
Abstract
Subjective ratings of communication function reflect both auditory sensitivity and the situational, social, and emotional consequences of communication difficulties. Listeners interact with people and their environment differently, have various ways of handling stressful situations, and have diverse communication needs. Therefore, understanding the relationship between auditory and mental health factors is crucial for the holistic diagnosis and treatment of communication difficulty, particularly as mental health and communication function may have bidirectional effects. The goal of this study was to evaluate the degree to which social anxiety and negative affect (encompassing generalized anxiety, depression, and anger) contributed to subjective communication function (hearing handicap) in adult listeners. A cross-sectional online survey was administered via REDCap. Primary measures were brief assessments of social anxiety, negative affect, and subjective communication function measures. Participants were 628 adults (408 women, 220 men), ages 19 to 87 years (mean = 43) living in the United States. Results indicated that individuals reporting higher social anxiety and higher negative affect also reported poorer communication function. Multiple linear regression analysis revealed that both negative affect and social anxiety were significant and unique predictors of subjective communication function. Social anxiety and negative affect both significantly, and uniquely, contribute to how much someone feels a hearing loss impacts their daily communication function. Further examination of social anxiety and negative affect in older adults with hearing loss may help researchers and clinicians understand the complex interactions between mental health and sensory function during everyday communication, in this rapidly growing clinical population.
Introduction
The World Health Organization estimates that by the year 2030 1.9 billion people will be living with hearing loss (WHO, 2021). Although it is most common in older adults, with approximately 50% of adults over the age of 70 years experiencing hearing loss (Goman and Lin 2016), the process of gradual hearing decline begins in middle age or earlier (Morrell et al. 1996). The gold standard measure of hearing ability, hearing sensitivity, is performed using pure tone audiometry. However, pure tone thresholds have limited predictive ability for determining who may be experiencing difficulty with communication, particularly in background noise (Vermiglio et al. 2012). Furthermore, impaired sensitivity is not a good predictor of who will seek out and use hearing aids (Laplante-Lévesque, Hickson and Worrall 2012). In fact, a main driver for seeking hearing health care is a person's self-perceived impairment in daily life functions that they attribute to a hearing loss, typically referred to as their hearing handicap (Ventry and Weinstein 1982). Increased hearing handicap is prevalent in middle and older adulthood (Hannula et al. 2011; Tremblay et al. 2015; Wiley et al. 2000), is associated with reduced quality of life (Gopinath et al. 2012), and is a better predictor of hearing health behaviors than audiometrically defined hearing loss (Fischer et al. 2009; Laplante-Lévesque, Hickson and Worrall 2012). Given its importance to clinical treatment of hearing loss, a better understanding of the factors influencing subjective communication function is critical.
There is increasing interest in how hearing health interfaces with other facets of mental and physical health. For example, hearing loss is associated with an increased risk for depression, whereby adults with depression are more likely to report having difficulty with their hearing (Golub et al. 2020; Rutherford et al. 2018). Recent studies also indicate a higher prevalence of anxiety symptoms in people who also report having vision and hearing loss (Shoham et al. 2019; Park et al. 2024). Less well understood is how hearing health may be related to social anxiety, which is defined as fear of negative evaluation, embarrassment, or humiliation in situations in which one can be observed by others (including social interactions). Although some anxiety in social contexts is normal, social anxiety can become debilitating when it leads people to avoid situations that are important to their goals, at which point social anxiety disorder may be diagnosed. Social anxiety disorder is common and is associated with reports of significant impairment in interpersonal roles (Ruscio et al. 2008), and it is a unique predictor of impairments in friendships (Rodebaugh 2009). Importantly, the available evidence suggests that challenges with interpersonal function and loneliness predict future social anxiety more strongly than vice versa (Lim et al. 2016; Rodebaugh, Fernandez and Levinson 2012), although social anxiety does appear to prospectively predict loneliness (Lim et al. 2016). As such, it is easy to imagine that hearing difficulties and social anxiety could have a similar reciprocal relationship as seen with loneliness. Perceived difficulties in communication could lead to social anxiety and withdrawal, which could lead to further perceived communication difficulties when the listener is confronted with subsequent subjectively stressful listening situations.
Understanding the relationship between hearing handicap and anxiety in social situations is therefore important for at least two reasons. First, if social anxiety is driven in part by auditory factors, auditory rehabilitation (such as the use of a hearing aid) may not only improve hearing, but also lower social anxiety. Second, the converse may also be true—that is, if hearing handicap is affected by social anxiety, addressing this mental health concern may improve self-perceived communication function. The existence of multiple efficacious treatments for social anxiety (Mayo-Wilson et al. 2014) would support such an intervention.
To elucidate the link between subjective communication function and social anxiety we collected self-report survey data on subjective hearing health and social anxiety from adults aged 19–87 years. We also assessed negative affect because a general tendency toward experiencing unpleasant emotions is related to a wide range of mental health conditions, including generalized anxiety, social anxiety, and depression (Kotov et al. 2017). It is thus important to determine whether any effect that appears to be due to social anxiety is instead more related to this underlying general tendency. We used this cross-sectional sample to test for a significant relationship between hearing handicap and social anxiety and to determine if social anxiety uniquely contributed to self-reported hearing handicap scores in a large sample of adults with a range of self-reported hearing abilities. We hypothesized that listeners with more social anxiety would report greater difficulties with communication and that both social anxiety and negative affect would significantly contribute to the heterogeneity in subjective hearing handicap scores.
Method
Participants
Participants were recruited through the Washington University School of Medicine Research Participant Registry, Facebook, and Twitter, under a protocol approved by the Washington University in St. Louis Institutional Review Board (#202105175). Participants aged 18 years or older with and without self-reported hearing loss were included.
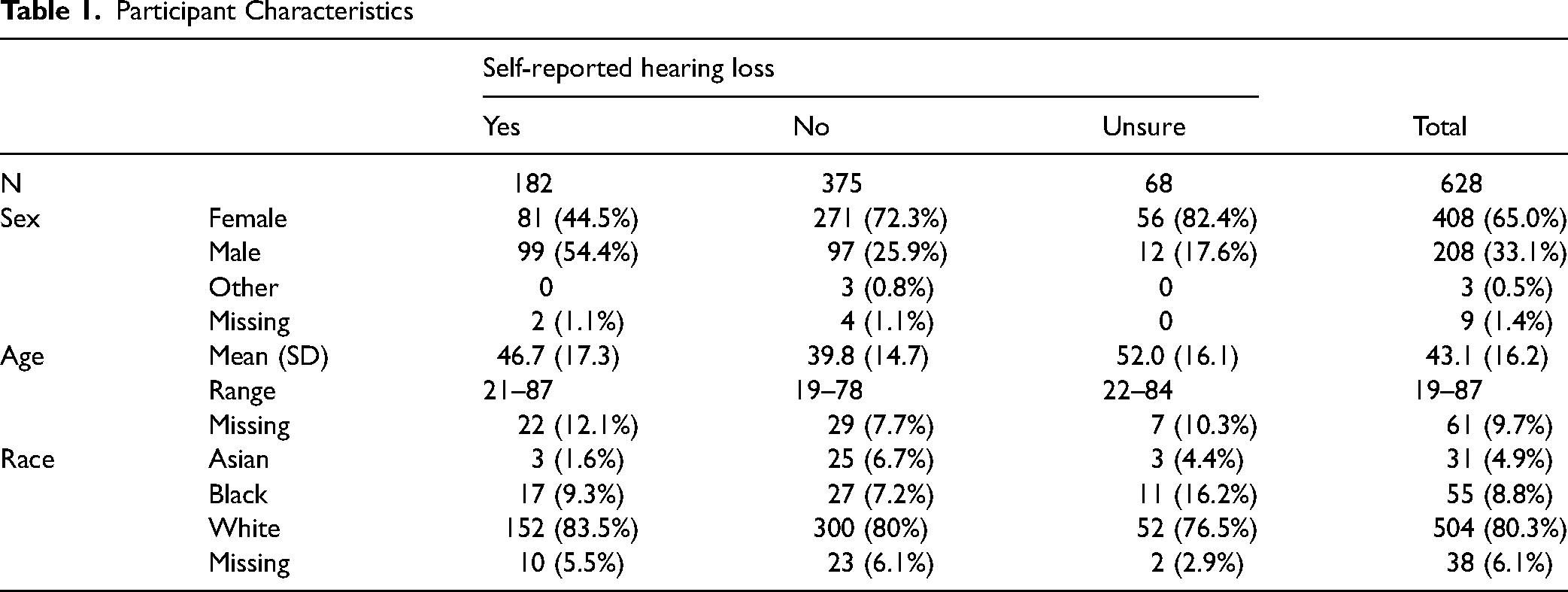
A total of 628 participants were included in the study. Participants were aged 19–87 years (M = 43.06, SD = 16.2) and the majority were female (65%, n = 408) and white (80.3%, n = 504). Twenty-nine percent of respondents self-reported hearing loss severity (n = 182) as moderate (14%, n = 88), severe (4.3%, n = 27), or profound (0.8%, n = 5). Of those reporting hearing loss, hearing aids were used at least some of the time (49.5%, n = 90) and provided significant benefit at least some of the time (47.8%, n = 87).
Materials
Hearing status was determined by self-report (Do you have a hearing loss? Possible answers: Yes, No, Unsure). Participants were also asked a series of questions regarding their hearing health, which can be found in supplemental materials. Demographic information for the study sample is shown in Table 1. For our variables of interest (self-reported hearing handicap, social anxiety, and negative affect), we used composite scores of the following measures, described by variable.
Participant Characteristics
Self-Reported Hearing Handicap
Hearing Handicap for the Elderly - Screening (HHIE-S)
The HHIE-S is a 10-question screening survey that evaluates the perceived social and emotional effects of hearing loss on an individual's daily activities. Questions are scored as yes (4 points), sometimes (2 points), and no (0 points) with total scores ranging from 0 (no handicap) to 40 (maximum handicap). A score of ≥ 10 indicates the presence of a hearing handicap and the measure has been shown to be a reliable and valid measure of hearing difficulties (Lichtenstein, Bess and Logan 1988).
15-item Speech, Spatial, and Qualities of Hearing Scale (15iSSQ)
The original Speech Spatial and Qualities of Hearing Scale is a 49-item questionnaire designed to measure an individual's hearing ability across a variety of listening contexts based on a 10-point Likert scale (Gatehouse and Noble 2004). The 15iSSQ (Moulin et al. 2019) is a shortened version of the SSQ that maintains the original three subscales (speech, spatial, and qualities) with greater discriminatory power between normal hearing and hearing-impaired participants. Each item describes a listening scenario and asks the participant to rate how well they can do what is being described with 0 being unable and 10 being perfectly able, thus, lower scores indicate lower ability to perform. Scores were reversed prior to creating the composite.
Negative Affect
Patient-Reported Outcomes Measurement Information System (PROMIS)
Mental health was evaluated using PROMIS item bank instruments for Anxiety (v1.0), Depression (v1.0), and Anger (v1.1) (Cella et al. 2010), which represent the mental health domain of negative affect (Cook et al. 2016). These scales were administered as computer adaptive tests in which a participant's response to each item guides the system's choice of subsequent items from the full item bank. Questions continue until the standard error drops below a specified level or the maximum number of questions has been answered, whichever occurs first. Example questions from each PROMIS subdomain instrument are included in the supplemental materials. Raw scores are standardized to a t-score (M = 50, SD = 10) with a higher t-score indicating more of the concept being measured.
Social Anxiety
Social Interaction Anxiety Scale (SIAS-6) & Social Phobia Scale (SPS-6)
The SIAS-6 and SPS-6 are two short form scales designed to measure fears of specific scrutiny and more generalized anxieties around social interactions as factors of social anxiety (Peters et al. 2012), which we combined as an overall measure of social anxiety. Items are scored on a 5-point scale ranging from 0 (not at all characteristic or true of me) to 4 (extremely characteristic or true of me). The shortened scales maintain satisfactory psychometric validity and internal consistency and discriminate well between anxious and non-anxious respondents (Le Blanc et al. 2014). Example questions from each scale are included in supplemental materials.
Procedure
Data were collected and stored on the Washington University instance of REDCap (Research Electronic Data Capture) which is maintained by the Institute for Informatics, Data Science, and Biostatistics Informatics Core Services (Harris et al. 2009, 2019). The survey was distributed via public URL and initiated 1378 times. Upon review, 553 submissions were removed after they were determined to be bad faith responses. Removal criteria included blocks of responses that displayed patterned or identical data across instruments, synchronized survey completion identified by timestamps, logical inconsistencies such as reported hearing loss in one ear and hearing aid use in the other ear or years of education inconsistent or out of proportion with degree selected (e.g., 12 years of education and doctoral degree), and duplicate submissions from the same email address. We further restricted inclusion to those who had completed all PROMIS measures and at least one hearing handicap measure, resulting in 628 usable participants.
Data Analysis
All analyses were completed in R (Version 4.3.2). Data and analysis scripts are available at https://osf.io/he3qu/. Instruments for each variable (self-reported hearing handicap, negative affect, and social anxiety) were scored and standardized before creating composite scores. Bivariate relationships were examined, via Pearson correlation, to determine the relationships between our three main variables of interest: hearing handicap, social anxiety, and negative affect. Assumptions for linear regression were met (see analysis scripts for test results). Linear regression was used to determine the unique contributions of each variable to hearing handicap scores. We completed our regression in steps, with
Results
Distributions and bivariate correlations of outcome measures are shown in Figure 1. Pearson correlation revealed significant moderate relationships between each of our variables of interest, with participants with higher hearing handicap also reporting higher negative affect (r = .41, p < .001) and social anxiety (r = .47, p < .001) and participants with higher negative affect reporting higher levels of social anxiety (r = .51, p < .001).

Characterization of outcome measurements and their relationship to each other. The diagonal shows score distributions for each outcome measure. Off-diagonal panels show either a scatterplot or Pearson correlation value for the variables indicated. *** = p < .001.
We used linear regression to determine the unique contributions of age, negative affect, and social anxiety to self-reported hearing handicap. Age, negative affect, and social anxiety each uniquely and significantly contributed to self-reported communication function (Table 2
Regression Results

A significant b-weight indicates the semi-partial correlation is also significant.
b represents unstandardized regression weights.
sr2 represents the semi-partial correlation squared.
Square brackets are used to enclose the lower and upper limits of a confidence interval.
* indicates p < .05. ** indicates p < .01.
We then completed further exploratory analyses to identify if the relationship amongst the variables changed depending on self-reported hearing loss status (Yes, No, Unsure). Figure 2 shows the bivariate relationships and score distributions separated by hearing status.

Characterization of outcome measurements and their relationship to each other as a function of hearing status (“yes” in purple, “no” in green, and “unsure” in orange). Conventions as in Figure 1.
We then added the self-reported hearing loss variable into our regression analyses, which increased the amount of variance in hearing handicap explained from 32% to 63%, with negative affect, social anxiety, and self-reported hearing loss making significant and unique contributions (Table 3
Regression Results with the Addition of Self-Reported Hearing Loss Status

A significant b-weight indicates the semi-partial correlation is also significant.
b represents unstandardized regression weights.
sr2 represents the semi-partial correlation squared.
Square brackets are used to enclose the lower and upper limits of a confidence interval.
* indicates p < .05. ** indicates p < .01.
Discussion
In this study, we asked people to rate their hearing handicap via two commonly used clinical scales, and assessed how much that hearing handicap was accounted for by their self-reported levels of negative affect and social anxiety. The primary finding of note was that hearing handicap was associated with both negative affect and social anxiety, with higher levels of negative affect and social anxiety correlating with higher levels of hearing handicap. Additionally, negative affect and social anxiety each uniquely and significantly accounted for variance in self-reported hearing handicap scores. It is particularly notable that we identified a link between subjective communication difficulty and social anxiety. This relationship has received very little attention in the literature, with research restricted to pediatric and adolescent populations (Ariapooran and Khezeli 2021; Theunissen et al. 2012; Broekhof, Bos and Rieffe 2021) or late deafened adults seeking cochlear implantation (Knutson, Johnson and Murray 2006).
An association between hearing handicap and social anxiety suggests that both conditions may reciprocally relate to each other over time. That is, we propose that hearing handicap can lead to social anxiety (e.g., because people fear they do not understanding others in social situations and being negatively evaluated for miscommunications) and that social anxiety can lead to social avoidance and therefore decreased communication function (e.g., individuals become even more avoidant of noisy social situations). Gallagher and colleagues (2024), for example, found that roughly 20% of adults with hearing loss reported social avoidance due to their hearing loss. Although it is traditional to try to interpret cross-sectional relationships as if they provide a guide to how large a level of prediction is expected over time, we will refrain from this practice here because we expect complicated causal relationships between hearing handicap, social anxiety, and other variables. Accordingly, what is important is whether there is an association. Understanding how large the association is and how it plays out over time will require data that include repeated measurement over time. An additional limitation of this online study was the lack of an objective assessment of auditory function. Self-reported hearing loss, while correlated with audiometrically defined hearing loss, is subjective. In future studies of the relationship between hearing and anxiety it would be useful to include an objective measure of hearing.
There is ample work, particularly in older adults, linking hearing loss to depression (Brewster et al. 2018; Golub et al. 2020; Rutherford et al. 2018), and some, but much less, information regarding the association of hearing loss and generalized anxiety (Contrera et al. 2017; Zhang et al. 2023). Therefore, there is established evidence that, in the context of normal aging, hearing loss may put people at increased risk for developing symptoms of depression and anxiety. Furthermore, depression and hearing loss have been linked to social isolation and loneliness (Brewster et al. 2018; Rutherford et al. 2018; Weinstein and Ventry 1982; Shukla et al. 2020), which can increase one's risk for cognitive decline and dementia (Joyce et al. 2021; Shen et al. 2022). Our current findings suggest that social anxiety should also be considered in this context, as it likely also contributes to diminished social engagement. Given the high rates of comorbidity between social anxiety and depression and the established link between depression and hearing loss, further examination of the temporal relationship between social anxiety, depression, and hearing loss may be warranted.
Moreover, we believe the distinction between social anxiety and negative affect (including generalized anxiety) is critical in the context of hearing health care. As reflected in the references provided above, negative affect correlates with many outcomes; so too does generalized anxiety. Measures of these factors, however, are purposefully global and thus unlikely to guide us to intervention points relevant for hearing. Knowing that someone with high hearing handicap struggles with anxiety generally might lead to a referral to a mental health clinician. That clinician's first step will almost certainly be to narrow down the type of anxiety. However, anxiety may have pernicious relationships with hearing handicap without the presence of a mental health condition, and there may be appropriate interventions that audiologists can suggest without needing the support of mental health clinicians. To determine whether this is the case, we must investigate how specific forms of anxiety relate to hearing handicap, and we propose that social anxiety is a prime candidate for further evaluation.
In conclusion, we provide evidence consistent with the literature that self-reported hearing loss is related to negative affect, as well as novel evidence suggesting a unique relationship between hearing handicap and social anxiety in a large cross-sectional sample of adults. Further work focusing on specific clinical populations (e.g., older adults with audiometrically defined hearing loss) and studies using longitudinal designs will be vital in understanding how subjective communication function and hearing sensitivity interact in a holistic model of patient wellness. Establishing the relationship between hearing loss and mental health has significant clinical implications, as it may open pathways for ameliorating negative mental health symptoms through auditory rehabilitation. As the ultimate goal of hearing health care is improving overall communication and quality of life, the identification of contributing factors to hearing handicap is timely and essential to future improvement in the treatment of hearing loss.
Supplemental Material
sj-docx-1-tia-10.1177_23312165251317925 - Supplemental material for Social Anxiety, Negative Affect, and Hearing Difficulties in Adults
Supplemental material, sj-docx-1-tia-10.1177_23312165251317925 for Social Anxiety, Negative Affect, and Hearing Difficulties in Adults by Katrina (Kate) S. McClannahan, Sarah McConkey, Julia M. Levitan, Thomas L. Rodebaugh, and Jonathan E. Peelle in Trends in Hearing
Supplemental Material
sj-docx-2-tia-10.1177_23312165251317925 - Supplemental material for Social Anxiety, Negative Affect, and Hearing Difficulties in Adults
Supplemental material, sj-docx-2-tia-10.1177_23312165251317925 for Social Anxiety, Negative Affect, and Hearing Difficulties in Adults by Katrina (Kate) S. McClannahan, Sarah McConkey, Julia M. Levitan, Thomas L. Rodebaugh, and Jonathan E. Peelle in Trends in Hearing
Supplemental Material
sj-docx-3-tia-10.1177_23312165251317925 - Supplemental material for Social Anxiety, Negative Affect, and Hearing Difficulties in Adults
Supplemental material, sj-docx-3-tia-10.1177_23312165251317925 for Social Anxiety, Negative Affect, and Hearing Difficulties in Adults by Katrina (Kate) S. McClannahan, Sarah McConkey, Julia M. Levitan, Thomas L. Rodebaugh, and Jonathan E. Peelle in Trends in Hearing
Footnotes
Acknowledgments
The authors would like to thank the participants who completed the study and Dr. Michael Strube for his guidance regarding statistical analyses.
The authors wish to acknowledge the Siteman Cancer Center's National Cancer Institute (NCI) Cancer Center Support Grant P30 CA091842, the Washington University Institute of Clinical and Translational Sciences Grant UL1 TR002345 from the National Center for Advancing Translational Sciences (NCATS), and the I2DB and Becker Library REDCap Support teams for supporting the Washington University instance of REDCap (Research Electronic Data Capture). NCI and NCATS are part of the National Institutes of Health (NIH).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.