
Abstract
This nationwide retrospective cohort study examines the association between adults with hearing loss (HL) and subsequent injury risk. Utilizing data from the Taiwan National Health Insurance Research Database (2000–2017), the study included 19,480 patients with HL and 77,920 matched controls. Over an average follow-up of 9.08 years, 18.30% of the 97,400 subjects sustained subsequent all-cause injuries. The injury incidence was significantly higher in the HL group compared to the control group (24.04% vs. 16.86%, p < .001). After adjusting for demographics and comorbidities, the adjusted hazard ratio (aHR) for injury in the HL cohort was 2.35 (95% CI: 2.22–2.49). Kaplan–Meier analysis showed significant differences in injury-free survival between the HL and control groups (log-rank test, p < .001). The increased risk was consistent across age groups (18–64 and ≥65 years), with the HL group showing a higher risk of unintentional injuries (aHR: 2.62; 95% CI: 2.45–2.80), including falls (aHR: 2.83; 95% CI: 2.52–3.17) and traffic-related injuries (aHR: 2.38; 95% CI: 2.07–2.74). These findings highlight an independent association between HL and increased injury risk, underscoring the need for healthcare providers to counsel adult HL patients on preventive measures.
Introduction
The escalating global incidence of sensorineural hearing loss (HL) is becoming a significant public health concern (GBD 2017 Disease and Injury Incidence and Prevalence Collaborators, 2018; Wilson et al., 2017). Recent studies reveal that between 2017 and 2019, HL emerged as the third most common cause of functional impairment. During this period, the prevalence of HL of varying types and degrees affected approximately 1.4 billion individuals, constituting about 18% of the global population. This figure marks a substantial increase from the 0.75 billion individuals identified with similar impairments in 1990. Projections for 2024 suggest that over 430 million people will require rehabilitation services for disabling HL, with estimations rising to more than 700 million by 2050 (World Health Organization, 2024).
Concurrently, the years lived with disability due to HL has surged from 22 million in 1990 to 40 million in 2019 (GBD 2017 Disease and Injury Incidence and Prevalence Collaborators, 2018; Li et al., 2022). This increase signifies a global rise in this condition's economic and financial burden (Brown et al., 2018). The World Health Organization (WHO) estimates the annual global cost of unaddressed HL at approximately US$980 billion, accounting for healthcare, educational, and societal costs and lost productivity. These findings underscore the urgency of addressing HL as a critical public health issue, necessitating coordinated global efforts for effective management and prevention strategies (Olusanya et al., 2019).
HL significantly impacts health and quality of life across all age demographics. Studies by Xu et al. (2021) and others have demonstrated its pervasive effects. In early childhood, HL can hinder the optimal acquisition of speech and language (Kennedy et al., 2006), potentially delaying the development of both verbal abilities and nonverbal intelligence (Emmett & Francis, 2014). Among teenagers and young adults, even mild HL is frequently linked to early school dropout, unemployment, or underemployment, as observed in studies by Jarvelin et al. (1997) and Shan et al. (2020).
In the context of older adults, Genther et al. (2015) found that HL is associated with a 20% increased risk of mortality, even after adjusting for cardiovascular and other risk factors. Xu et al. (2021) further identified that this association is significantly mediated by fall-related injuries, including both serious and minor injuries, particularly in middle-aged and older adults. Age-related HL has been shown to compromise gait control during daily activities (Foster et al., 2022; Sakurai et al., 2021), underscoring the well-established link between HL and increased fall risk in older adults. This link is supported by a breadth of literature, including studies by Grue et al. (2009), Lin and Ferrucci (2012), Heitz et al. (2019), Huang et al. (2022), Jiam et al. (2016), Wang et al. (2022), Lin et al. (2018), Lopez et al. (2011), Powell et al. (2021), and Criter and Gustavson (2020).
The heightened incidence of drop attacks in patients with HL, coupled with nonfatal falls as a predominant cause of injury among adults, as reported by Bergen et al. (2016), Drew and Xu (2020), and Xu and Drew (2016), led to the hypothesis that HL may be associated with increased risk of subsequent injury across individuals of all age groups. Consequently, this study examined the risk of various injuries following the diagnosis of HL.
Methods
Data Sources
This retrospective cohort study included outpatient and inpatient data between 2000 and 2017, obtained from the Taiwanese Longitudinal Health Insurance Database, a subset of Taiwan's National Health Insurance (NHI) Research Database. The study was reviewed and approved by the Institutional Review Board of Cardinal Tien Hospital (CTH-110-3-5-044). The requirement for written informed consent was waived due to the analysis of deidentified data.
Study Design and Participants
In this retrospective cohort study, an initial random selection of 1,949,101 patients was made from the database. Of these, 27,159 patients with HL were enrolled, identified by diagnostic codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) for data from 2000–2015, and the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) for data from 2016–2017. Eligible individuals were those diagnosed with HL at least three times and had undergone one or more of the following tests: pure tone audiometry, speech audiometry, sound field testing, or brain stem response. Exclusions were made for patients with HL diagnosed before 2000, injuries occurring before the study period, individuals under 18 years of age, those with unknown sex, and those without tracking. Patients with conditions such as epidemic vertigo, benign neoplasm of cranial nerves, vertiginous syndromes, other vestibular system disorders, sudden HL, dizziness or giddiness, post-concussion syndrome, or transient brain injury—all of which could significantly affect fall or other injury risks—were also excluded from the study.
Ultimately, 19,480 patients with HL diagnoses during the study period were included. A control group was introduced at a 1:4 patient-to-control ratio based on propensity score matching for sex, age, underlying disease, and index date. This resulted in 77,920 patients who met the same exclusion criteria as the study cohort. The index date was defined as when HL diagnosis met the inclusion criteria. A detailed study flowchart is presented in Figure 1, with diagnostic codes for inclusion and exclusion criteria listed in Supplemental Table S1.
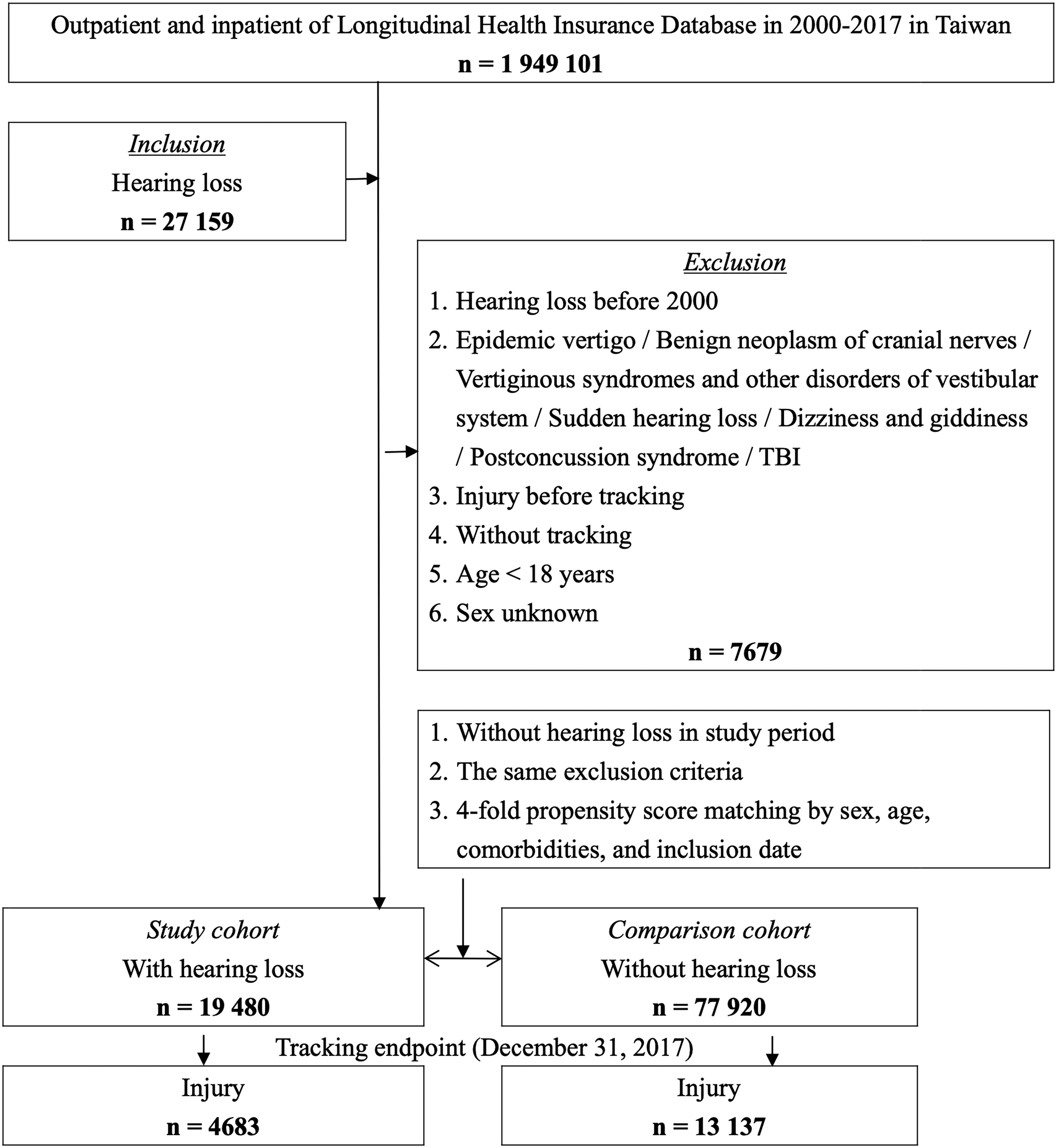
Flow diagram of study sample selection.
Outcome Measures
Participants in the study were followed from the index date until the occurrence of an injury, withdrawal from the NHI program, or the end of the follow-up period, whichever came first. We tracked the incidence of injury for both cohorts until December 31, 2017. Injuries were identified using diagnostic codes from the ICD-9-CM codes 800 to 999 and ICD-10-CM codes V01 to Y89, along with E-codes in the patient records. These E-codes provided detailed information on the events, circumstances, and conditions leading to the injuries and specified external causes, facilitating additional categorization of injuries.
The study calculated crude hazard ratios (HRs) and adjusted HRs (aHRs) for individual subtypes of injuries within the HL and non-HL cohorts. Injury Severity Scores (ISSs), ranging from 0 to 75, were employed to evaluate injury severity. An ISS exceeding 16 is categorized as major trauma and a catastrophic illness in Taiwan's NHI system, granting patients with such conditions an exemption from copayments.
Potential Confounders
To calculate aHRs, the study controlled for several confounding factors: sex, age or age group, insurance premium, underlying disease, season of the year, geographic location within Taiwan, urbanization level, and the level of care received. The insurance premium levels were employed as indicators of the socioeconomic status of the insured individuals. Additionally, the study documented the seasons in which injuries occurred in both cohorts, and the last visit date for participants who did not experience any injury event. The urbanization level was determined based on population density and various indicators reflecting the city’s developmental status. The study also stratified individuals based on the presence or absence of multiple comorbidities, either before or on the index date, to facilitate comparison between those with and without these comorbid conditions.
The cohort with HL was stratified into subgroups based on patients’ histories, including those who underwent sound field tests and those with age-related macular degeneration (AMD), cataract, and lens operations. This stratification allowed comparing risks associated with individual injury subtypes within these subgroups.
The study identified various injury subtypes to facilitate a more comprehensive discussion of the potential mechanisms behind these injuries. This identification was based on the E-codes from the International Classification of Diseases recorded in the patient's data. These E-codes detailed the events, circumstances, and conditions leading to the injuries and further specified the external causes, thereby aiding in the supplemental categorization of the injuries. Subgroup analyses were subsequently performed to examine these distinctions in detail.
Statistical Analysis
All analyses in this study were conducted using SPSS Statistics version 22 (IBM, Armonk, NY, USA). The researchers reported the incidence rate as events per 105 person-years. To evaluate the distributions of categorical and continuous variables, the chi-square test and Student's t-test were employed, respectively. Furthermore, the study utilized multivariate Cox proportional hazards regression to determine the risk of injury, presenting the findings as HRs. The Kaplan–Meier method and log-rank tests were applied to estimate the differences in the risk of injury between the cohorts with and without HLs Two-tailed 95% confidence intervals (CIs) and p-values were also calculated. p-Values below .05 were considered statistically significant.
Results
Baseline Characteristics
Table 1 presents the baseline characteristics of both the HL and non-HL cohorts, stratified by comorbidities. The mean age of the participants was 59.95 years with a standard deviation (SD) of 16.62, and 59.19% of the patients were male. The average follow-up durations for the HL and non-HL cohorts were 9.15 years and 9.06 years, respectively, as detailed in Supplemental Table S2. There were no significant differences between the cohorts regarding sex, age, age groups, and underlying diseases. Supplemental Table S3 records the characteristics of the participants either at the end of the tracking period or at their last medical visit.
Characteristics of Participants in the Baseline.

Note. AID: autoimmune disease; AIS: acute ischemic stroke; CAD: coronary heart disease; CI: confidence interval; CKD: chronic kidney disease; COPD: chronic obstructive pulmonary disease; NTD: New Taiwan Dollar; SD: standard deviation.
Kaplan–Meier Model for Injury-Free Survival
During the study period, 18.30% of participants sustained some form of injury. The incidence of injury was significantly higher in the HL group compared to the non-HL group (24.04% vs. 16.86%, p < .001). Kaplan–Meier analysis demonstrated significant differences in injury-free survival between patients with and without HL throughout the tracking period (log-rank test, p < .001, as depicted in Figure 2A). Similar results were observed in subgroup analyses. For both age groups, 18 to 64 years and over 64 years, there were significant differences in injury-free survival between patients with and without HL (log-rank test, p < .001), illustrated in Figure 2B and C.

Kaplan–Meier curves showing the injury-free survival of (A) overall, (B) 18-to-64-year age groups, and (C) ≥ 64-year age groups.
Supplemental Table S4 enumerates the factors associated with injury as identified through Cox regression analysis. Within the HL cohort, the crude HR for injury was calculated at 2.40 (95% CI: 2.100–2.530). Following adjustments for sex, age or age group, insurance premium, underlying disease, season, geographic location within Taiwan, urbanization level, and level of care, the aHR stood at 2.35 (95% CI: 2.219–2.487). Even when stratified by these factors, subgroups within the HL cohort consistently exhibited a higher risk of injury than that of their control counterparts, as detailed in Supplemental Table S5.
Subgroup Analyses
Table 2 presents the results of the Cox regression analysis concerning injury types in both cohorts. The study identified a significantly elevated risk of unintentional subsequent injuries among patients with HL (aHR: 2.62; 95% CI: 2.45–2.80) compared to those without HL. In contrast, the risk of intentional injuries was not significantly higher (aHR: 1.34; 95% CI: 0.86–3.58) in the HL group. Additionally, patients with HL were found to have an increased risk of traffic injuries (aHR: 2.38; 95% CI: 2.07–2.74) and falls (aHR: 2.83; 95% CI: 2.52–3.17). Furthermore, these patients also exhibited a higher risk of injuries with ISSs of less than 16 (aHR: 2.28; 95% CI: 2.14–2.38) and 16 or greater (aHR: 2.72; 95% CI: 2.57–2.95) compared to the non-HL cohort.
Risk of Injury Subtypes Stratified by Age Groups.

Note. aHR:: adjusted hazard ratio; CI: confidence interval; PYs: Person-years.
Sensitivity Analyses
Table 3 displays the results of the Cox regression analysis of injuries in patients categorized by their history of sound field testing, AMD, cataract, and lens operations. Within the HL cohort, patients who had undergone sound field testing exhibited a significantly higher risk of injury than those who had not (aHR: 1.45; 95% CI: 1.05–2.00). However, the risk of injury did not significantly differ among subgroups with a history of cataracts (aHR: 1.03; 95% CI: 0.51–1.57) or lens operation (aHR: 0.95; 95% CI: 0.48–1.50).
Factors of Injury Stratified by Age Groups among Different Hearing Loss Subgroups.
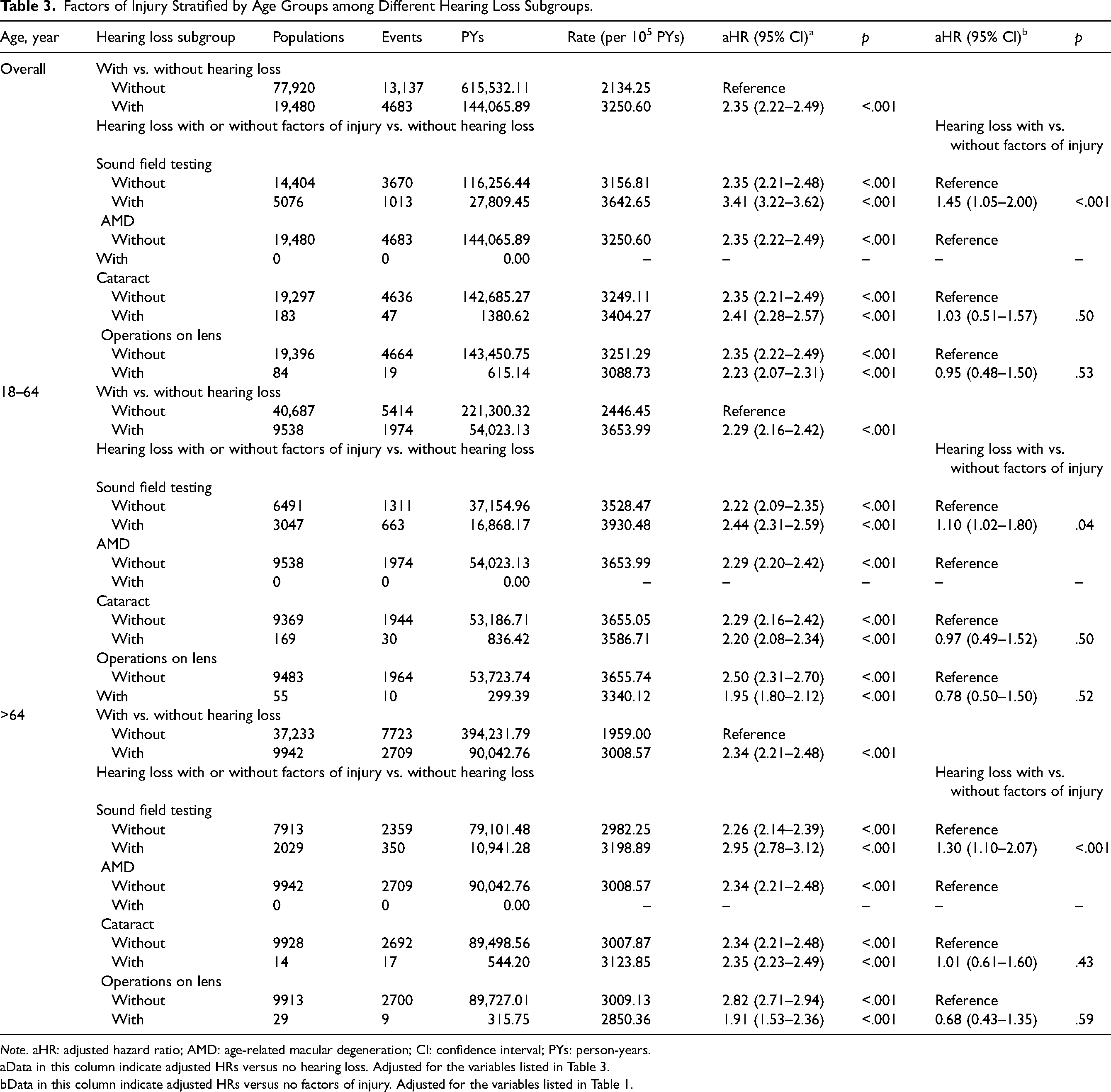
Note. aHR: adjusted hazard ratio; AMD: age-related macular degeneration; CI: confidence interval; PYs: person-years.
Data in this column indicate adjusted HRs versus no hearing loss. Adjusted for the variables listed in Table 3.
Data in this column indicate adjusted HRs versus no factors of injury. Adjusted for the variables listed in Table 1.
Discussion
This study elucidate the association between HL and all-cause injury in adults across all age groups. The findings indicate that patients with HL experience a higher risk of subsequent injury compared to individuals without HL, matched based on propensity scores. This pattern persisted across different age groups, specifically in the 18-to-64 and ≥ 65-year age groups, and was consistent across various injury subtypes. Notably, the risks associated with both minor injury (ISS < 16) and major trauma (ISS ≥ 16) were found to be elevated in the HL cohort compared to the non-HL cohort.
Interestingly, our study revealed significant differences of insured premium, location, urbanization level and level of care between HL and non-HL group (Table 1). The findings on socioeconomic disparities among individuals with HL and their associated risk of unintentional injuries are particularly noteworthy. Socioeconomic status is critical in determining access to healthcare services, including the timely diagnosis and treatment of HL. Individuals from lower socioeconomic backgrounds may face financial constraints, transportation issues, and limited healthcare availability, leading to delayed access to necessary interventions.
For individuals with HL, particularly those in lower socioeconomic groups, access to care is a major concern. These individuals often experience higher rates of HL and face challenges in obtaining audiological assessments and hearing aids, further increasing the risk of unintentional injuries. Addressing these disparities is crucial for improving health outcomes and ensuring equitable access to care.
The interaction between socioeconomic factors and injury risk underscores the need for targeted public health initiatives aimed at improving healthcare access for vulnerable populations. By addressing these barriers, we can potentially reduce the incidence of unintentional injuries and significantly enhance the overall quality of life for those with HL.
Acknowledging HL as a modifiable risk factor for subsequent injury in adults is essential for public health strategies. The coexistence of vision and hearing impairments, or dual sensory impairment, independently predicts a heightened risk of falls and accidental injuries at work in older adults, as evidenced by studies from Gopinath et al. (2016), Grue et al. (2009), and Palmer et al. (2015). Gopinath et al. (2016) found that individuals with best-corrected dual sensory impairment were twice as likely to experience incidental falls as those without sensory loss.
Numerous studies have established a connection between self-reported HL and an increased risk of falls or injuries, including research by Grue et al. (2009), Lin and Ferrucci (2012), Heitz et al. (2019), Huang et al. (2022), Jiam et al. (2016), Wang et al. (2022), Lin et al. (2018), Lopez et al. (2011), Powell et al. (2021), and Criter and Gustavson (2020). However, some studies, like those by Lee et al. (2011) and Purchase-Helzner et al. (2004), have reported contrary findings. In 2016, Jiam et al. conducted a systematic review of 12 studies and determined that the risk of falling was 2.39 times greater in older adults with HL than those with normal hearing. Powell et al. (2021), in a cross-sectional study involving a pooled analysis of patients aged 50 years and older, revealed that moderate or greater hearing difficulties were associated with a 1.26 to 1.29 times higher risk of injuries or falls. Kwan et al. (2011) noted that while not all falls result in injuries, 60% to 75% of ethnically Chinese older adults who reported falls sustained injuries. Furthermore, Heitz et al. (2019) concluded that the risk of nonfatal fall-related injury was 1.60 times higher among individuals with HL compared to those without. Additionally, a cross-sectional analysis by Lin et al. (2018) from 2007 to 2015, involving a sample of 232.2 million individuals aged 18 years or older in the National Health Interview Survey in the United States, revealed a consistently higher risk of accidental injury among individuals with varying degrees of hearing difficulties compared to those with excellent hearing.
Contrastingly, a cohort study based on interviews by Purchase-Helzner et al. (2004), which examined hearing sensitivity and the risk of incident falls and fractures in older women, found no evidence to support the hypothesis that HL is a risk factor for fractures or falls. Similarly, Lee et al. (2011) reported that sensory impairments, such as visual or hearing impairments, were not identified as risk factors for falls in rural Taiwan. However, in these studies, hearing sensitivity was evaluated by inquiring about the patients’ self-perceived hearing status, with descriptions ranging from “good” to “a little trouble hearing,” “moderate,” or “a lot of trouble hearing.” The reliance on subjective self-assessments in these studies could have introduced recall bias, potentially leading to an underestimation of the severity of HL. This bias arises from the possibility that individuals might perceive their hearing issues as less severe than if assessed through a formal diagnosis.
Sound field testing, a variant of pure-tone audiometry, is often used to ascertain hearing thresholds for populations unable to wear or tolerate earphones (Guidelines for the Review of Medical Expenses under NHI 2022). According to Taiwan NHI payment guidelines, sound field testing is limited to patients who require testing for the use of hearing aids or the installation of artificial electronic ears. Thus, we can link the history of receiving sound field testing to hearing impairment of various degrees. The use of sound field testing in this study provides a unique opportunity to assess the relationship between the severity of HL and the risk of unintentional injuries. Participants who underwent sound field testing were likely to have moderate to severe HL, which may correlate with a higher risk of injury. Our findings suggest that individuals with greater HL, particularly those evaluated for amplification, exhibit a significantly increased risk of unintentional injuries compared to those with mild or no HL. This distinction is crucial for understanding the mechanisms underlying injury risk in this population. Overall, our findings underscore the importance of assessing the severity of HL when evaluating the risk of unintentional injuries. Understanding this relationship can inform targeted prevention strategies and interventions for individuals with varying degrees of hearing impairment.
Hearing aids are recognized as a treatment option for imbalance in older adults with HL. Rumalla et al. (2015) conducted a cross-sectional study demonstrating that hearing aid use significantly improves balance and lowers the risk of falls in older adults with HL. However, the present study found that patients with a history of sound field testing exhibited a higher risk of injury (aHR: 1.45) than those without such a history. Riska et al. (2022) found that using hearing aids had no impact on the relationship between self-reported hearing status and the risk of falls or fall-related injuries. Gopinath et al. (2016) noted that users of hearing aids and individuals with severe hearing impairments were more likely to report multiple falls over a five-year period. The lack of a reduced risk of falls with hearing aid use may be attributable to several factors. Firstly, those undergoing hearing aid fitting typically present with worse baseline hearing conditions, potentially compromising safety in daily activities. Secondly, older adults often exhibit suboptimal compliance with hearing aid use, as a survey in Finland by Salonen et al. (2013) indicated, with only 55.4% of participants using their hearing aids daily and 10.7% never using them. Thirdly, in older adults, hearing aid use may be compounded by nonauditory, age-related conditions like visual impairment or reduced manual dexterity due to arthritis (Erber, 2009; Singh et al., 2013).
Hearing aid use, therefore, may not directly cause increased falls in the long term, but rather indicate more severe hearing issues or potential frailty and aging (Gopinath et al., 2016). The effect of hearing aids on the risk of falling or non-falling injury remains uncertain due to limited research. Nevertheless, the use of hearing aids benefits health, as evidenced by improved mood, reduced depression, enhanced quality of life, and increased life expectancy (Chisolm et al., 2007; Kochkin and Rogin, 2000). Hence, despite uncertainties regarding fall risk, the multifaceted benefits of hearing aid use underscore their necessity.
The study identified a significant correlation between HL and subsequent unintentional injury (aHR: 2.62). Falls (aHR: 2.83) and traffic injuries (aHR: 2.38) emerged as the most prevalent types of unintentional injuries among this cohort. Other less common subtypes of unintentional injury, in decreasing order of incidence, included poisoning, suffocation, injuries due to crushing, cutting, or piercing, and those caused by animals. Nonetheless, these injuries were infrequent among the participants. Notably, the incidence rate of injuries from crushing, cutting, or piercing did not significantly differ between individuals with HL and those without. Numerous studies have established the relationship between HL and the occurrence of falls, as mentioned earlier, but there is relatively little research on how HL affects traffic safety. Jörgen (2004) pointed out that adult pedestrians and cyclists with moderate HL face an increased risk of vehicle-related injuries due to difficulty discerning sound sources’ direction. However, the evidence does not support a relationship between hearing impairment and increased risk of motor vehicle crashes for drivers with HL (Dow et al., 2022; Thorslund et al., 2013).
Regarding intentional injuries, the overall risk within the HL cohort did not exceed that in the non-HL cohort. However, the study found a heightened risk of committing homicide or abuse among younger adults with HL compared to those without (aHR: 4.63; 95% CI: 1.09–9.18). This trend might be attributed to the age distribution of homicide offenders. A study by Vernon et al. (1999) compared 27 deaf murderers with the national profile of murderers in the United States, revealing that a majority (82%) of the deaf murderers were aged between 17 and 34 years, closely mirroring the proportion in the national sample (76%). This suggests that younger adults with HL are more commonly implicated in homicide cases. Additionally, the higher prevalence of psychosis among younger individuals with HL could contribute to this observation. Research by Gevonden et al. (2014), Stefanis et al. (2006), van der Werf et al. (2011), and van der Werf et al. (2007) indicates more frequent associations between HL and psychotic disorders in younger populations compared to older ones, potentially leading to incidents of violence.
The study's findings indicate that the risk of falls is elevated in younger and older adults with HL. Specifically, for older adults, age-related hearing impairment not only impacts communication and quality of life but is also associated with accelerated cognitive decline and an increased incidence of all-cause dementia (Brown et al., 2018; A. Davis et al., 2016; Deal et al., 2017). Hearing impairment in adults over 65 years may serve as an indicator of cognitive dysfunction (Gurgel et al., 2014). The combined effects of age-related sensory and cognitive changes necessitate older adults to exert more effort to maintain balance during daily activities (Gopinath et al., 2016). Therefore, further research into the role of dementia as a potential mechanistic link in the association between HL and falls is justified. (Powell et al., 2021)
Excessive exposure to noise, resulting in noise-induced hearing loss (NIHL), ranks as the second most common cause of acquired HL, following the natural aging process. (Carroll et al., 2017) Young individuals are often exposed to extended periods of unsafe sound levels due to activities such as music-related hobbies, noise pollution, and workplace noise. A systematic review by Jiang et al. (2016) showed that up to 58.2% of adolescents and young adults are exposed to daily noise levels exceeding the recommended maximum. Although a population-based cohort study by Girard et al. (2014) indicated an increased risk of hospitalization due to falls as the severity of NIHL increased among retired workers, the association between NIHL and fall risk in young adults remains underinvestigated.
Soylemez and Mujdeci (2020) found that patients with more severe NIHL exhibited more abnormal vestibular test results and more significant impairment in dual-task performance. Since dual-task performance may indicate fall risk (Wollesen et al., 2018), these findings suggest that individuals with NIHL might be at an increased risk of falling. Like age-related HL, NIHL is irreversible, but unlike age-related HL, it is preventable or can be minimized. Addressing NIHL, which may augment fall risk, requires preventive measures. These measures include reducing the intensity and duration of environmental noise, using ear protectors, and promoting early detection of NIHL (Sulkowski et al., 2017; Świerczek et al., 2020).
The results of our study suggest that individuals with cataracts or those who have undergone lens operations do not face a significantly higher risk of unintentional injury compared to those with HL alone. A key consideration is that individuals who undergo lens operations may not fully represent those with significant visual impairment, as their vision is likely corrected, potentially lowering the observed injury risk. While individuals with multiple sensory impairments may encounter unique challenges that could compromise their safety and quality of life, this suggests that our study may not accurately reflect the risks faced by individuals with uncorrected dual sensory loss, emphasizing the need for further investigation into the injury risks associated with uncorrected sensory impairments.
This study possesses several strengths. Firstly, while numerous studies have focused on the correlation between older individuals with HL and fall risk, this research encompassed older and younger adults. The findings reveal that HL is a risk factor for unintentional injuries, independent of age considerations. Therefore, addressing disabling hearing conditions assists in enhancing the quality of life for individuals with early-onset or congenital HL. Secondly, while most studies in this field have relied on subjective assessments of HL through questionnaires or interviews, this study employed diagnoses made by specialists using validated diagnostic codes. This approach effectively mitigated recall bias and facilitated a more objective confirmation of HL. Finally, the analysis of different injury subtypes, with adjustments for comorbidities, provided a more comprehensive understanding of the mechanisms underlying injuries associated with HL. This comprehensive approach established a definitive relationship between HL and subtypes of unintentional injuries, expanding beyond the scope of many studies that have primarily focused on falls or fall-related incidents.
This study is subject to certain limitations. Firstly, the NHI research database did not provide detailed medical records regarding the specific etiologies and severities of HL among participants. Variations in the causes of hearing impairment might significantly impact the incidence and subtype of subsequent injuries. Future research should include comprehensive audiological assessment results to better understand the relationship between the characteristics of HL and the risk of subsequent injuries. Additionally, the database lacked information on potential residual confounding factors such as genetic, physical, psychological, behavioral, and socioenvironmental variables that could be associated with different types of injuries. While we excluded patients with vertigo-related diagnoses, it lacks vestibular data for the HL group. Individuals with HL might experience compromised vestibular function, potentially increasing their risk of falls and related injuries. Furthermore, since there is no information about objective audiological testing of study groups, we cannot assess the severity of HL and its impact on the risk of injury. Thirdly, the reliance on diagnostic codes presented challenges in evaluating the impact of post-diagnosis management, including hearing aids or participation in hearing rehabilitation programs for individuals with HL. The inability to assess treatment outcomes and verify whether patients received appropriate treatment resulted in an incomplete understanding of the effectiveness of interventions in reducing injury risk. Despite these limitations, this population-based cohort study established that HL significantly increased the risk of injury by 2.35 times over an average follow-up period of 9.08 years. Therefore, physicians must advise adult patients with HL on preventive measures against subsequent injuries.
Conclusions
In conclusion, this study provides population-based evidence that adults of all age groups with HL are at an increased risk of sustaining subsequent injuries compared to those without HL. Healthcare providers should consider HL as a potential risk factor for injuries and provide appropriate interventions to reduce the risk. This study emphasizes the need for further research to explore the underlying mechanisms linking HL and injury risk and to develop effective interventions to mitigate this risk. Overall, this study highlights the importance of addressing HL as a public health concern and underscores the need for increased awareness and advocacy for hearing health.
Supplemental Material
sj-doc-1-tia-10.1177_23312165241309589 - Supplemental material for Association of Increased Risk of Injury in Adults With Hearing Loss: A Population-Based Cohort Study
Supplemental material, sj-doc-1-tia-10.1177_23312165241309589 for Association of Increased Risk of Injury in Adults With Hearing Loss: A Population-Based Cohort Study by Kuan-Yu Lai, Hung-Che Lin, Wan-Ting Shih, Wu-Chien Chien, Chi-Hsiang Chung, Mingchih Chen, Jeng-Wen Chen and Hung-Chun Chung in Trends in Hearing
Footnotes
Acknowledgments
The authors are grateful for the administrative assistance on this project provided by Chiu-Ping Wang, Shu-Hwei Fan, Wei-Chun Chen, Uan-Shr Jan, and Wan-Ning Luo. They received no additional compensation for their contributions. They also appreciate the Health and Welfare Data Science Center, Ministry of Health and Welfare, Taiwan, for providing the National Health Insurance Research Database. This manuscript was edited by Wallace Academic Editing.
Author Contributions
Jeng-Wen Chen and Hung-Chun Chung had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis.
Kuan-Yu Lai: Study concept and design, Interpretation of data, Drafting of the manuscript, Critical revision of the manuscript for important intellectual content.
Hung-Che Lin: Study concept and design, Acquisition and analysis of data, Interpretation of data, and technical support.
Wan-Ting Shih: Study concept and design, Interpretation of data, Critical revision of the manuscript for important intellectual content.
Wu-Chien Chien: Study concept and design, Acquisition and analysis of data, Interpretation of data, and technical support.
Chi-Hsiang Chung: Acquisition and analysis of data, Interpretation of data, and technical support.
Mingchih Chen: Critical revision of the manuscript for important intellectual content, Administrative, technical, or material support.
Jeng-Wen Chen: Study concept and design, Interpretation of data, Critical revision of the manuscript for important intellectual content, Obtained funding, Administrative, technical, or material support.
Hung-Chun Chung: Study concept and design, Interpretation of data, Critical revision of the manuscript for important intellectual content.
Hung-Che Lin disclosed no relevant relationships.
Wan-Ting Shih disclosed no relevant relationships.
Wu-Chien Chien disclosed no relevant relationships.
Chi-Hsiang Chung disclosed no relevant relationships.
Mingchih Chen disclosed no relevant relationships.
Jeng-Wen Chen disclosed no relevant relationships.
Hung-Chun Chung disclosed no relevant relationships.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Science and Technology Council of the Republic of China (Taiwan) under grant NSTC 110-2511-H-567-001-MY2, NSTC 112-2410-H-567-001-MY3 and, in part, funded by Cardinal Tien Hospital under grant CTH112A-2218 and Cardinal Tien Junior College of Healthcare and Management under grant CTCN-109C-09. This study was also supported by the Tri-Service General Hospital Research Foundation (TSGH-B-113025). We also appreciate the Health and Welfare Data Science Center, Ministry of Health and Welfare (HWDC, MOHW), Taiwan, for providing the National Health Insurance Research Database(NHIRD).
Role of the Funder/Sponsor
The funders had no role in the design and conduct of the study; data collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
Data Availability Statement
Share upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.