
Abstract
Often the first-time health professionals work together is as new graduates, with a paucity of shared learning among the various health disciplines within university curricula. This is largely due to the complexities of delivering interprofessional education (IPE) and the preference of individuals to work within their established silos. With its ability to nurture collaboration among students, there is a developing trend to use team-based learning (TBL) as a teaching method to engage health care students in IPE. Using the conceptual lens of social capital theory, the purpose of this article is to provide readers with an overview and evidence for the use of TBL within the interprofessional health care education setting, highlighting the benefits and challenges.
Keywords
Introduction
Team-based learning (TBL) has been described as “an active learning and small group instructional strategy that provides students with opportunities to apply conceptual knowledge through a sequence of activities that includes individual work, teamwork, and immediate feedback.” 1 Team-based learning offers an effective and resource-efficient pedagogy to teach a large number of students in small groups. With the ability to transform small groups into teams, TBL has the capacity to enhance the quality of student learning by fostering active small and large group discussion, collaborative decision-making, and immediate feedback. 2 Although originally developed in the United States for use in business schools during the 1970s, and first introduced to medicine in 2001, TBL has become popular internationally as a student-centered teaching method across all health care disciplines, with reported use in medicine, pharmacy, nursing, dentistry, allied health, public health, and health sciences.3-5 Within health care education, the key focus of TBL is on clinical problem-solving activities, requiring development of competencies critical for health care workers: teamwork skills and critical thinking.
With its ability to nurture collaboration among students, there is a developing trend to use TBL as a teaching method to engage health care students in interprofessional education (IPE). 6 Defined as occasions “when two or more professions learn with, from and about each other to improve collaboration and the quality of care,” 7 IPE helps to develop the behaviors and attitudes requisite to working in teams with colleagues from different health professions to deliver patient care. Provision of an interprofessional context to university health education activities has the potential to improve students’ leadership, collaboration, and communication skills in preparation for entering the workforce.8-10 Although widely acknowledged that excellence in healthcare and patient safety relies on effective communication between professionals, most university health care education programs provide little shared learning among the various health disciplines (such as medicine, allied health, pharmacy, nursing, and dentistry). 7 Despite the accepted importance of building skills for effective collaboration, it is still often the case that the first-time health professionals work together is as new graduates. This is largely due to the complexities of delivering IPE, including the timetabling and logistical issues associated with the delivery of face-to-face IPE activities.11,12 In addition, there is often a preference for individuals to work within their established silos.13-15
There is a paucity of pedagogical practices that are student-centered, provide active learning with content that is simultaneously relevant to the learning needs of different professions, and are designed for implementation on a large scale. However, interprofessional TBL provides a structured platform to promote opportunities for health care students to learn effectively together. The structured format means that they can be redesigned to suit a range of topics with case scenarios chosen to suit a particular mix of disciplines. 16 Interprofessional TBL provides a new approach to learning and instruction, and therefore, research regarding its effectiveness is only emerging. Theories informing educational practice offer valuable lenses to observe, design, and analyze student learning and teaching. 17 Sociocultural learning theories view learning as a social activity, with social interactions key to learning. 18 In this review, we propose that the interprofessional class-based activities in TBL encourage the building of social capital. 18
Using the conceptual lens of social capital theory, the purpose of this article is to provide readers with an overview and evidence for the use of TBL within the interprofessional health care education setting, highlighting the benefits, challenges, and limitations. Here, we provide a tentative conceptual framework related to interprofessional TBL practice. We first describe TBL in detail and, providing examples of interprofessional TBL, reinterpret these activities in light of social capital theory.
Structure of TBL
While the pedagogy of TBL supports the flipped classroom method, requiring individual preparation, it relies on the cohesive teamwork of students in class. 19 Team-based learning classes typically consist of 40 to 100 students, which are subsequently divided into small teams consisting of 5 to 7 students. 5 These teams are assigned by the facilitator to ensure that a diverse mix of students are assigned to each team. Each student must take responsibility for adequate preparation and engagement in small-group and large-group learning. The facilitator must manage the process of student engagement and feedback, encouraging collaboration, critical reasoning, problem-solving, and reflection. 19 In TBL, a peer review process provides an incentive for students to contribute to group learning and also helps to develop professional competencies. 5 The process usually requires students to contribute to the grades of other students by providing qualitative and quantitative feedback to their team members. Team-based learning involves specific tasks organized into three distinct phases: the “preparatory” phase, the “readiness assurance” phase, and the “application” phase (Figure 1).
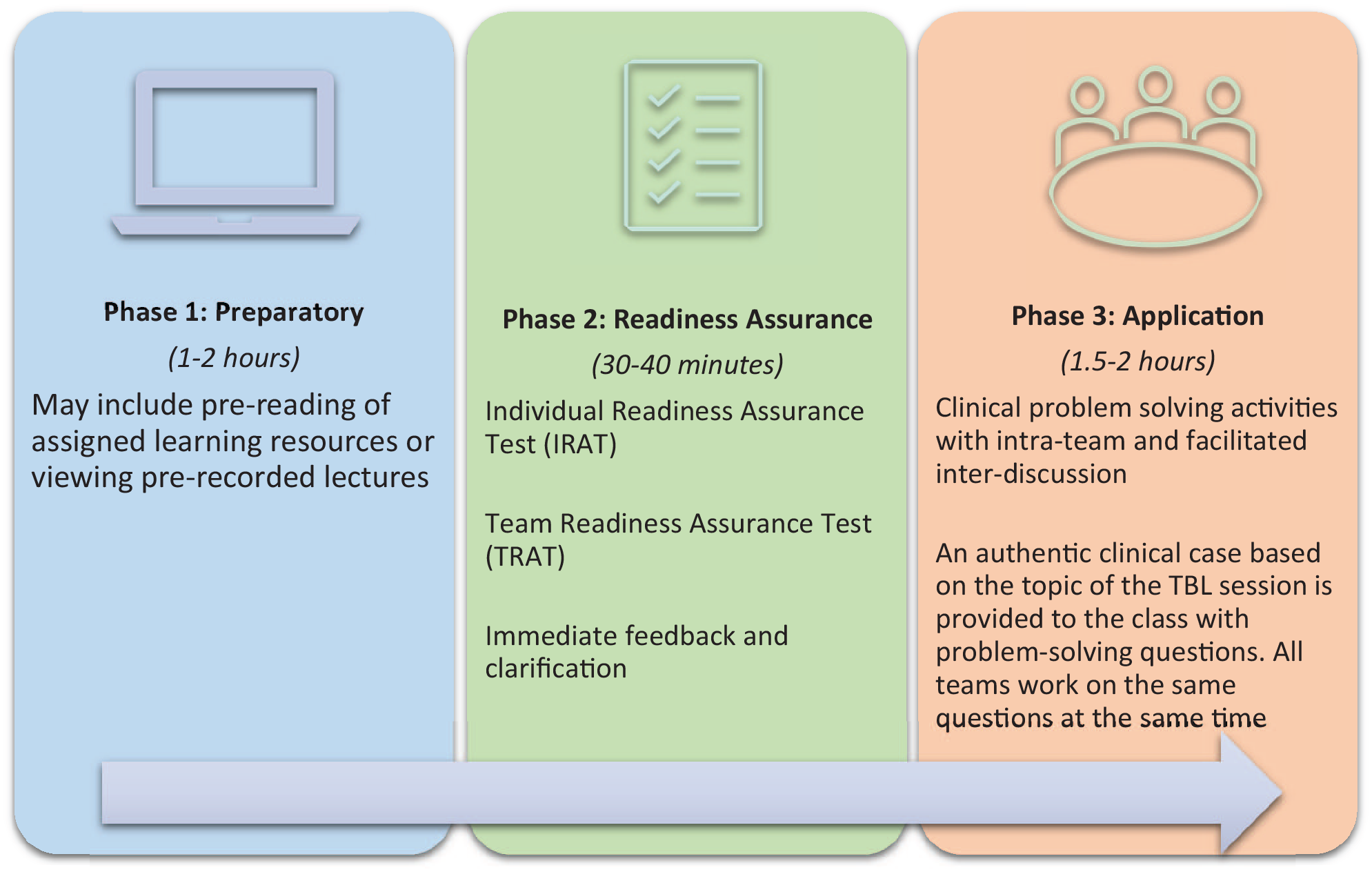
The 3 phases and specific steps of TBL with suggested time frames. TBL indicates team-based learning.
The first phase is the “preparatory” phase, where students are provided with specific material to prepare prior to class. Students are assigned learning resources that align with the in-class topic. The second (“readiness assurance”) and third (“application”) phases of TBL occur in class. During the “readiness assurance” phase, students first complete an individual readiness assurance test (IRAT), consisting of multiple-choice questions. This is followed by a team readiness assurance test (TRAT), where the same questions are taken by the team. Here, students discuss each question before deciding on the best answer. The class then receives immediate scoring for each team. Feedback and clarification are then provided by the TBL facilitator. During the “application” phase, students work in their teams on the clinical problem-solving activities.5,20,21 The clinical problem-solving activities lie at the heart of TBL, 20 where both student learning and team development are promoted. Teams are required to apply their collective knowledge, skills, and values to solve complex, real-life clinical problems. 20 The “Four S principle” of design guides this process, where the clinical problem is “Significant,” all team members work on the “Same” problem, with a “Specific choice” being reported by all teams “Simultaneously.” 20
TBL research
Current evidence suggests that TBL provides an effective means of improving students’ academic performance. 4 A systematic review by Reimschisel et al 4 confirmed previous findings that TBL is most effective in supporting students who are academically poor performers, compared to those who are academically stronger. Although learner reaction to TBL has been mixed, both students and faculty generally prefer TBL to more traditional teaching formats, such as lectures. 4 TBL is generally favored because of increased student engagement created through its active learning style and the peer learning and problem-solving opportunities provided. 4 Internationally, interprofessional TBL studies have reported implementation within a range of discipline mixes and topics.22-26 Yet, despite its increasing popularity, the scope of research on interprofessional TBL is limited. The majority of interprofessional TBL studies provide descriptions of implementation, report on student perception, and provide comparisons of IRAT with TRAT scores.22-27
Social capital within the context of interprofessional TBL
Social capital is described as “a collective asset in the form of shared norms, values, beliefs, trust, networks, social relations, and institutions that facilitate cooperation and collective action for mutual benefit.” 18 First identified by Pierre Bourdieu, the concept was further drawn on and popularized by other sociologists. 28 The conceptual framework of social capital has previously been used to measure and describe the individual gains of network participants within interprofessional activities. 18 It provides a tool to conceptualize and understand the processes involved in a social network. Accordingly, by learning to build social capital within interprofessional activities as students, health care workers will be better prepared to collaborate and invest in real-world interprofessional teams once they enter the workforce. Within the context of interprofessional TBL, social capital provides a means to view and analyze the processes involved and the outcomes of a social network. 18 There are three key attributes of the social capital network: (1) Trust, (2) Resources, and (3) Norms and Rules. These attributes can be considered within the context of interprofessional TBL (Figure 2).
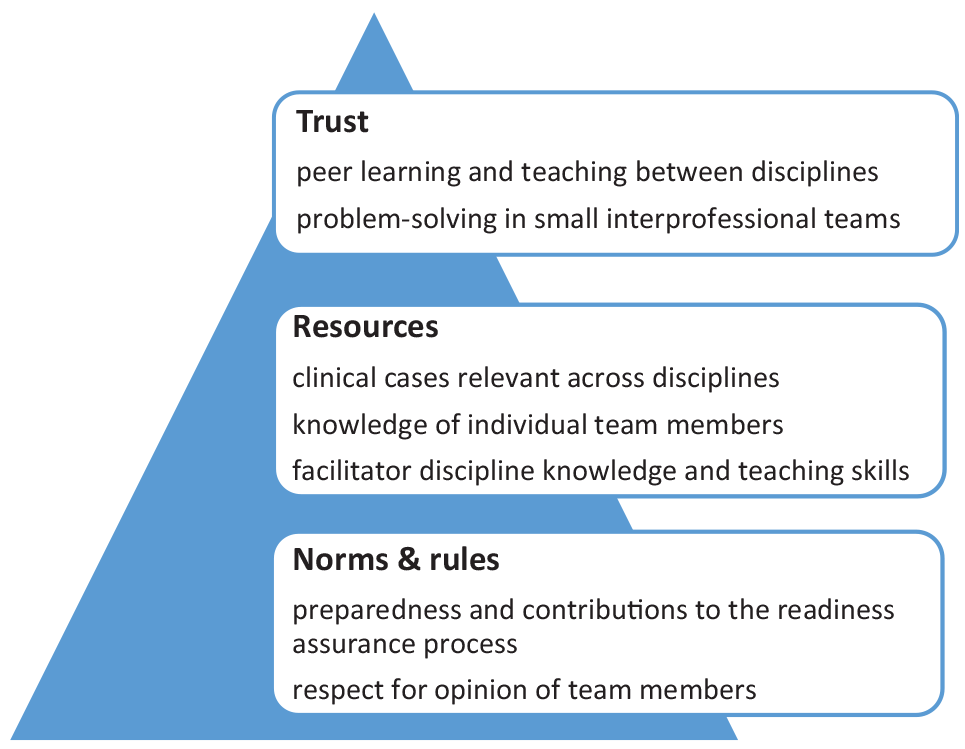
Examples of the “Trust,” “Resources,” and “Norms and Rules” within the context of interprofessional TBL. TBL indicates team-based learning.
“Trust” refers to the trust that builds within the social network. 18 A sense of trust is developed when students feel they are being treated as a member of a group with similar aims. In interprofessional TBL, trust is exemplified by the trust that builds between students largely because of their intra-team interactions. Students rely on their peers to attend class prepared for the TRAT and contribute to their clinical problem-solving activities. Having received the same required preparation material, all students are placed on a “level playing field” on attending the face-to-face class. A previous study by Burgess et al 26 presented the outcomes of a single, 2.5 hour interprofessional TBL module on the topic of back pain, involving Year 1 medical students (n = 277) and Year 2 physiotherapy students (n = 89) at the University of Sydney, Australia. Comparison of academic performance on the IRAT, consisting of 10 multiple-choice questions prior to class, showed no difference between the two disciplines, suggesting similar baseline knowledge. In addition, there was no perceived difference between medical students’ and physiotherapy students’ perceptions of their TBL experience.
On attendance at class, there must be a willingness of the network members to engage and assist others in the problem-solving activities. 18 Interprofessional TBL sessions are likely to be infrequent “one offs,”22,24,26 or only occurring across a few sessions,23,25 rather than regularly integrated curricula activities. It has been suggested that a negative bias might result when exposure to TBL is minimal, and hence, the benefits of TBL may not be fully realized. 29 Although at the outset of an interprofessional TBL, individuals are less to have firsthand knowledge of each other, evidence suggests that they appear to trust in the good will and professional knowledge and skills of each other.22-27 A key strength of the TBL pedagogy is the trust that is required to collaborate and complete teamwork activities, including the TRAT and clinical problem-solving tasks. Indeed, most interprofessional TBL studies report that teams outperform the mean score of their individual team member during the readiness assurance process.22,23,25-27 For example, Burgess et al 26 reported that all TRAT scores were higher than any individual’s IRAT score, suggesting that team members discussed their responses in class and collaborated to come to a consensus on each answer. Within the context of an interprofessional TBL, this generalized trust is developed and may be transferable to future interprofessional collaborations with health professionals in the workplace.
“Resources” describe the resources the social network offers to its members, including the knowledge and skills that each individual holds. 22 Relevant resources include both external and internal resources. External resources are accessed through interactions with other network members, and in the context of an interprofessional TBL, external resources include students within the team, the class, and facilitators. Being able to communicate knowledge and skills regarding a patient case, with consideration of the views of others is essential to working in the interprofessional setting. 16 Student teams must be carefully allocated to ensure the shared resource of knowledge from different disciplines. The TBL class provides opportunities for students to work together to problem-solve and “speak up” to discuss and model their thinking process according to their disciplinary knowledge. Wheeler et al 22 described a single, 2-hour, interprofessional TBL on the topic of health professional roles and responsibilities, at the University of Ohio, USA. Participants included early year pharmacy (n = 132) and medical students (n = 195). Students completed an Interprofessional Collaborative Competencies Attainment Survey (ICCAS) before and after the TBL. Results showed significant improvement in IPE competencies, particularly in students’ perceived capacity to “understand the abilities and contributions of the interprofessional team members” and “recognise how others’ skills and knowledge complement and overlap with (their) own,” indicating better preparedness for future collaborative practice in the workplace. 22
Importantly, facilitators bring not only their professional knowledge and skills but also their teaching skills to the TBL. Throughout the TBL session, facilitators are required to provide immediate and accurate feedback to individuals, teams, and the class. When facilitating interprofessional activities, it can be difficult to remove a discipline-based “hat” and consider the perspectives and roles of all health care professions. 16 However, Burgess et al 26 reported that students found it beneficial to be taught by a multidisciplinary team of facilitators (a rheumatologist, physiotherapist, and basic scientist) who each brought their clinical experience, providing continuous feedback and “multidimensional explanations of patient care.” Importantly, facilitators must carefully develop material and resources for interprofessional activities that are relevant to all network participants,30-32 and in TBL, this includes the TBL pre-reading, the readiness assurance test, patient case, and the clinical problem-solving questions. Other important material resources in the interprofessional TBL include the large room facilities—requiring multiple small tables and chairs to ensure intra-team and inter-team interaction.
“Norms and Rules” refer to the implicit values that govern the actions of individuals during the activities of the network. 18 For both students and faculty participating in TBL, the expectations for preparation and engagement are set through the “norms and rules” of each specific step: preparation, IRAT, TRAT, feedback, and problem-solving activities. For example, it is expected that students attend class having completed the preparation requirements and are ready to contribute to the team test (TRAT). Due to the lack of integration of interprofessional TBL into curricula, there is little reporting of a peer review process; however, it is anticipated that the “peer pressure” of small group work encourages participants to complete their assigned pre-reading and contribute to in-class activities. 33 During class, there are expectations around behaviour. For example, it is expected that students listen to the views of their team members when deciding and committing to TRAT answers and when problem-solving. A large-scale interprofession TBL initative, reported by Chan et al, 24 involved participation of 801 students from 6 disciplines (medicine, biomedical sciences, nursing, pharmacy, social work, and Chinese medicine) across 7 programs at two universities in Hong Kong (The University of Hong Kong and The Hong Kong Polytechnic Universty), in a “one off,” 4-hour TBL session. Students were asked to indicate their readiness for IPE using the Readiness for Interprofessional Learning Scale (RIPLS) before and after the TBL. 24 Following participation, students showed significant improvement on the RIPLS in their attitudes toward interprofessional learning and their readiness to engage in interprofessional learning. On the scale, “Communicate opinions to other professionals and listen respectfully to others’ opinions” received the highest attainment, as well as outcomes relating to the need to collaborate with others, compare roles and responsibilities, and recognize the acceptability of views of others. 24
Students participating in interprofessional activities learn to build their own social capital by investing in the group work. Dependent on the context, students need to share the appropriate disciplinary knowledge with each other, and through participation, they are better prepared for collaboration on entry into the workforce. 34 Literature suggests that students with higher collective efficacy find teamwork to be necessary and meaningful. 35 Burgess et al 26 reported that qualitative feedback from students demonstrated an appreciation for the opportunity to learn about another healthcare discipline curriculum and their scope of practice, and gain perspectives on a patient case from a different discipline. Certainly, the quality of social capital is influenced by the quality of the relationships formed by those undertaking the activity, as they learn about, from, and with each other. 34
Challenges of building social capital through interprofessional TBL
Although the concept of social capital is valuable, there are also limitations in the application to interprofessional TBL. For example, it cannot always be assumed that all students are familiar with the steps and requirements of TBL, particularly in the interprofessional context. That is, students will be most familiar with the teaching pedagogies that are predominantly used within their own disciplines. For example, Burgess et al 26 reported that while medical students were well versed in the practice of TBL, physiotherapy students were new to the pedagogy, potentially hindering their engagement and contributions.
Another challenge of interprofessional TBL is ensuring the provision of an evenly distributed interprofessional team of facilitators for each TBL class in large-scale TBL initiatives. Similarly, it can be challenging to evenly distribute students to provide equal representation of disciplines within TBL teams, particularly with large numbers of students. Burgess et al 26 mentioned students’ dissatisfaction with the uneven ratio of medical and physiotherapy students within each team. With less physiotherapy students in each team, physiotherapy students felt they needed to provide greater rationale for their decisions, and medical students felt they needed to be mindfully inclusive. 26 Chan et al 24 noted the difficulty in matching students from across their 7 included programs and 6 disciplines.
Access to adequate resources and differences in personal goals may influence student engagement in learning, and it is how individuals with differing levels of knowledge and skills work together that will ultimately shape the quality of the experience. Lochner et al 25 reported on a 3-day interprofessional TBL on the topic of patient safety and learning from errors, at the Claudiana College of Healthcare Professions, Bolzano/Bozen, Northern Italy. Participants included senior health care students (n = 39) from 5 disciplines (nursing, dietetics and nutrition, occupational therapy, radiology techniques, laboratory techniques). Although the topic of patient safety and learning from errors is relevant to all health professions, they reported that student learning outcomes may have been hindered to some extent by the need for specific clinical cases to be inclusive of all 5 disciplines. 25 In addition, disparities between how IRAT and RAT scores may contribute toward students’ summative assessment for individual disciplines is a potential issue in interprofessional TBL. For example, Chan et al 24 suggested that such differences may have affected participant motivation.
Black et al 23 reported on 3, half-day interprofessional TBL sessions on patient safety, professional ethics, and health systems and disparities, at the University of Florida Health Science Centre, USA. Participants included 639 junior health professional students, across 10 disciplines (audiology, dental, medicine, nursing, occupational therapy, pharmacy, physician assistant, physical therapy, public health, speech pathology). Although students’ perception of teamwork competencies and participation were excellent, there were significant differences reported in IRAT performance by some disciplines across the 10 included in the TBL. 23 Perhaps readiness to participate in the TBL is influenced by where the topic is aligned within the curriculum of each individual discipline. Although the preparation material provided for each TBL session will be the same for all disciplines, it may be that students have learnt topics at different time points within various curricula. As the number of discplines included in a TBL session increases, it becomes increasingly difficult to find consistent alignment. However, TBL offers a structured format to help shape the interprofessional interactions and experience. Notably, the same study (Black et al) reported a positive correlation between students’ perception of teamwork and TRAT performance. 23
As with any class-based interprofessional activities, logistical issues, such as timetabling, also bring challenges. For example, Chan et al 24 reported difficulty using large lecture halls as TBL venues, which was required for such a large-scale interprofessional activity. To promote student engagement in small-group TBL activities, access to the right space is essential: large rooms that can accommodate 40 to 100 students, for groups to work effectively in small teams of 5 to 7 students. Another difficulty is access to Learning Management Systems (LMS) across different programs and disciplines. For example, Chan et al 24 and Wheeler et al 22 both reported the LMS requirements as potential barriers to the implementation of interprofessional TBL. We have summarized both the benefits and challenges of implementing interprofessional TBL in Table 1.
Benefits and challenges of interprofessional TBL for students, faculty, and institutes.

Abbreviations: MCQ, multiple-choice questions; TBL, team-based learning.
Conclusions
Although university education of professionals involves preparing students for responsible practice, often the first time health professionals work together is as new graduates. Formal university education has a responsibility to implement IPE to prepare health professional students for their graduate roles in interprofessional teams, where shared learning continues. 16 Interprofessional TBL provides an opportunity for students to work together in newly formed teams. The social interactions and exchanges promoted by the different steps of TBL uniquely equip students with the skills and incentive to contribute to and understand the social capital inherent in interdisciplinary teams. Aside from tangible and transferrable teamwork and communication skills gained within interprofessional TBL, we suggest that the cultivation of social capital raises students’ awareness of the importance of interprofessional teamwork, motivating them to collaborate effectively with other professions once they enter the workforce. As a relatively new instructional format in health professional education, a number of empirical questions remain outstanding with respect to interprofessional TBL, such as the best years for implementation; the optimal numbers of disciplines; discipline-specific outcomes; the role of peer review; and importantly, longitudinal follow-up to explore to what extent trust built in TBL is transferable to the workforce.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AB, CvD, and EM jointly developed the structure and content of the paper. All authors agreed on and approved the final manuscript.