
Abstract
This study presents a comprehensive analysis of global, regional, and national trends in the burden of hearing loss (HL) among children and adolescents from 1990 to 2019, using data from the Global Burden of Disease study. Over this period, there was a general decline in HL prevalence and years lived with disability (YLDs) globally, with average annual percentage changes (AAPCs) of −0.03% (95% uncertainty interval [UI], −0.04% to −0.01%; p = 0.001) and −0.23% (95% UI, −0.25% to −0.20%; p < 0.001). Males exhibited higher rates of HL prevalence and YLDs than females. Mild and moderate HL were the most common categories across all age groups, but the highest proportion of YLDs was associated with profound HL [22.23% (95% UI, 8.63%−57.53%)]. Among females aged 15−19 years, the prevalence and YLD rates for moderate HL rose, with AAPCs of 0.14% (95% UI, 0.06%−0.22%; p = 0.001) and 0.13% (95% UI, 0.08%−0.18%; p < 0.001). This increase is primarily attributed to age-related and other HL (such as environmental, lifestyle factors, and occupational noise exposure) and otitis media, highlighting the need for targeted research and interventions for this demographic. Southeast Asia and Western Sub-Saharan Africa bore the heaviest HL burden, while High-income North America showed lower HL prevalence and YLD rates but a slight increasing trend in recent years, with AAPCs of 0.13% (95% UI, 0.1%−0.16%; p < 0.001) and 0.08% (95% UI, 0.04% to 0.12%; p < 0.001). Additionally, the analysis revealed a significant negative correlation between sociodemographic index (SDI) and both HL prevalence (r = −0.74; p < 0.001) and YLD (r = −0.76; p < 0.001) rates. However, the changes in HL trends were not significantly correlated with SDI, suggesting that factors beyond economic development, such as policies and cultural practices, also affect HL. Despite the overall optimistic trend, this study emphasizes the continued need to focus on specific high-risk groups and regions to further reduce the HL burden and enhance the quality of life for affected children and adolescents.
Keywords
Introduction
Hearing loss (HL) poses a serious public health issue among children and adolescents globally. According to a 2024 report by the World Health Organization (WHO), approximately 430 million individuals worldwide suffer from HL, accounting for over 5% of the global population, and are categorized as needing rehabilitation due to disability (World Health Organization, 2024). Of these, approximately 34 million are children, predominantly located in economically weaker regions. Optimal hearing is crucial for the development of language skills and social competencies in children and adolescents. Optimal hearing is crucial for the development of spoken language skills and can significantly impact the social functioning, cognitive abilities, and quality of life of children and adolescents (Lieu et al., 2020). Compared to their peers with normal hearing, children with hearing impairments have twice the risk of psychosocial problems (de Jong et al., 2023). Furthermore, these children are less likely to receive formal education (Olusanya & Newton, 2007), and as adults, those with HL are more prone to unemployment and earn significantly less than their hearing counterparts (Jung & Bhattacharyya, 2012). Timely diagnosis and appropriate interventions can significantly improve conditions for these children. According to the WHO's report (World Health Organization, 2024), preventative measures can reduce HL for children by approximately 60%. Therefore, implementing suitable preventative measures, including vaccination, good maternal and child health practices, genetic counseling, and managing common ear diseases, are effective strategies to reduce HL for children.
In collaboration with the Global Burden of Disease (GBD) study (Global Burden of Disease Collaborative Network, 2020), we obtained data from 1990 to 2019, which provide a detailed and comprehensive overview of the global burden of HL for children and adolescents. Previous studies have provided prevalence and incidence data for HL among children and adolescents in specific regions (Birhanu et al., 2021; Emmett et al., 2023; Jensen et al., 2021) and countries (Barrett & White, 2017; Feder et al., 2017; Schmucker et al., 2019). According to the second national survey of disabled persons conducted in China in 2006, approximately 17.5 per 10,000 children aged 0−17 years had HL, with approximately 64.6% of these cases being preventable or treatable. The primary causes were genetic factors, otitis media, and drug toxicity (Yun et al., 2017). In the United States, a retrospective analysis of 7036 adolescents aged 12−19 years from the National Health and Nutrition Examination Survey (NHANES) data (National Center for Health Statistics, n.d.) spanning 1988−2010 found that the prevalence increased from 17.0% in NHANES III (1988–1994) to 22.5% in NHANES 2007−2008, but then decreased to 15.2% in NHANES 2009−2010 (Su & Chan, 2017). A recent study using GBD 2019 data (Global Burden of Disease Collaborative Network, 2020) analyzed the burden of complete HL caused by congenital birth defects for children under 5 from 1990 to 2030. It found a global prevalence of 15.4 per 100,000 population (95% UI, 5.8−33.8) in 2019, with a YLD rate of 3.3 per 100,000 (95% UI, 1.1−7.1). Using autoregressive integrated moving average and Bayesian age-period-cohort models, the study predicted a decline in prevalence by 2030. These models incorporated historical data and accounted for statistical uncertainties, assuming better prevention of infectious etiologies, improvements in genetic diagnoses, and advancements in hearing restoration methods. This emphasizes the importance of enhancing preventive, diagnostic, and treatment measures (Xiao et al., 2023). There is a lack of global trend data on the burden of HL of various severities caused by different causes among children and adolescents, broken down by age and sex, as well as a lack of national-level reports on the relationship between the HL burden and the sociodemographic index (SDI).
This study aimed to analyze the HL prevalence and YLD rates among children and adolescents at the global, regional, and national levels from 1990 to 2019, as well as their trends. By breaking down the data by age, sex, severity, and causes, and examining the impact of SDI at regional and national levels, this study provides a scientific basis for devising targeted intervention measures and related policies.
Methods
Overview
This study used the results of the GBD 2019 (Global Burden of Disease Collaborative Network, 2020), which provided estimates of the prevalence of HL and the use of hearing aids globally. The GBD study conducted a comprehensive and systematic assessment and analysis of 369 diseases and injuries, including HL, along with their related causes across 21 GBD study regions and 204 countries and territories during the period from 1990 to 2019. The methods have been detailed previously (GBD, 2019 Diseases and Injuries Collaborators, 2020) and are presented in Supplemental Data 1. This study adhered to the guidelines for accurate and transparent health estimate reporting (World Health Organization, 2023).
Case Definition and Data Collection
HL can affect one or both ears and range from mild to complete deafness. The GBD study defines hearing impairment as an HL >20 decibels (dB) in the ear with better hearing, based on the average across 500, 1000, 2000, and 4000 Hz (Institute for Health Metrics and Evaluation, 2021a). This definition is consistent with the WHO's definition of HL (World Health Organization, 2024). The GBD study classified HL into six severities: mild HL (20–34 dB), moderate (35–49 dB), moderately severe (50–64 dB), severe (65–79 dB), profound (80–94 dB), and complete HL (>95 dB) (GBD, 2019 Hearing Loss Collaborators, 2021). In addition, two health states were assigned to each severity level based on the presence or absence of tinnitus, a ringing or buzzing sound in the ears that often accompanies HL. Health states describe the subjective experience and functional limitations of patients at different levels of HL. Disability weights quantify the burden of these health states on a scale from 0 (completely healthy) to 1 (equivalent to death). Detailed descriptions of these health states and their corresponding disability weights are provided in Supplemental Table S1 (GBD, 2019 Hearing Loss Collaborators, 2021). A summary of the data and methods is provided in Supplemental Data 2.
This study focused on individuals aged 0–19 years, divided into four age groups (0–4, 5–9, 10–14, and 15–19 years). Each individual was assigned to one of 21 regions based on geographical and epidemiological similarities according to the GBD project's guidelines. The GBD 2019 provided each country's SDI, a composite indicator designed to quantify the socioeconomic development of a country or region. The SDI is the geometric mean of per-capita income, education level, and fertility rate after each has been scaled to range from 0 to 1. The SDI ranges from 0 to 1, where 0 indicates the lowest socioeconomic development level and 1 the highest.
In this study, to comprehensively and thoroughly understand and analyze the different causes of HL, we selected the level 3 causes of HL, including age-related and other HL, congenital birth defects, meningitis, and otitis media. Age-related and other HL includes all non-meningitis, non-chronic otitis media, and non-congenital causes of HL (Institute for Health Metrics and Evaluation, 2021b). Since our study focuses on HL in children and adolescents aged 0–19 years, in our study, age-related and other HL mainly refers to HL caused by environmental factors, lifestyle factors, and occupational noise exposure, rather than presbycusis, which is HL caused by aging and primarily due to the loss of sensory cells in the inner ear, especially hair cells (Wu et al., 2020).
Data Processing and Disease Model
This study extracted the prevalence of each category of HL and YLD data. Prevalence was defined as the number of individuals with a specific degree of HL, either as an absolute number or a percentage of the total population. To estimate the effect of non-fatal conditions, the GBD study used YLDs to quantify the associated disability by multiplying the severity-specific prevalence of a disease by a corresponding disability weight. They were obtained from a series of global surveys through pairwise comparisons of the severity of different health states (Salomon et al., 2015) and converted into disability weights through probit regression analysis.
Global patterns of HL prevalence and YLD rates were analyzed across different age categories, with their average annual percentage changes (AAPCs) determined through linear regression, where the log-transformed rate served as the dependent variable and the year as the independent variable. For example, an AAPC of 0.1 indicates a 0.1% annual growth rate.
To understand the data's trend over time, we used joinpoint regression analysis to construct the simplest model of the data by connecting multiple line segments (the so-called joinpoints) on a logarithmic scale. This method allowed us to start with the simplest model (i.e., a straight line with no joinpoints) and validate each new point using the Monte Carlo permutation method by adding more joinpoints. The analysis was conducted using Joinpoint software provided by the National Cancer Institute and Information Management Services. We selected the final model using the weighted Bayesian information criterion. Statistical computations were conducted utilizing GraphPad Prism (version 9.5.1), RStudio software (version 2023.12.0), and the Joinpoint Regression Program (version 5.0.2). A p-value <0.05 was considered to be statistically significant.
Results
Global Burden Trends by Sex and Age
Table 1 presents the trends in HL prevalence and YLDs (per 100,000 population) for all age groups. Globally, there was a decrease in both the prevalence and YLD rates of HL from 1990 to 2019, with AAPCs of −0.03% (95% UI, −0.04% to −0.01%; p = 0.001) and −0.23% (95% UI, −0.25% to −0.20%; p < 0.001), respectively. Joinpoint regression analysis revealed that HL prevalence gradually increased to a peak from 1993 to 2000 (APC = 0.22%; p < 0.001), the highest recorded prevalence over 30 years [Figure 1(A)]. From 2000 to 2009, HL prevalence declined significantly (APC = −0.23%; p < 0.001), then remained relatively stable until there was a slight increase in 2015 (APC = 0.08%; p < 0.001). As shown in Figure 1(B), apart from a slight increase from 1993 to 2001 (APC = 0.05%; p = 0.001), the HL prevalence and YLD rates showed a declining trend from 1990 to 2019, especially from 2004 to 2014 (APC = −0.36%; p < 0.001).

Joinpoint regression analysis shows the global prevalence (A) and YLD (B) rates of HL among children and adolescents from 1990 to 2019. APC = annual percentage change; YLD = years lived with disability. *p < 0.001.
Prevalence Rates and Years Lived with Disability Attributable to Hearing Loss and Their Average Annual Percentage Changes from 1990 to 2019 at the Global and Regional Levels
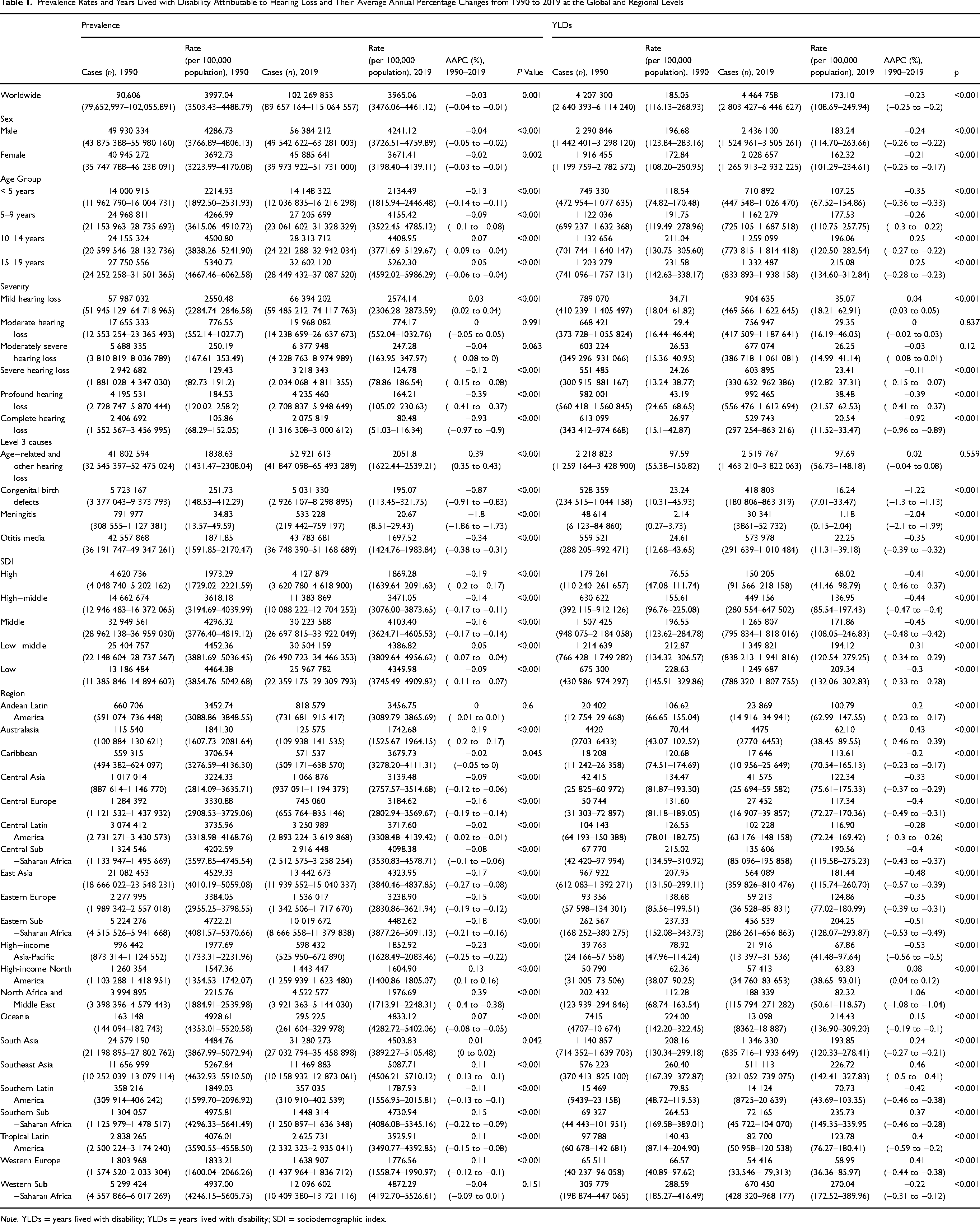
Note. YLDs = years lived with disability; YLDs = years lived with disability; SDI = sociodemographic index.
The global HL prevalence and YLD rates were greater for males than for females. The HL prevalence for both males and females declined from 1990 to 2019, with AAPCs of −0.04% (95% UI, −0.05% to −0.02%; p < 0.001) and −0.02% (95% UI, −0.03% to −0.01%; p = 0.002), respectively. YLD rates showed a significant decline for both males and females, with AAPCs of −0.24% (95% UI, −0.26% to −0.22%, p < 0.001) and −0.21% (95% UI, −0.25% to −0.17%; p < 0.001), respectively. From 1990 to 2019, the global HL prevalence and YLD rates exhibited a significant downward trend across all age groups. Specifically, the prevalence rates for the age groups <5 years, 5–9 years, 10–14 years, and 15–19 years declined with AAPCs of −0.13%, −0.09%, −0.07%, and −0.05%, respectively. YLD rates for these age groups also declined with AAPCs of −0.35%, −0.26%, −0.25%, and −0.25%, respectively.
Global Burden Trends by Severity and Cause
In 2019, 102.3 million children and adolescents globally were diagnosed with HL, with cases of mild and moderate HL accounting for 64.9% (95% UI, 51.7%−82.7%) and 19.5% (95% UI, 12.4%−29.7%), respectively (Figure 2(A) and Table 1). In the same year, of the 4.47 million YLDs attributed to HL, 22.2% (95% UI, 8.6%−57.5%) were due to profound HL, which represented the highest proportion of YLDs among the categories (Figure 2(A) and Table 1). Between 1990 and 2019, the prevalence and YLD rates for mild HL exhibited a slight upward trend, with AAPCs of 0.03% (95% UI, 0.02%−0.04%; p < 0.001) and 0.04% (95% UI, 0.03%−0.05%; p < 0.001), respectively (Table 1). In contrast, the prevalence and YLD rates for complete HL showed significant declines, with AAPCs of −0.93% (95% UI, −0.97% to −0.90%; p < 0.001) and −0.92% (95% UI, −0.96% to −0.89%; p < 0.001) (Table 1).

Global HL trends among children and adolescents by age and severity levels in 2019. (A) Prevalence of HL and YLDs by severity level. (B) Prevalence of HL by age and severity. (C) YLD rates by age and severity level. YLD = years lived with disability.
In 2019, mild HL had the highest prevalence across all age groups (Figure 2(B) and Table 2). With the exception of severe HL, the HL prevalence of varying severities increased with age, particularly among adolescents aged 15−19 years, where it was significantly higher than for children under 5 years of age (Figure 2(B)). As age increased, the YLD rates for all severities of HL, except for severe HL, also increased, especially in adolescents aged 15−19 years. The YLD rates attributable to mild, moderate, moderately severe, profound, and complete HL were significantly greater for adolescents aged 15−19 years than for children under 5 years of age (Figure 2(C)). Additionally, among different age groups, the proportion of YLDs caused by profound HL cases was the highest. Specifically, the proportions for the age groups <5 years, 5–9 years, 10–14 years, and 15–19 years were 21.4%, 22.1%, 23.0%, and 22.1%, respectively (Supplemental Figure S1).
Prevalence Rates and Years Lived with Disability Attributable to Hearing Loss and Their Average Annual Percentage Changes from 1990 to 2019 by Severity at the Global Level
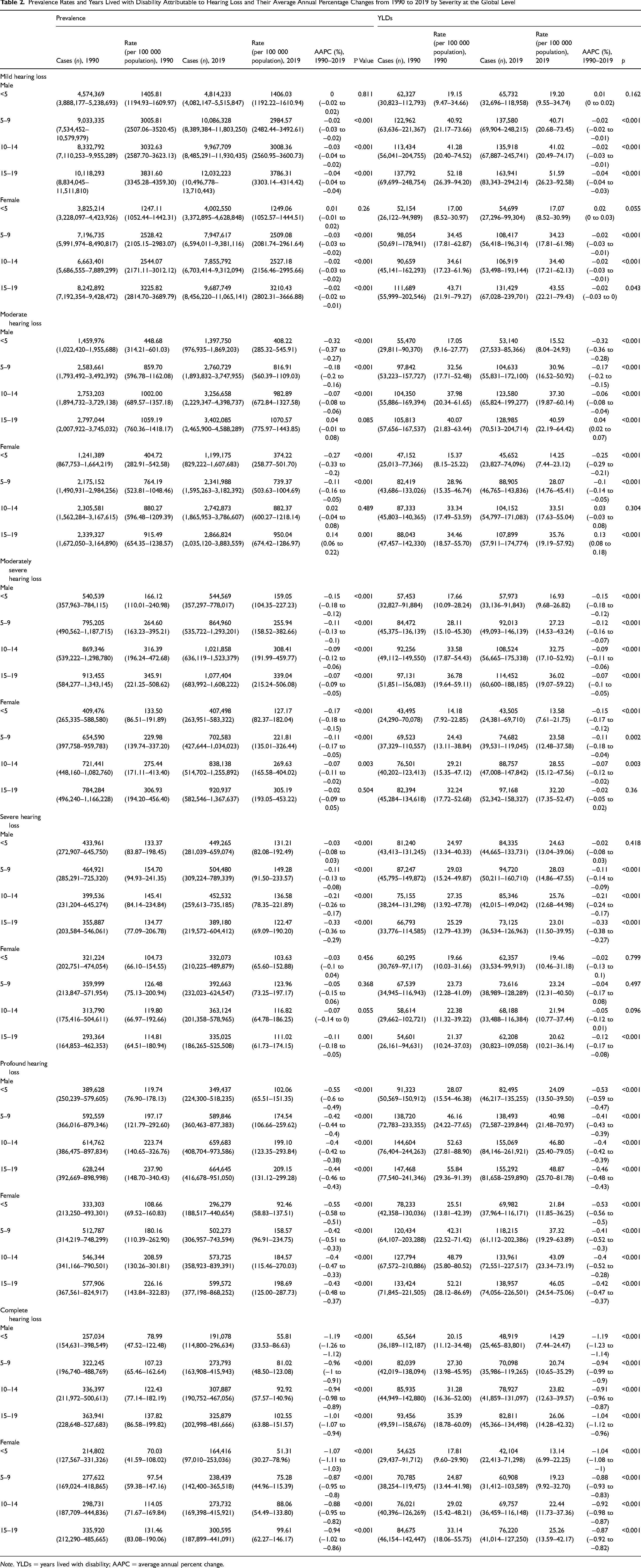
Note. YLDs = years lived with disability; AAPC = average annual percent change.
Between 1990 and 2019, the global prevalence of age-related and other HL demonstrated an upward trend, with AAPCs of 0.39% (95% UI, 0.35%−0.43%; p < 0.001). In contrast, the prevalence and YLD rates for HL caused by congenital disabilities, meningitis, and otitis media all showed a downward trend (Table 1). There was a significant decrease in the prevalence and YLD rates of HL caused by meningitis, with AAPCs of −1.8% (95% UI, −1.86% to −1.73%; p < 0.001) and −2.04% (95% UI, −2.1% to −1.99%; p < 0.001), respectively (Table 1). The YLD rate attributed to congenital disabilities also showed a significant decrease, with an AAPC of −1.22% (95% UI, −1.3% to −1.13%; p < 0.001) (Table 1).
The prevalence and YLD rates for HL of various severities for both males and females across different age groups generally showed a declining trend. However, for females aged 15−19 years, the prevalence and YLD rates for moderate HL showed an upward trend, with AAPCs of 0.14% (95% UI, 0.06%−0.22%; p = 0.001) and 0.13% (95% UI, 0.08%−0.18%; p < 0.001), respectively (Table 2). For males of the same age group, the YLD rates for moderate HL also showed a slight upward trend, with AAPC of 0.04% (95% UI, 0.02%−0.07%; p < 0.001) (Table 2). Figure 3 illustrates the prevalence and YLD rates for HL of various severities due to different causes among children and adolescents of different age and sex groups globally in 2019. For moderate HL, females aged 15–19 years exhibited higher prevalence and YLD rates compared to those in the <5 years, 5–9 years, and 10–14 years age groups, with age-related and other HL as the primary cause. Specifically, the prevalence and YLD rates attributable to age-related and other HL for females in this age group were 616.6 and 16.3 per 100,000 population, respectively (Figure 3(B)). This indicates that despite being a relatively young age group, HL resulting from age progression, genetic factors, or early exposure to high noise levels should not be ignored. Otitis media also played a significant role in causing moderate HL for this age group of females. The contributions of congenital disabilities and meningitis to moderate HL for females aged 15–19 years were relatively lower compared to age-related and other HL as well as otitis media (Figure 3(B)).

Global trends in the severity of HL due to different causes among children and adolescents by age and sex in 2019. (A) Mild HL. (B) Moderate HL. (C) Moderately severe HL. (D) Severe HL. (E) Profound HL. (F) complete HL. YLD = years lived with disability.
Burden Trends by Region and Nation
The HL prevalence and YLD rates for children and adolescents declined globally from 1990 to 2019 in most regions (Table 1) and countries (Supplemental Table S2). As shown in Table 1, Southeast Asia had the highest prevalence in 1990 and 2019 (5268 and 5088 per 100,000 population, respectively). Western sub-Saharan Africa had the highest YLD rates in 1990 and 2019 (289 and 270 per 100,000 population, respectively). High-income North America had the lowest prevalence (1547 and 1605 per 100,000 population, respectively) and YLD rates (62.4 and 63.8 per 100,000 population, respectively) in 1990 and 2019 among the 21 GBD regions; however, both the prevalence and YLD rates showed an increasing trend from 1990 to 2019, with AAPCs of 0.13% (95% UI, 0.1%−0.16%; p < 0.001) and 0.08% (95% UI, 0.04%−0.12%; p < 0.001), respectively.
In 2019, Myanmar, Madagascar, and Kenya were the countries with the highest prevalence (5633, 5357, and 5626 per 100,000 population, respectively) (Figure 4(A) and Supplemental Table S2). The three countries with the highest YLD rates were Nigeria, Madagascar, and Myanmar (322, 297, and 297 per 100,000 population, respectively) (Figure 4(B) and Supplemental Table S2). Finland had the lowest prevalence and YLD rates (1302 and 41 per 100,000 population, respectively) in 2019 among the 204 countries (Figure 4(A) and 4(B), Supplemental Table S2). From 1990 to 2019, the prevalence decreased in 152 countries, with the largest declines observed in Oman (AAPC = −0.57%; p < 0.001), the Islamic Republic of Iran (AAPC = −0.52%; p < 0.001), and Saudi Arabia (AAPC = −0.5%; p < 0.001). The United Kingdom (AAPC = 0.19%; p < 0.001), the Democratic People's Republic of Korea (AAPC = 0.21%; p < 0.001), and the Northern Mariana Islands (AAPC = 0.34%; p < 0.001) showed significant increasing trends in HL prevalence (Figure 4(C) and Supplemental Table S2). The countries with the largest decreases in YLD rates were Saudi Arabia (AAPC = −1.59%; p < 0.001), Oman (AAPC = −1.5%; p < 0.001), and the Islamic Republic of Iran (AAPC = −1.25%; p < 0.001). Kiribati (AAPC = 0.07%; p = 0.005), the USA (AAPC = 0.11%; p < 0.001), and the Northern Mariana Islands (AAPC = 0.26%; p < 0.001) showed increasing trends in HL prevalence and YLD rates (Figure 4(D) and Supplemental Table S2).

Global maps show prevalence (A) and YLD (B) rates for HL among children and adolescents in 2019 and AAPCs in prevalence (C) and YLD (D) from 1990 to 2019. YLD = years lived with disability; AAPCs = average annual percentage changes.
Relation of Prevalence and YLD Rates to SDI
From 1990 to 2019, the HL prevalence rates declined across all SDI groups, with AAPCs of −0.19%, −0.14%, −0.16%, −0.05%, and −0.09% for the high, high-middle, middle, low-middle, and low SDI groups, respectively. YLD rates also showed a significant downward trend, with AAPCs of −0.41%, −0.44%, −0.45%, −0.31%, and −0.3% for these respective groups (Table 1). From 1990 to 2019, there were significant negative correlations between SDI and HL prevalence (r = −0.74; p < 0.001) and YLD (r = −0.76; p < 0.001) rates across regions (Figure 5(A) and 5(B)). In 2019, there were significant negative correlations between SDI and the HL prevalence (r = −0.63; p < 0.001) and YLD (r = −0.73; p < 0.001) rates across nations (Figure 5(C) and 5(D)). From 1990 to 2019, AAPCs of HL prevalence and YLD rates in most countries were negative (Figure 5(E) and 5(F) and Supplementary Table 2). However, the changes in HL prevalence (r = −0.11; p = 0.112) and YLD (r = −0.07; p = 0.287) rates were not correlated with the SDI (Figure 5(E) and 5(F)). This suggests that while countries with higher SDI values tend to have lower growth rates of HL prevalence and YLDs for children and adolescents, this trend is neither uniform nor significant.

Trends in HL prevalence and YLD among children and adolescents from 1990 to 2019 in relation to SDI. (A) Prevalence rates in 21 GBD study regions (1990–2019). (B) YLD rates in 21 GBD study regions (1990–2019). (C) Prevalence rates in 204 countries and territories (2019). (D) YLD rates in 204 countries and territories (2019). (E) AAPCs in prevalence for 204 countries and territories from 1990 to 2019. (F) AAPCs in YLD for 204 countries and territories from 1990 to 2019. YLD = years lived with disability; GBD = Global Burden of Disease study 2019; SDI = sociodemographic index; AAPCs = average annual percentage changes.
Discussion
To our knowledge, this study is the first to comprehensively consider the effect of age, sex, severity, cause, and SDI, providing a detailed description of HL prevalence and YLD rates among children and adolescents (aged 0–19) globally, regionally, and nationally from 1990 to 2019. Over the past three decades, the global burden of HL among children and adolescents has generally shown a downward trend, reflecting improvements in preventive measures and treatment methods. However, the increasing prevalence of HL attributable to age-related and other HL, as well as the disparities at different sex and region levels, require ongoing monitoring and intervention. Our analysis indicated that there are significant negative correlations between SDI and HL prevalence and YLD rates at both the regional and national levels. Nonetheless, the variations in HL trends across countries did not exhibit a significant linear relationship with SDI, suggesting that other factors influence the progression of HL. These findings provide crucial evidence for formulating future HL intervention strategies targeted at different ages, sexes, regions, and countries. For example, interventions for younger children (0–5 years) can focus on prevention and early diagnosis, while interventions for adolescents (15–19 years) can prioritize reducing noise exposure and increasing awareness of hearing protection. Strategies tailored to different genders can meet the unique needs of males and females, such as providing more community hearing screening programs for female adolescents to promote early detection and intervention. Strategies at regional and national levels can be adjusted according to the varying HL burdens in different areas. In low-income regions and countries, it is essential to consider the impact of socioeconomic factors on HL and address health disparities through strategies such as improving education, healthcare services, and public health awareness. Lastly, the lack of a significant linear relationship between SDI and changes in HL trends indicates that other factors also influence the progression of HL. Therefore, future strategies should consider a comprehensive approach that includes genetic, environmental, and lifestyle factors to develop holistic intervention plans.
Globally, in 2019, approximately 102 million children and adolescents were affected by HL, resulting in approximately 4.47 million YLDs. Compared to 1990, the prevalence and YLD rates in 2019 decreased, with AAPCs of −0.03% and −0.23% respectively. Our findings align with previous analyses of the burden of congenital profound HL in children under 5 years of age from 1990 to 2019 (Xiao et al., 2023). Over the past 30 years, HL prevalence and YLD rates among children and adolescents have shown fluctuating trends, with an increase to a peak between 1993 and 2000, possibly reflecting an increase in risk factors or a lack of public health interventions. The significant decline in HL prevalence and YLDs from 2000 to 2009 suggests that effective prevention and intervention measures may have been implemented. The significant decline in HL prevalence and YLDs from 2000 to 2009 suggests that effective prevention and intervention measures may have been implemented. For example, WHO established World Hearing Day in 2007, held annually on March 3rd, to promote HL prevention and improve hearing care (World Health Organization, 2020). In 1999, the Global Alliance for Vaccines and Immunization was founded to overcome barriers preventing millions of children from receiving vaccines, eliminate childhood diseases, and improve global health (World Health Organization, 1999). The alliance's initiatives indirectly reduce the prevalence of HL, as vaccines that prevent meningitis and measles help reduce HL caused by these diseases. A 2001 WHO conference in Geneva discussed establishing public-private partnerships to drastically reduce the cost of hearing aids to $10−$20 and issued new guidelines for hearing aids and services in developing countries, addressing cost, service, and training issues (World Health Organization, 2001). Although hearing aids themselves may not directly lead to a reduction in the prevalence of HL, they could significantly decrease YLD rates by improving the management of HL and reducing the burden of long-term disability. However, a slight increase in prevalence since 2015 suggests emerging challenges. Several hypotheses can explain this trend, including increased environmental noise exposure (Balk et al., 2023) and advancements in genetic screening technology significantly improving early detection and diagnosis of HL (Korver et al., 2017). This emphasizes the importance of continuous monitoring and adaptive interventions to maintain and enhance public hearing health.
From 1990 to 2019, the overall HL prevalence and YLD rates among children and adolescents globally showed a declining trend. The rates were higher for males than females, with a smaller decrease for males, consistent with previous studies on sex differences in HL (Villavisanis et al., 2018; Villavisanis et al., 2020). This phenomenon may be related to biological differences (Azcoitia et al., 2019; Maurizi et al., 1988; Nolan, 2020; Shuster et al., 2019; Williamson et al., 2020), behavioral and sociocultural factors, and environmental exposures (Bhatt et al., 2020; Reavis et al., 2023; Wang et al., 2021; Warner-Czyz & Cain, 2016). Males are more susceptible to severe and early-onset HL, and this sex difference remains significant even after excluding factors such as noise exposure (Nolan, 2020). In a study on the effects of sex on auditory brainstem responses (ABR) in infancy and early childhood, Maurizi et al. (Maurizi et al., 1988) found significant differences in the latency of ABR waves III and V and the III–V and I–V intervals between genders. This study, which involved 171 full-term normal children, revealed that girls had significantly shorter latencies for waves III and V and shorter III–V and I–V intervals than boys. These differences became more pronounced with age and were suggested to be associated with factors such as head size, brain size, and hormone-related neural conduction speed. The research indicates that sex differences in auditory function are evident even in infancy. Further supporting the important role of biological factors in the sex differences in HL, Meltser et al. (2008) found that Estrogen Receptor Beta (ERβ) significantly contributes to neuroprotection in the auditory system by upregulating brain-derived neurotrophic factor (BDNF) expression. ERβ is primarily located in the inner and outer hair cells and spiral ganglion neurons of the cochlea. Treatment with the selective ERβ agonist 2,3-Bis(4-Hydroxyphenyl)-Propionitrile markedly reduced auditory threshold shifts following acoustic trauma in mice. This indicates that ERβ plays a crucial role in regulating BDNF expression, which enhances neuronal survival and repair, protecting the auditory system from damage. Therefore, due to the more pronounced effect of ERβ in females, males are more susceptible to HL. Boys engage in high-risk noise activities about twice as often as girls, for example attending loud music events, using personal listening devices for longer periods or at higher volumes, and being more likely to work or be in noisy environments (Warner-Czyz & Cain, 2016). The HL prevalence and YLD rates for all severity levels of HL except severe increase with age, particularly among adolescents aged 15−19 years. This increase may be related to changes in the social environment during adolescence, such as the use of personal music players (PMPs) and exposure to video games (Harrison, 2012; Jiang et al., 2016; Lauren et al., 2024; Le Clercq et al., 2016; Twardella et al., 2017). Le Clercq et al. (2016) found that PMP users exhibit significantly poorer hearing thresholds and reduced otoacoustic emission distortion products after music exposure, along with a high incidence of tinnitus, suggesting a link between music exposure and early HL onset. WHO and the International Telecommunication Union jointly issued a new international standard in February 2019 aimed at making personal listening devices safer for hearing. This standard includes features such as “sound allowance” settings, personalized profiles, and volume control options (World Health Organization, 2019). WHO also launched the “Make Listening Safe” initiative to improve listening practices, especially among youths, when exposed to music and other sounds, and provided a practical guide to implementing global standards for safe listening devices (World Health Organization, 2022).
This study's findings indicate that in 2019 HL cases among children and adolescents globally were primarily mild and moderate, consistent with previous research (Ganek et al., 2023). Nassrallah et al. (2022) studied speech and language skills in children with unilateral and mild/moderate HL. The study included 238 children with HL up to 55 dB, and their outcomes were measured using three standardized tests. It was found that 25% of the children scored low in expressive communication and 28.3% scored low in articulation, especially those identified late and fitted with hearing aids late. The study highlights the importance of early identification and intervention. Although not as common as mild and moderate HL, profound HL accounted for the highest proportion of YLDs across all age groups, reflecting the severe cognitive dysfunctions and psychological issues it can cause, which significantly impact individual health and quality of life (Cejas et al., 2021; Xuan et al., 2018). Managing and mitigating the effects of profound HL requires specialized medical services and targeted interventions.
There was a slight upward trend in the prevalence of age-related and other HL from 1990 to 2019, with an AAPC of 0.39%. GBD database's “age-related and other HL” includes all non-meningitis, non-chronic otitis media, and non-congenital causes of HL (Institute for Health Metrics and Evaluation, 2021a). Given that our study focuses on HL for children and adolescents, in our study context, age-related and other HL primarily refers to HL caused by environmental factors, lifestyle factors, and occupational noise exposure rather than age-related degeneration. Conversely, HL caused by congenital disabilities, meningitis, and otitis media showed declining trends in both HL prevalence and YLD rates, with the decrease for meningitis being particularly significant. This positive change reflected improvements in global medical interventions, including early hearing screening and vaccinations against pneumococcus, Hib, and meningococcus (Ali et al., 2014). Additionally, preventing HL through vaccinations against measles, mumps, and rubella (MMR) was also crucial. According to Dudley et al. (2018), the MMR vaccine protected against HL by preventing natural infections such as measles and mumps that caused it. Therefore, the reduction in HL can also be attributed to the widespread use of these vaccines, further emphasizing the importance of comprehensive vaccination programs. However, there was an increase in HL prevalence and YLD rates of moderate HL among females aged 15−19 years, primarily due to age-related and other HL and otitis media, indicating that this age group may face specific risk factors, such as increased noise exposure and lifestyle changes. A study of Henderson et al. (2011), which involved hearing tests conducted on 4310 adolescents aged 12–19 years between NHANES III (1988–1994) and NHANES 2005–2006, demonstrated a significant increase in noise-induced hearing threshold shifts among adolescent females compared to the data from NHANES III (1988–1994). This underscores the need for protective and preventive measures for hearing in adolescent females and suggests that public health policies should focus more on this group, using education, community involvement, and health promotion activities to reduce the risk of HL.
From 1990 to 2019, we observed a general decline in HL prevalence among children and adolescents across most regions and countries. This trend reflects improvements in public health policies aimed at preventing HL, such as vaccination programs and better maternal and child health practices. However, there were significant disparities between regions and countries. For instance, Southeast Asia had high HL prevalence rates. In contrast, high-income North America had the lowest prevalence rates, although there has been a slight upward trend in recent years. This trend could be related to lifestyle changes (such as excessive use of electronic devices). Additionally, improvements in early detection and diagnostic technologies, including the use of low-cost otoacoustic emission probes based on smartphones, have led to more cases being identified and reported in a timely manner (Chan et al., 2022). Furthermore, HL YLD rates have also declined globally from 1990 to 2019. This decrease can be attributed to advances in medical technology and rehabilitation services, which have improved the quality of life for individuals with HL. Western Sub-Saharan Africa, however, still experiences high YLD rates, highlighting the need for improved access to hearing care and rehabilitation services in this region. Myanmar and Madagascar, the HL prevalence and YLD rates among children and adolescents are notably high, linked to deficiencies in the public health systems and medical resources of these developing countries. The Northern Mariana Islands showed a trend of increasing HL prevalence and YLD rates, suggesting a need for special attention to these areas and targeted interventions to mitigate the health burden of HL. There was a negative correlation between the SDI and both HL prevalence and YLD rates, consistent with the general trends observed in GBD studies. This may indicate that regions with higher SDI have more widespread health awareness and more effective public health interventions. However, the correlation between changes in HL prevalence and YLD rates among children and adolescents and SDI was not significant, suggesting that factors beyond economic development level, such as policies, cultural practices, and public health infrastructure, also significantly affect HL.
Limitations
This study had several limitations. First, our analysis was constrained by the quality and completeness of the GBD data, particularly for low and middle-income countries, where gaps and quality issues may have led to inaccurate estimates of the HL burden. Second, the GBD dataset lacked comprehensive information on certain key factors and specific etiologies affecting HL, such as genetic factors, environmental exposures, drug toxicity, and noise exposure, which limits our ability to fully understand the trends and determinants of HL. Third, our findings are based on data available up to 2019 and thus do not cover recent global changes, such as the potential impact of the COVID-19 pandemic on the burden of HL. Future research should focus on filling these data gaps and employing updated data to provide more accurate and comprehensive estimates of the global and regional burden of HL.
Conclusions
This study analyzed trends in the burden of HL among children and adolescents at global, regional, and national levels from 1990 to 2019. The global data revealed that the overall burden of HL declined. The HL prevalence and YLD rates were generally higher for males than for females. Mild and moderate HL were the most common categories across all age groups, but the highest proportion of YLDs was caused by profound HL. There was an increasing trend in the HL prevalence and YLD rates of moderate HL among females aged 15−19 years, primarily due to age-related and other HL and otitis media, underscoring the need for further research and attention to specific risk factors in this demographic. The burden of HL was high in Southeast Asia and Western Sub-Saharan Africa. High-income North America, despite having low prevalence and YLD rates, has experienced an upward trend in recent years, possibly related to lifestyle changes and improvements in early detection technologies. Moreover, there was a negative correlation between the SDI and both HL prevalence and YLD rates among children and adolescents. However, the relationship between HL trends and SDI was not significant, indicating that factors beyond economic development, such as policies and culture, also influence HL. Overall, although the global burden of HL among children and adolescents is decreasing, it remains crucial to focus on specific high-risk groups and regions where disparities persist. Future policies and health interventions should be more precisely targeted toward these groups and areas to further reduce the global burden of HL and enhance the quality of life for children and adolescents.
Supplemental Material
sj-docx-1-tia-10.1177_23312165241273391 - Supplemental material for Global, Regional, and National Burdens of Hearing Loss for Children and Adolescents from 1990 to 2019: A Trend Analysis
Supplemental material, sj-docx-1-tia-10.1177_23312165241273391 for Global, Regional, and National Burdens of Hearing Loss for Children and Adolescents from 1990 to 2019: A Trend Analysis by Kan Chen, Bo Yang, Xiaoyan Yue, HeMi, Jianjun Leng, Lujie Li, Haoyu Wang and Yaxin Lai in Trends in Hearing
Supplemental Material
sj-tif-2-tia-10.1177_23312165241273391 - Supplemental material for Global, Regional, and National Burdens of Hearing Loss for Children and Adolescents from 1990 to 2019: A Trend Analysis
Supplemental material, sj-tif-2-tia-10.1177_23312165241273391 for Global, Regional, and National Burdens of Hearing Loss for Children and Adolescents from 1990 to 2019: A Trend Analysis by Kan Chen, Bo Yang, Xiaoyan Yue, HeMi, Jianjun Leng, Lujie Li, Haoyu Wang and Yaxin Lai in Trends in Hearing
Footnotes
Acknowledgments
We would like to express our gratitude to the contributors of the GBD study. We also extend our heartfelt thanks to Professor Yongze Li from The First Affiliated Hospital of China Medical University for his guidance and support throughout this study. His expertise and insights have significantly contributed to the advancement of our work.
Data Availability
The data for this study originate from the GBD database, which is maintained by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington, providing data on the burden of diseases at global, regional, and national levels. The datasets involved in this study are publicly available through the official IHME website and consist of publicly released aggregated data without any personal identification information. Researchers can obtain and use these data in accordance with the IHME data use agreement. For researchers interested in the data from this study, we will provide detailed explanations of the data processing and analysis methods used in this research upon scientifically reasonable requests. Access requests for research data and related materials will be reviewed by the principal investigators and the collaborative team based on scientific merit. Upon approval, data will be shared through a secure online platform after the signing of a data access agreement.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.