOL can range from structural forces, such as racism, misogyny, or classism, to downstream effects, including access to resources, such as housing or food (see, e.g., Osher et al., 2020, for an excellent review of the literature). See Figure 1 for a visual depiction of SDOL (with thanks to Ball, 2018, for inspiring the outer cloud).
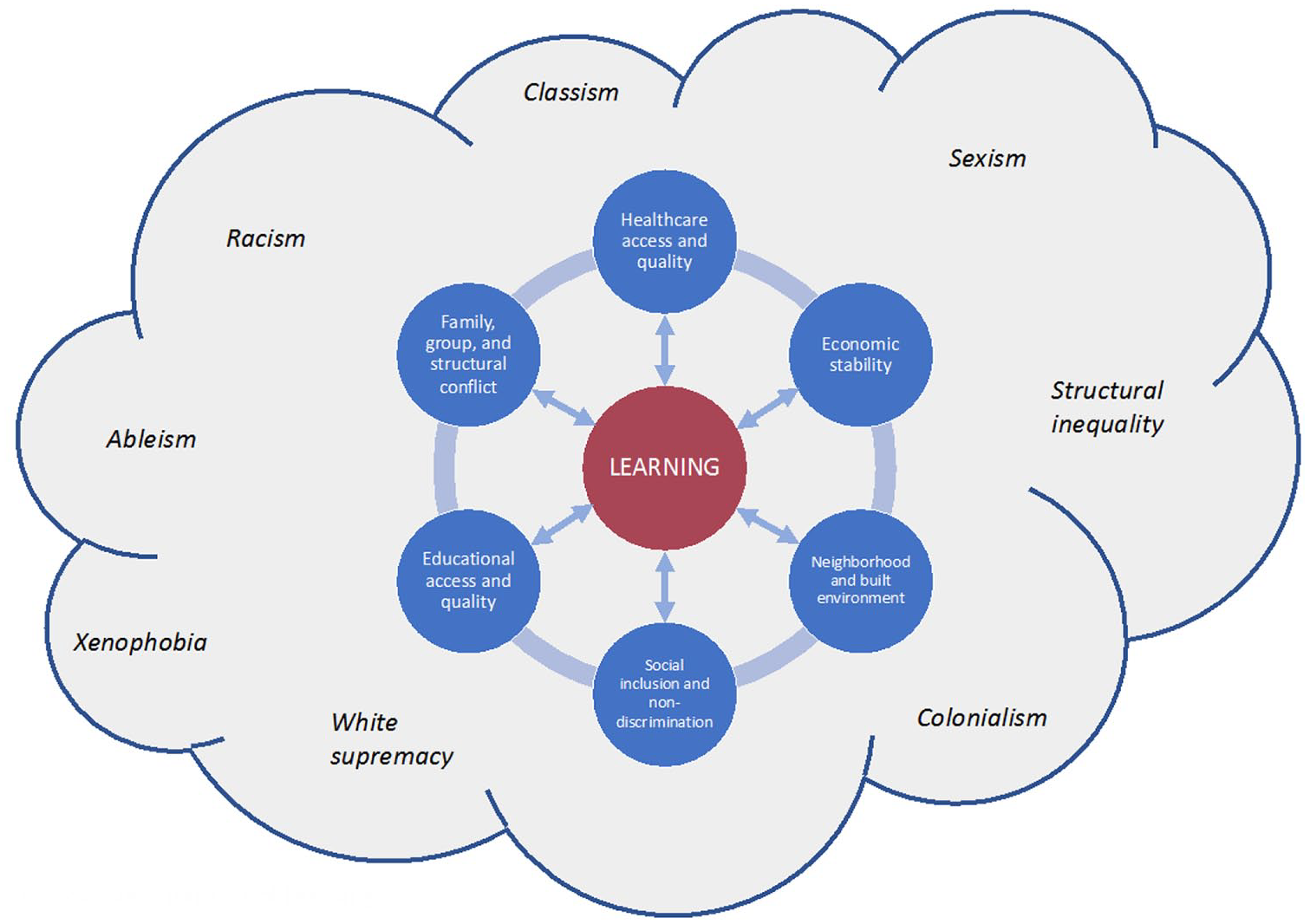
Social determinants of learning.
Aligned with the CDC’s model for SDOH, for instance, is ample evidence that learning is shaped by social and community context (Carter & Merry, 2021), economic stability (Volante et al., 2019), neighborhood and built environment (Chetty et al., 2016; Hyde et al., 2021), educational access and quality (Shi et al., 2022), and health care access and quality (Cohodes et al., 2016). Building on the WHO’s more expansive formulation of SDOH, social inclusion, nondiscrimination, and structural (as well as family and group) conflict are also powerful influences on individual learning (Carter & Merry, 2021). It is also worth noting that relationships between these social forces and learning can be complex and bidirectional—for example, although all of these forces shape learning, learning can also be empowering and can lead to young people taking critical civic action to change these social forces (Ginwright et al., 2006; Gustafson et al., 2021; Kirshner et al., 2021; Levinson, 2012; Logan & Mackey, 2020). This concept is aligned with the inclusion of education in many SDOH lists; just as health inequities influence educational access and attainment, so do educational inequities influence individual and communal health (Cohen & Syme, 2013).
Also, as with health, these SDOL may be present within the “clinical setting” of the school—such as when Black students are subject to more punitive discipline than are White students and hence learn less due to exclusion from classrooms and schools and due to school-based trauma (e.g., Jabbari & Johnson, 2020; LiCalsi et al., 2021; Pearman et al., 2019; Welsh & Little, 2018), or when students from families with lower socioeconomic positions have access to fewer advanced courses and electives than do students from wealthier and higher-income families (GAO, 2018; A. E. Lewis & Diamond, 2015). But, as with health, these social determinants may also affect students’ learning even when they are located entirely outside the school. Students’ differential access to reliable high-speed Internet at home, experiences of food insecurity, and opportunities to develop interests and talents by attending high-quality summer camps, for instance, are all highly correlated with their families’ differential access to financial resources, and all have significant impacts on students’ learning and development (e.g., Haderlein et al., 2021; Kaushal et al., 2011).
Given the already extant massive body of research showing how social and structural practices, relationships, contexts, and systems shape learners’ trajectories, experiences, and outcomes, one may ask why naming these findings as SDOL is likely to make a difference. The “Opportunity to Learn” standards movement in the 1990s and 2000s, for instance, similarly tried to emphasize the importance of taking a contextual perspective on what students need to have equal learning opportunities—although it is notable that Opportunity to Learn scholars and policymakers remained comparatively focused on within-school contexts rather than out-of-school features of learners’ lives (Elmore & Fuhrman, 1995; Moss et al., 2008; National Council of Teachers of English, 2019). Scholars have also tried more recently to make change through emphasizing the impacts of structural inequality (e.g., A. E. Lewis & Diamond, 2015), structural racism (Merolla & Jackson, 2019), and White supremacy (Gillborn, 2005) on learners’ trajectories—also seeing sometimes disappointing results or, even more recently, facing explicit backlash by state and federal policymakers (Stout & Wilburn, 2022). Furthermore, there is the risk that emphasizing the impact of nonschool factors on students’ learning trajectories may lead some educators to disavow responsibility for addressing learning inequities because they are “out of our hands” and/or reinforce racist, classist, or other deficit-oriented beliefs about the inability of some groups to learn (e.g., O. Lewis, 1959; Payne, 2018).
Despite these concerns, we believe that reframing learning as subject to social determinants that are constructed and perpetuated outside the individual learner could motivate two necessary changes in education research, policy, and practice. First, it would shift focus from individual students’ choices and differences as responsible for learning outcomes to collective behaviors and structural forces as shaping learning. In so doing, an SDOL framing may challenge educators and policymakers who persist in locating “failure” in the bodies and minds of individual students instead to recognize that schools are essential spaces for mitigating versus amplifying external sources of risk (see, e.g., Osher et al., 2014). Second, it would reinforce the importance of researching and enacting structural interventions outside the education sector—including interventions in SDOH themselves—to improve learning outcomes. We now describe each in further detail.
First, many (particularly White) education researchers and policymakers have made notable shifts in recent decades in how they discuss racial and socioeconomic differences in learning outcomes, rooting blame less frequently in the bodies of students and their families and more frequently, for better or worse, in the actions of teachers, principals, and district-level policies. (We call out White scholars in particular because Black, Indigenous, and People of Color [BIPOC] researchers and policymakers were less prone to blame BIPOC students and families in the first place [see, e.g., Givens, 2021; Kendi, 2016; Ladson-Billings, 2006; A. E. Lewis & Diamond, 2015; Noguera & Alicea, 2021; Patel, 2014; Tuck & Yang, 2012].) However, there is still a pervasive tendency in education research, policy, and practice to “control for” such factors as race, class, parents’ education, and home language (see C. P. Jones, 2001, for a powerful critique of similar practices in epidemiological research). By reflexively controlling for these factors to essentially erase their effects rather than consistently interrogating the causes of these disparities, researchers and policymakers reinforce the idea that these features are biological and social givens that are outside the scope of intervention rather than treat them as social processes that actively turn difference into disparity (by contrast, see Garcia et al., 2018; Gillborn et al., 2018; and the growing Quantitative Critical Theory, or QuantCrit, scholarship movement). Reframing well-known disparities in terms of SDOL puts the onus on every researcher, policymaker, and educator to recognize disparities in learning as active social constructions that are open to intervention and change rather than as fixed features of the educational landscape.
In this way, the SDOL framing interrupts the false binary between teachers’ presumptive responsibility for school-based impacts on student learning and their presumptive lack of responsibility for impacts that originate outside schools. Rather, SDOL point out that the source of many differences in students’ learning opportunities will be out-of-school factors, such as systemic racism, housing (in)security, fluency in the language of instruction, air and water quality, and so forth—and that classroom teachers, schools, and school systems must therefore proactively be prepared and designed to address and mitigate these differences. These mitigations may include nutritious school meals (Anderson et al., 2018), ventilation improvements (Corsi et al., 2021), full-time staffing with qualified school nurses (Darnell et al., 2019; Yoder, 2020), implementation of culturally relevant curricula (Dee & Penner, 2017), support for students’ ethnoracial identity formation (Miller-Cotto & Byrnes, 2016; Umaña-Taylor, 2023), use of Word Generation to support vocabulary and academic language acquisition (S. M. Jones et al., 2019), and, of course, hundreds of other research-supported initiatives. The point is that the SDOL framing can help counter educators’ sense of impotence in the face of out-of-school impacts on students by reframing racism, classism, sexism, and so forth as active and ongoing processes that they can directly intervene in and redirect or even overcome.
Second, once we name racism, classism, xenophobia, and economic and environmental injustice as SDOL, researchers and policymakers are empowered (and, we believe, required) to seek interventions and study change across the whole range of students’ lived experiences rather than solely intervene upon and study what occurs in schools. Insofar as racism rather than race shapes students’ learning, and because structural and systemic racism manifests in many ways, there may be many potential mechanisms for intervention to improve learning, including reducing racism in students’ access to health care and reducing racial bias in housing access in addition to reducing racism in classroom practices or district policies (Trent et al., 2019). Similarly, school districts and departments of education that are concerned about graduation rates might seek to collaborate with urban designers and housing experts, not only truant officers and school principals, to understand the causes and consequences of student mobility and absenteeism (Brooks-Gunn et al., 1993; Derian, 2016). Chetty et al.’s (2016, 2018) research, for instance, has shown that “every year spent in a better area during childhood increases college attendance rates and earnings in adulthood” (Chetty et al., 2016, p. 856). Additionally, school districts can be part of systems of care to support juvenile reentry from the criminal-legal system; the Second Chance program in Oakland, California, is one such example, although barriers to collaboration remain (Jain et al., 2018; Jain-Aghi et al., 2017).
The COVID-19 pandemic brought the interdependence among social sectors into especially stark light, as the same populations who have suffered the most from health, economic, and environmental inequities have also suffered from the greatest learning inequities, for similar reasons (Goldhaber et al., 2022; Levinson et al., 2021). Although all bureaucracies are distinct, public health and education agencies share many commonalities, and so there are clear opportunities for collaboration that could be improved by using similar vocabulary to describe shared goals and values (Cohen & Schuchter, 2013; Ream et al., 2015). For example, the San Francisco Unified School District has partnered with other city agencies—including the Human Services Agency; the Department of Public Health; the Department of Homelessness and Supportive Housing; and the Department of Children, Youth and Their Families; among others—to integrate select data sets to take actions designed to support students holistically.
We hope that as education researchers and policymakers adopt the SDOL construct, therefore, they will recognize the importance of seeking collaborations with experts in public health, design, and housing—fields that have little representation in most education or state departments at the moment, but that have tremendous insights to offer into the inequities that have bedeviled education research, policy, and practice for centuries. Many promising initiatives have been started or received increased attention during the pandemic, including an effort by Mississippi’s superintendent of education to direct funding to increase students’ telehealth and teletherapy access in rural communities (Levinson & Markovits, 2022) and threefold expansion of funding for social supports for homeless children (DeParle, 2022). Educators and municipalities are now also paying belated attention to the importance of “healthy” school buildings in promoting learning, including the significant impact of improved classroom and building ventilation on student attendance, cognitive function, physical health, academic achievement, and standardized test scores (Lancet COVID-19 Commission Task Force on Safe Work, Safe School, & Safe Travel, 2021).
In conclusion, we emphasize the interconnections between SDOH and SDOL as a tool for reframing research and policy intervention. It is no accident that many SDOH are also SDOL. Therefore, we encourage public health and education practitioners and policymakers to work together to identify structural interventions to address some of these shared social determinants, building upon shared values toward a goal of improving learning and health (Cohen & Schuchter, 2013; Levinson et al., 2021) and shared professional values (Ream et al., 2015). In addition to identifying shared interventions that could address SDOH and SDOL, we recommend identifying interventions that focus specifically on addressing SDOL. The SDOL framework can be an important tool to identify and intervene in structural forces that affect educational inequities within schools as well as open up the world of possible interventions beyond the education sector that can further reduce inequities in learning. This enterprise will inevitably be a long-term proposition. Although the language of SDOH and health in all policies is increasingly used in public health departments (Fosse et al., 2018; Guglielmin et al., 2018), there remains unrealized potential for government uptake of interventions that could address SDOH (Carey et al., 2014) and achieve systemic change (Carey & Crammond, 2015). Large-scale and lasting systemic change is never quick or easy, but that gives us all the more reason to start now.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors
MEIRA LEVINSON is the Juliana W. and William Foss Thompson Professor of Education and Society at Harvard Graduate School of Education and Director of the Design Studio for Ethics and Civics Pedagogy at Harvard's Edmond and Lily Safra Center for Ethics; 413 Gutman Library, 6 Appian Way, Cambridge, MA 02138;
ALISON K. COHEN is an assistant professor of epidemiology and biostatistics at the University of California San Francisco, 550 16th Street, San Francisco, CA, 94158;