
Abstract
The medical education system in the United States has gone through a rapid transition to emergency remote teaching as a consequence of the COVID 19 pandemic. For the Engineering Medicine (EnMed) track of the College of Medicine at Texas A&M University, the most challenging aspects are the transition from in-class team-based learning (TBL) to online sessions and virtual facilitation with an interdisciplinary group of faculties. This article outlines the TBL format used in the EnMed curriculum, along with challenges in delivery, student perspective, and strategies for transitioning existing TBL online.
Keywords
The COVID-19 pandemic has affected the education system at all levels. Many institutions have shifted to remote teaching in response to this crisis (Abel, 2020; Bozkurt & Sharma, 2020; Crick et al., 2021; Mohmmed et al., 2020; Rahim, 2020). Such overnight transformation to online learning is known as emergency remote teaching, which uses remote teaching solutions for face-to-face or hybrid courses during crisis circumstances (Hodges et al., 2020). However, a sudden shift to remote teaching does present challenges for the instructors, students, and other stakeholders. For example, institutions need to build adequate infrastructure for implementing digital learning (Dubey & Pandey, 2020; Ferri et al., 2020; Pokhrel & Chhetri, 2021), students need access to technology to participate in remote learning (Adedoyin & Soykan, 2020; Dubey & Pandey, 2020; Ferri et al., 2020; Thomas & Rogers, 2020), and instructors need to prepare to deliver quality remote teaching with minimum resources and limited time (Dubey & Pandey, 2020; Ferri et al., 2020; Whalen, 2020; Yusuf & Jihan, 2020). The main challenges for the instructors are associated with a lack of digital literacy, the knowledge needed to modify the pedagogical strategies for digital teaching, and the ability to facilitate meaningful online discussion and interaction (Cardullo et al., 2021; Ferri et al., 2020; Thomas & Rogers, 2020; Whalen, 2020).
The Engineering Medicine (EnMed) track within Texas A&M University college of Medicine, also has gone through a rapid transition to emergency remote teaching. EnMed, launched in the 2019–2020 academic year, is a 4-year dual-ME/MD program for engineering or computer science undergraduates. As a tripartite partnership between the Texas A&M College of Medicine, College of Engineering, and Houston Methodist Hospital, EnMed aims to train engineering and entrepreneurially focused medical practitioners to design and implement medical technologies. The ultimate learning goals for students are to master the content of subjects (both engineering and medicine), enhance problem-solving skills, and transition beyond critical thinking to creative thinking. Accordingly, team-based learning (TBL) is one of the primary instructional strategies applied to all the preclerkship courses at EnMed. Specifically, this flipped classroom approach ensures students study the subject content individually and then attend structured, engineering-blended clinically relevant TBL activities in the preclerkship courses. During in-class TBL activities, an interdisciplinary faculty team facilitate the students’ problem-solving processes from various perspectives of clinical, engineering, and fundamental science aspects. When transitioning to emergency remote teaching, the EnMed track switched from in-person TBL activities to online learning sessions while still encouraging and ensuring active participation from students and faculty.
This article first outlines the TBL used by EnMed in its curriculum, along with challenges, student perspectives, and strategies for transition to online teaching of TBL. The conclusion section discusses the limitation of our case and reflects on which of the above strategies are worth continuing in a postpandemic context.
Overview of EnMed
While EnMed students earn a dual degree in Doctor of Medicine (MD) and Master of Engineering, the 4-year medical curricular timeline is similar to that of the regular track students. EnMed curriculum is Liaison Committee on Medical Education (LCME) approved with 18 months of preclerkship and 30 months of clerkship. The Master of Engineering degree is additional to this curriculum and completed within the 4-year EnMed medical timeline. This degree focuses on the design and implementation of medical technologies, and is accomplished by a combination of didactic lectures, hands-on workshops, and experiential learning. Didactic lectures blend engineering technologies, medical science, and commercialization to give the students an understanding of the full process of commercialization of medical technology. Hands-on workshops give the student practical knowledge of devices used in medical care. Experiential activities such as TBL activities give the students an opportunity to integrate and apply this knowledge to real-world examples and reinforce their knowledge.
The EnMed Track
The goal of the integration of engineering and medicine in EnMed is to create a new type of problem-solving doctor or “physicianeer” (i.e., physician–engineers) to address health care challenges. To help students achieve this learning goal, an interdisciplinary group of engineering, basic science, and clinician–educators develop strategies to blend engineering concepts into the medical curriculum. Additionally, students, clinicians, and engineers work within this framework of interprofessional education to identify opportunities to improve health care. This blended curriculum is one of the key characteristic features of the EnMed track. Toward this end, the TBL activities are especially useful for this integration of engineering and medicine in the preclerkship courses. For example, the respiratory physiology TBL activities include hands-on use and development of devices such as spirometers, ventilators, and pulse oximeters used to diagnose, and monitor patients with respiratory ailments. In this way, the EnMed TBL facilitates the application of specific skills, deeper learning, and interprofessional education.
Team-Based Learning in Health Care Education
The TBL, a teaching method, developed by Michaelsen, has roots in the social constructivist approach (Hrynchak & Batty, 2012) that emphasizes developing a high level of team collaboration to address significant problems (Michaelsen et al., 2004; Murzi & Carrero, 2014). The highly structured TBL activities provide an active learning environment in which teachers play a facilitator role during the team discussion (River et al., 2016; Swanson et al., 2019; Thompson et al., 2007). In addition, empirical studies have reported that the implementation of the TBL enhances performance on content acquisition (Fatmi et al., 2013; Swanson et al., 2019), problem-solving ability (Choi & Park, 2014; Kim et al., 2016; Oh, 2015), critical thinking skills (Choi & Park, 2014; Espey, 2018; McInerney & Fink, 2003; Oh, 2015), and so forth. These positive effects of the TBL method hold promise for achieving the designated objectives set for EnMed students.
TBL has grown swiftly in health care education over the past few decades, particularly in medical education (Reimschisel et al., 2017). The existing literature on TBL in health care education intensively concentrated on the TBL experience from both instructor and student perspectives (Davidson, 2011; Levine et al., 2007; Okubo et al., 2012; Reimschisel et al., 2017; Searle et al., 2003) and the impact of TBL on student academic performance (Bouw et al., 2015; Carbrey et al., 2015; Farland et al., 2015; Levine et al., 2007; Reimschisel et al., 2017). In general, both instructors and students had a positive attitude toward the TBL experience. Instructors appreciated high learner participation and interaction in TBL compared with the traditional lecture format (Okubo et al., 2012; Searle et al., 2003). Students valued the opportunities that allowed them to work with peers in the team (Davidson, 2011; Levine et al., 2007). The majority of research studies that investigated the impact of TBL on academic performance reported that students taught by the TBL method performed better on class activities, course exams, or standardized tests such as the National Board of Medical Examiners (Bouw et al., 2015; Carbrey et al., 2015; Farland et al., 2015; Levine et al., 2007). However, most of the studies administered TBL only once or twice (Davidson, 2011). It is necessary to conduct longitudinal studies to fully understand the long-term effect of TBL on education (Reimschisel et al., 2017).
Compared with rigorous research on classroom TBL, studies on teaching TBL in the online environment were fairly limited (Goh et al., 2020; Gomez et al., 2010; Palsolé & Awalt, 2008). The main concerns with online TBL were communication and collaboration among students and between instructors and students (Clark et al., 2021; Goh et al., 2020; Mastel-Smith et al., 2015; Roddy et al., 2017). Most of the studies addressed online communication and collaboration issues through technology (Clark et al., 2021; Goh et al., 2020). Either the instructors identify any specific digital tools, or students could self-select technologies (Clark et al., 2021). As online TBL has received growing attention due to the COVID-19, researchers and educators need to share their experiences and best practices on online TBL implementation.
Challenges and Strategies for Teaching Online TBL in EnMed
Prior to the pandemic, students self-studied course materials and participated in the weekly in-class TBL activities facilitated by an interdisciplinary team of faculty. Such a collaborative teaching allowed students to receive multiperspective feedback to solve highly relevant clinical problems (Anderson & Speck, 1998; Carpenter et al., 2007; Colarulli & McDaniel, 1990; Schaefer Fu & Chase, 1991; Winn & Messenbeimer-Young, 1995). However, the complexity of collaborative teaching added a layer of difficulty in not only generating effective TBL content but also facilitating effective online TBL. This section described how in-class TBL was organized in EnMed and what strategies were applied for ensuring a quality online TBL.
In-Class TBL
The EnMed TBL integrated the prior week’s course content and followed a structure proposed by Michaelsen et al. (2004). In general, there were three phases (Figure 1): preparation before class, in-class readiness assurance tests (RAT), and in-class application of focused exercise.
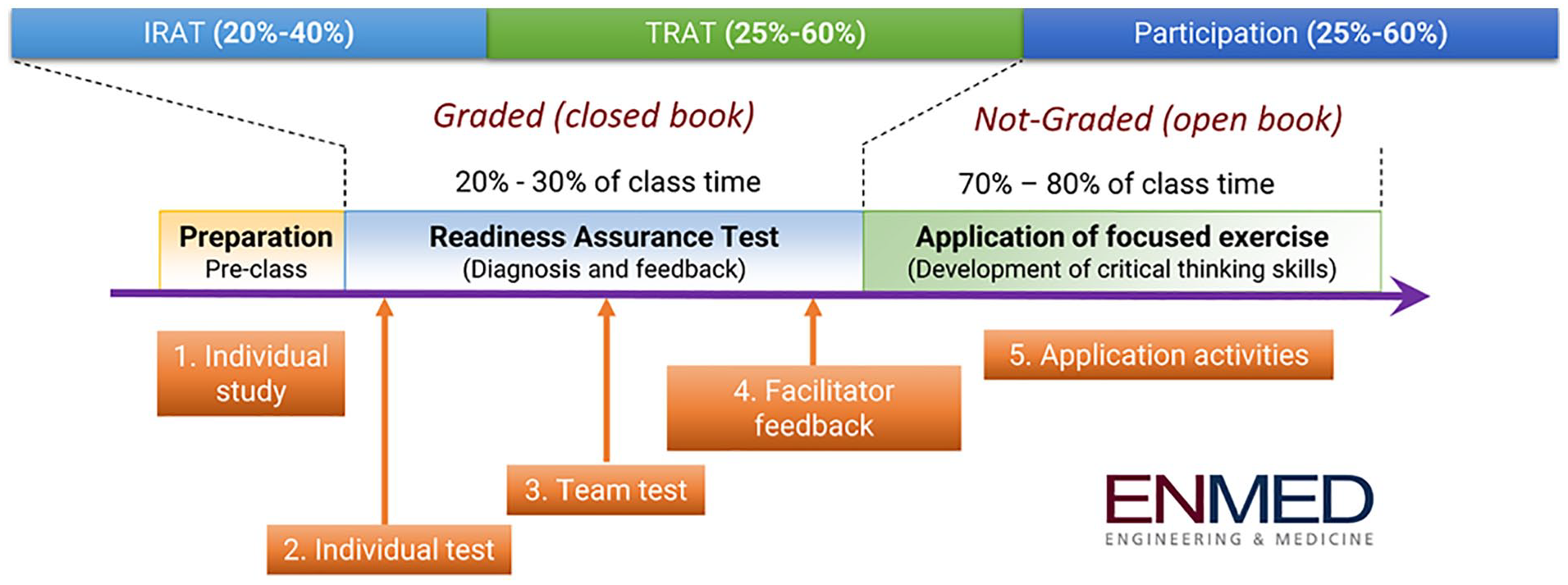
EnMed team-based learning (TBL) process.
Teams were determined by course professors at the beginning of each preclerkship course. Microsoft Excel spreadsheet was used to assign students to teams randomly. The key principle behind teams was to make them as heterogeneous as possible. Therefore, professors conducted spot checks for heterogeneity to avoid assigning students with a similar background to one team. Students stayed in the same team throughout the course. Each team had 4 to 5 students depending on the total number of students in that cohort.
Preparation Before Class
Students reviewed the preparatory materials on their own before the in-class TBL session. The preassigned course materials included faculty-generated notes, recorded lectures, Lecturio videos, and reading assignments as preparation for the medical topics covered that week. Lecturio, an online learning program, provided short online, medical educational video lectures on basic science and organ topics such as anatomy, physiology, histology, cardiology, and microbiology. Each Lecturio video included recall questions at the end of the video that allowed students to check their knowledge. Importantly, these recall questions were presented to the students in a spaced repetition model using an adaptive algorithm with the goal to improve student learning. The preparatory materials and TBL cases were posted on the learning management system eCampus, powered by Blackboard.
In-Class Readiness Assurance Tests
The students’ preparedness was evaluated via a graded, in-class RAT. The RAT was composed of individual and team (iRAT, and tRAT), administered via a web-based application named InteDashboard. Students first completed the iRAT consisting of approximately 10 multiple-choice questions. On completion of iRAT, the students immediately answered the same questions as a team in the tRAT portion and learned content through peer–peer teaching. The tRAT provided immediate feedback with partial credit for subsequent answers provided for any incorrect answer selection. The real-time, automated grading within InteDashboard provided instant feedback on question performance, identifying the difficult concepts in the iRAT, which were subsequently resolved (or not) by the team peer–peer teaching in the tRAT. Learning analytics provided by InteDashboard allowed the facilitators to give feedback on RAT questions where students performed poorly or needed additional clarification. Such an in-class assessment held students accountable for coming to class prepared and working together as a team.
In-Class Application Exercises
Each TBL session consisted of three to five in-class application activities designed to allow students to apply what they have learned to real-life clinical cases. Given that EnMed integrated engineering with medicine, at least one application activity was engineering biodesign- or innovation-related and was related to the medical and engineering content from that week. Each application activity required student teamwork, with the teams arriving at a consensus through discussion and simultaneously reporting their answers for classroom discussion between teams using placards. The facilitators then guided the discussion by asking teams to defend their answer choices, and other teams to corroborate or counteract the choices, thereby facilitating peer–peer teaching. While the main goal was peer–peer student teaching, these application activities allowed the facilitators to address the problem from different disciplines (basic science, clinical, and engineering). As a teaching team presented during a TBL session, a lead discussion facilitator was identified in a mock run-through of the TBL a week prior to the actual TBL date for each RAT and application question.
Transitioning to Online TBL
Despite the unprecedented challenges due to the pandemic, EnMed faculty transitioned the TBL online with countless hours dedicated to this process. Derived through constant communications among faculty and students, the teaching team discovered several strategies that proved effective for delivering TBL online in EnMed.
Preparation was essential for an effective online TBL delivery, particularly for a sudden switch to remote teaching. The key was to create a plan that provided a clear direction on what we needed to do in the transition process. The major areas addressed in the plan included technology requirements, online TBL schedule, and online collaboration in teaching. In EnMed, InteDashboard and Zoom empowered the transition to emergency remote teaching. InteDashboard was already used for EnMed TBL since its inception, and Zoom, a collaborative video conferencing tool, was added as a platform for synchronous online class sessions. The teaching team also outlined detailed online TBL agenda in the planning stage (Table 1). Last in this section for preparation, since there were many different aspects to the online TBL, the faculty were assigned roles for online TBL facilitation: one was to lead class discussion, one was to operate InteDashboard and Zoom, and one was to interact with students in Zoom chat.
A practice run was beneficial for both professors and students to get familiar with online teaching and learning. For the faculty, a practice run could help them get acquainted with the digital tools and the online teaching environment, particularly those who had no prior knowledge of online teaching. In addition, a practice run allowed an evaluation of timing, technology operation, the quality of online collaborative teaching, and adjustment of the delivery plan. In EnMed, the teaching team had a practice session on Zoom before every online TBL, which was particularly helpful for the visiting physicians who were subject to change depending on the TBL topics. For students, a practice run could help mitigate their stress due to a sudden switch to online learning and teach them the skills needed in an online environment. Therefore, the EnMed students participated in a mock session at the beginning of the semester. During the mock session, they identified the technical requirements for online TBL and tested the functionalities of the devices. Moreover, the mock session allowed them to recognize the differences in online TBL, such as the modified process and online interaction patterns.
Adaptive facilitation was critical to improving the quality of online TBL. Research indicated that an effective adaptation of the teaching process promoted students’ learning motivation (Kostolányová et al., 2011). In EnMed, the facilitation process was adapted regularly based on students’ learning needs. During the application activities, the professors visited random groups periodically to observe students’ discussions. When professors observed the problems or difficult concepts, they could be separately discussed in the faculty breakout room, allowing a private space for the faculty to quickly identify a solution and adjust their facilitation strategy accordingly. Such adaptation of the facilitation process motivated students in the online TBL discussions and contributed to a continual improvement in the delivery of online TBL.
Establishing a social presence could help to promote online engagement and virtual collaboration. Social presence, rooted in constructivist learning theory, was essential to facilitate the interactions between the teachers and students, thus facilitating the development of knowledge and skills (Collins et al., 2019). In EnMed, the faculty always had their cameras on and communicated with students in Zoom chat. Students were also encouraged to keep their cameras on to establish a social presence in the virtual learning environment. Zoom chat feature reassembled a learning community for students to post their questions, get supports from peers and professors, and collaborate with peers.
An Example of an Online Team-Based Learning Agenda

Note. iRAT = individual readiness assurance tests; tRAT = team readiness assurance tests.
Some Preliminary Findings on Online TBL From Students’ Perception
To understand how students perceived online TBL transition, we surveyed the student satisfaction of the online TBL. All students from the first cohort received a Qualtrics survey in July to provide their perspective on their online TBL experience. The TBL satisfaction survey (Roh et al., 2014) was a 5-point Likert-type scale that evaluated seven categories: learning process, preassignment, team activity, learning environment, orientation, course content, and peer evaluation. The survey was slightly modified to fit the EnMed TBL experience, which did not have the peer assessment category. In addition, the learning environment factor focused on classroom management, such as seat arrangement and microphone installation, were not evaluated with online TBL.
Of the 25 first-year medical students, 19 completed the survey for a student response rate of 76%. Overall, students were satisfied with their online TBL experience. The overall average of scores on online TBL experience was moderate (M = 3.67, SD = 0.5). Of the five measured factors, the average of scores on learning process (M = 3.74, SD = 0.47) and team activity (M = 3.79, SD = 0.51) factors were a little higher than preassignment (M = 3.53, SD = 0.84), orientation (M = 3.53, SD = 0.66), and course content (M = 3.58, SD = 0.6) factors.
To captured in-depth insights from students on their online TBL experience, some open-ended questions were attached to the end of the survey. According to students’ responses, online TBL were more time-efficient and allowed more effective team discussion compared with in-class TBL. Students mentioned that the online format seemed more efficient in sticking to time. When attending online team discussions, only one student was talking at a time that avoided wasting time in “shout over one another.” Students became more patient in listening to each other, thereby promoting more effective team discussions. In addition, students explained that they were more engaged in team discussions because of fewer distractions in breakout rooms.
Students also shared that interaction was their major concern with online TBL. Students stated that the issues existed in both student–professor interaction and student–student interaction. Although professors visited breakout rooms periodically, online TBL was challenging to give timely feedback when students needed it most. Students recalled that they had to wait for professors to enter their breakout rooms after asking for help. Moreover, students felt it difficult to gauge appropriate times to ask questions to professors during class discussions. Similarly, students were aware that it was harder to discuss team collaboration issues with peers in an online format. Students commented that it was harder to gauge how peers would respond to constructive criticism in an online medium. Besides online interaction, students reported other concerns with the TBL, such as spending too much time on a single concept and develop a better structure in collaborative teaching with a team of professors. Yet, these concerns were not unique for online TBL.
Conclusions
In closing, the quality of TBL is essential in EnMed because it is the primary instructional strategy for all preclerkship courses. Although in-class TBL is optimal for EnMed students, the survey results indicate that online TBL can be as effective in mastering the content of subjects, building problem-solving skills, and developing collaborative skills. The implementation of online TBL on a weekly basis allows EnMed faculty to continually improve the delivery of online TBL. Therefore, the significance of the EnMed case lies in its effort in sharing best practices of implementing online TBL.
There are unavoidable limitations in this article. Although online TBL appears to be effective based on survey results, we need empirical research to confirm that the strategies applied in online TBL positively influence students’ learning performance. Furthermore, the cohort we discussed in this article has 25 students. Some strategies summarized from our practices might not be applicable for those with big class sizes.
Overall, the sudden change to teaching TBL online allows us for a reevaluation of the teaching practices. Some adjustments made to adapt to online TBL seem beneficial for in-class TBL, such as assigning particular roles to instructors and adaptive facilitation. Moreover, in response to the increasing use of technology in the postpandemic, it is crucial to help educators better teach in a technology-based environment. Therefore, we call for more research to investigate the implementation of online TBL using digital technologies, thereby summarizing a set of applicable guidelines for better educational practices.
Footnotes
Authors’ Note
Student satisfaction data collection was approved by Texas A&M Institutional Research Board (IRB number IRB2020-0785M). We acknowledge the support of Open Access Publication Funds by the Department of Medical Physiology in the College of Medicine at Texas A&M University.
Authors
YUN LI is affiliated with the College of Medicine at Texas A&M University. Her research interest is educational technology.
NICHOLAS A. SEARS is affiliated with the EnMed and College of Engineering at Texas A&M University. His research interest is the integration of engineering in medical education.
IAN V. J. MURRAY is affiliated with the EnMed at Texas A&M University. His research interests are physiology and medical education.
KAMLESH K. YADAV is affiliated with the EnMed at Texas A&M University. His research interest is medical education.