
Abstract
Background:
To investigate the trends in Burkitt lymphoma incidence, mortality, and disability-adjusted life-years, considering sex and age, from 1990 to 2021, with a 20-year forecast.
Method:
Data regarding Burkitt lymphoma were extracted from the Global Burden of Disease study for the year 2021.
Results:
Globally, there were 19,072 incident cases of Burkitt lymphoma in 2021. Cases of Burkitt lymphoma experienced a 207% increase from 1990 to 2021. Over three decades, Burkitt lymphoma-associated deaths rose from 3843 to 6525. The global incidence rate of Burkitt lymphoma increased from 0.127 in 1990 to 0.236 in 2021 per 100,000 population. High body-mass indexes contribution to Burkitt lymphoma is evident in the disability-adjusted life-years, with the United States and the United Kingdom recording 0.06 and 0.05, respectively. Conversely, China and India demonstrated substantially lower contributions, at 0.02 and 0.005, respectively. The groups aged 0–14 and 50–74 years surpassed other age groups in both Burkitt lymphoma-associated incidence and death numbers. Moreover, males consistently had higher Burkitt lymphoma-associated mortality rates and numbers than females in all age groups. Furthermore, the estimated annual percentage changes of incidence with Burkitt lymphoma were positively correlated with sociodemographic index (Pearson r = 0.606; p = 0.003). The Bayesian age-period-cohort model predicts a significant increase in the age-standardized incidence rates of Burkitt lymphoma over the next 20 years. Interestingly, the age-standardized rates of death did not change dramatically from 1990 to 2021; and the trend is expected to remain relatively stable in the future 20 years.
Conclusion:
The burden of Burkitt lymphoma varies according to different regions and genders, and children of 0–14 years, adults of 50–74 years with Burkitt lymphoma disease as well as male patients need special attention. High body-mass index contributes significantly to Burkitt lymphoma burden in the United States and United Kingdom, but less so in China and India. Hopefully, this study will help optimize the prevention, diagnosis, treatment, and management of Burkitt lymphoma to reduce the disease burden.
Keywords
Key points
Globally, there were 19,072 incident cases of Burkitt lymphoma (BL) in 2021. High body-mass indexes contribution to BL is evident in the disability-adjusted life-years, with the United States and the United Kingdom recording 0.06 and 0.05, respectively. Conversely, China and India demonstrated substantially lower contributions, at 0.02 and 0.005, respectively.
The group of 0–14 and 50–74 years surpassed other age groups both in BL-associated incidence and death number.
Introduction
Burkitt lymphoma (BL) is a highly aggressive lymphoma that often presents in extra nodal sites or as an acute leukemia. It is composed of monomorphic medium-sized B cells with basophilic cytoplasm and numerous mitotic figures, usually with a demonstrable MYC gene translocation to an IG locus. In 1958, the surgeon Dennis Burkitt first observed a tumor affecting the jaw of one of the a pediatric population of Equatorial Africa. 1 This tumor was initially purported as a sarcoma of the jaw; however, it was promptly reclassified as a distinct form of non-Hodgkin’s lymphoma (NHL) based on its histopathological features. 2 BL accounts for up to 40% of pediatric lymphomas in the United States and Western Europe, 20% in adolescents. 3 In contrast, BL makes up less than 5% of all NHLs in adults. 4
BL is categorized into three distinct variants: endemic, sporadic, and immunodeficiency-associated, presenting specific epidemiologic and clinical feature. 5 Sporadic BL occurs worldwide, being more common in children and young adults, rarely affecting elderly patients, who, when affected, tend to have a significantly poorer prognosis compared to pediatric patients. 6 In equatorial Africa, Epstein–Barr virus (EBV) infection plays a causative role (endemic BL variant) to BL which is the highest incidence rate in pediatric cancer (5–10 cases per 100,000 people/year).7,8
HIV-positive patients who diagnosed with BL accounted for 10–35% of AIDS-defining lymphoma in people with HIV (PWH), making it the second most common subtype of NHL occurring in this patient populaiton. 9 BL in PWH is 261 times higher than that observed in the general population. 10 A variety of mechanisms contribute to the increased risk of BL in this population, including immune dysregulation, EBV co-infection, direct effect of the HIV Tat antigen, and multiple other structural proteins on the proliferation of polyclonal B cells. 11 The increased risk of morbidity and mortality in PWH with BL may be attributed to their higher likelihood of being diagnosed at a more advanced stage, even after accounting for healthcare-related factors.12,13 These disease dynamics, which constitute a heavy burden on patients and their families, have become global public health problems.
In this study, we utilized the Global Burden of Disease (GBD) statistical model to systematically describe the disease burden of BL encompassing incidence, mortality, and disability-adjusted life-years (DALYs), in 2021, with a focus on age and gender distribution and time trends. This analysis is valuable for clinicians, epidemiologists, and health policymakers to formulate more effective public health strategies and to further optimize the allocation of medical resources.
Methods
Data collection
The GBD 2021 project estimated the incidence, mortality, and DALY associated with 369 diseases and injuries for 204 countries and territories from 1990 to 2021. 14 Available data, standardized disease definitions, and their 95% uncertainty interval (UI) for incidence, mortality and DALYs information were gathered on all ages or age standard with BL from the GBD 2021 Data. Furthermore, the study employed the sociodemographic index (SDI), a measure that quantifies a region’s sociodemographic progression based on income, education, and fertility circumstances.
Burden description
In this study, we collected data regarding the number of cases and incidence of BL, associated mortality, and number of BL-associated DALYs, along with their corresponding rates at global, regional, and national levels. We computed mean estimated annual percentage changes (EAPCs) using linear regression. We also collected data regarding global risk factors (such as: body-mass index (BMI)) that contribute to BL mortality. To summarize age distribution of the BL burden, we divided age into four groups: 0–14, 15–49, 50–74, 75+ years.
Bayesian age-period-cohort models
Bayesian age-period-cohort (BAPC) models provide a comprehensive framework for making projections using integrated nested Laplace approximations for full Bayesian inference. 15 Key features of BAPC models include (1) generation of age-specific and age-standardized projected rates; (2) automatic addition of Poisson noise when interest lies in the predictive distribution.
Statistical analysis
Numbers of incidence, mortality, DALYs, and their corresponding rates were reported per 100,000 population, along with 95% UI according to the GBD algorithm. 16 The dynamics of BL were analyzed by calculating EAPCs to identify temporal trends in the disease burden17,18; 95% confidence intervals (CIs) of EAPCs were determined by linear modeling. If the upper limit of both EAPC and its 95% CI is negative, its corresponding rate shows a decreasing trend; conversely, if the lower limit of both an EAPC and its 95% CI is positive, its corresponding rate shows an increasing trend.19,20 The correlations between SDI level and EAPCs were visualized by Pearson’s correlation method. To predict the age-standardized rates (ASR) of incidence, death and DALYs for future BL, we used the BAPC packages in the R software to analyze the age-standardized incidence rates (ASIR) globally and in different sex groups from 2019 to 2041. 21 All calculations were performed using R Studio, version 4.2.1 (R Project for Statistical Computing). p values less than 0.05 were considered statistically significant.
Results
Global trends of Burkitt lymphoma
Incidence
In 2021, the global incident cases of BL were 19,072 (95% UI 9650–32,508). From 1990 to 2021, the global incident cases of BL increased by 207%. The corresponding incidence rate increased from 0.127 (95% UI 0.094–0.168) in 1990 to 0.236 (95% UI 0.121–0.398) in 2021; the EAPC was 2.179 (95% CI 1.788–2.572) (Table 1). The peak incidence was among boys aged 5–9 years in both 1990 and 2021 (899 and 1374, respectively, Figure 1(a) and (b)). The incidence rate of BL was consistently higher in males than in females across all ages in both 1990 and 2021 (Figure 1(c) and (d)). The male and female BL incidence numbers of different ages exhibited a bimodal distribution, with a peak among children aged 5–9 years and another peak among patients aged 65–75 years (Supplemental Figure S1).
The incident cases and ASIR in 1990 and 2021 and its temporal trends.

ASIR: age standard incident rate; EAPC: estimated annual percentage change; SDI: sociodemographic index; UI: uncertainty interval; CI: confidence interval.
EAPC is expressed as 95% CIs.
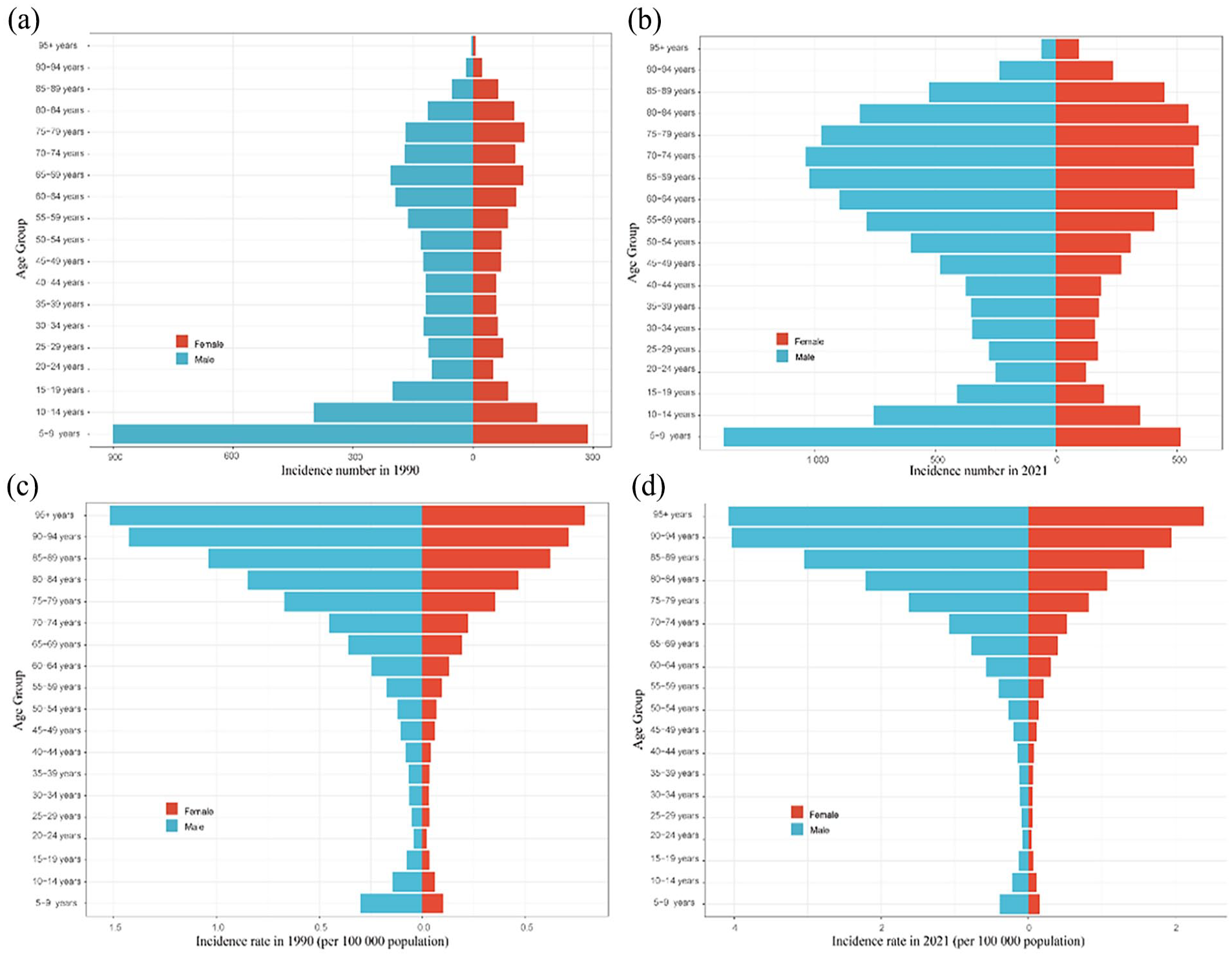
Sex- and age-structured analysis of BL global burden. (a) Age and sex distribution of incidence number in 1990; (b) age and sex distribution of incidence number in 2021; (c) age and sex distribution of incidence rate in 1990; (d) age and sex distribution of incidence rate in 2021.
Mortality
Over the past three decades, the global number of BL-associated deaths increased by 70%, from 3843 (95% UI 2483–5142) in 1990 to 6525 (95% UI 3955–9035) in 2021. However, the BL-associated death rate did not change dramatically, from 0.072 (95% UI 0.047–0.096) per 100,000 in 1990 to 0.083 (95% UI 0.050–0.114) per 100,000 in 2021; the EAPC was 0.623 (95% CI 0.449–0.797). As the number of BL deaths increased annually, the death rate also increased from 1990 to 2016, then slightly decreased from 2017 to 2021 (Supplemental Figure S2(a) and (b)). The highest numbers of deaths in 1990 and 2021 occurred among boys and girls aged 5–9 years (766 and 255 versus 1005 and 404, respectively, Supplemental Figure S3(a) and (b)). Male patients of all ages with BL, except for those over 95 years, dominated the death numbers in 1990 and 2021 (Supplemental Figure S3(c) and (d)).
Disability-adjusted life-years
The global number of BL-associated DALYs increased by 46.59% from 1990 to 2021, from 267,498 (95% UI 157,945–371,555) in 1990 to 392,126 (95% UI 244,124–512,401) in 2021; the EAPC was 0.037 (95% CI −0.052 to 0.126). From 1990 to 2021, the number of BL-associated DALYs increased in all age groups (Supplemental Figure S4(a)). The greatest increase in the number of BL-associated DALYs (23.52%) was observed among children aged 0–14 years. The groups with the highest numbers of BL-associated DALYs in 1990 and 2021 were children aged 0–14 years (207,119 and 255,842, respectively) (Table 2 and Supplemental Table S1). In 2021, the rate of BL-associated DALYs among children aged 0–14 years was higher in boys than in girls (younger than 5 years: boys 17.60; girls 6.17; 5–9 years: boys 23.69; girls 10.16; and 10–14 years, boys 11.13; girls 6.26). The rates of BL-associated DALYs slightly changed in all age groups of males and females from 1990 to 2021 (Supplemental Figure S4(b) and (c)).
The mortality, incidence, DALYs in2021 and EAPCs from 1990 to 2021 of BL in four ages groups.

DALYs: disability-adjusted life-years; EAPC: estimated annual percentage change; UI: uncertainty interval; BL: Burkitt lymphoma.
Burkitt lymphoma: national trends
Incidence
In 2021, among 204 countries, the United States of America had the most cases of BL (3572; 95% UI 5930–15,672) (Figure 2(a)). The global incidence rate of BL in 2021 was 0.236 (95% UI 0.121–0.398) (Supplemental Table S2). Andorra had the highest incidence rate of BL (1.43; 95% UI 0.46–3.13) (Supplemental Table S2 and Supplemental Figure S5(a)). Cyprus (EAPC 7.163; 95% CI 6.113 to 8.223) had the largest increase in BL incidence; Somalia (EAPC −0.065; 95% CI −0.292 to 0.163) had the largest decrease (Supplemental Table S3).

Incidence and death cases of BL in 204 countries and territories in 2021. (a) Incidence cases; (b) death cases.
Mortality
In 2021, Nigeria had the highest number of BL-associated deaths (717; 95% UI 358–1016); Tokelau had the lowest number of BL-associated deaths (0.0005; 95% UI 0.0001–0.0011) (Supplemental Table S4 and Figure 2(b)). The global BL-associated mortality rate in 2021 was 0.085 (95% UI 0.052–0.117) (Supplemental Table S6). Uganda (0.85; 95% UI 0.41–1.37) had the highest BL-associated mortality rate; Tajikistan (0.0006; 95% UI 0.0002–0.0012) had the lowest mortality rate (Supplemental Table S5 and Supplemental Figure S5(b)). American Samoa (EAPC 3.97; 95% CI 3.62 to 4.32) had the greatest increase in the mortality rate; Georgia (EAPC −3.26; 95% CI −4.21 to −2.30) had the greatest decrease (Supplemental Table S6). In 2021, Uganda (SDI 0.42) had the highest BL-associated mortality rate, whereas Tajikistan (SDI 0.54) had the lowest mortality rate.
Disability-adjusted life-years
In 2021, Nigeria had the highest number of BL-associated DALYs (57,244; 95% UI 28,150–81,255) (Supplemental Table S7 and Supplemental Figure S5(c)). The global rate of BL-associated DALYs in 2021 was 5.298 (95% UI 3.295–6.893); Uganda had the highest rate of BL-associated DALYs (52.6; 95% UI 28.0–78.8) (Supplemental Table S8). Guam (EAPC 4.466, 95% CI 4.002 to 4.931) had the greatest increase in the DALYs rate; China (EAPC −3.674; 95% CI −4.212 to −3.134) had the greatest decrease (Supplemental Table S9). Uganda (SDI 0.42) had the highest rate of BL-associated DALYs; Tajikistan (SDI 0.54) had the lowest rate.
Burkitt lymphoma: SDI regional trends
Incidence
The high SDI region had the most incidence cases of BL in 2021 (8834; 95% UI 3391–17,415) (Table 1). From 1990 to 2021, the incident cases in the high SDI region increased by 127% (95% UI 28%–176%). The greatest increase in the incidence of BL occurred in the high-middle SDI region (EAPC 3.451; 95% CI 3.069–3.833) (Table 1 and Figure 3(a)).
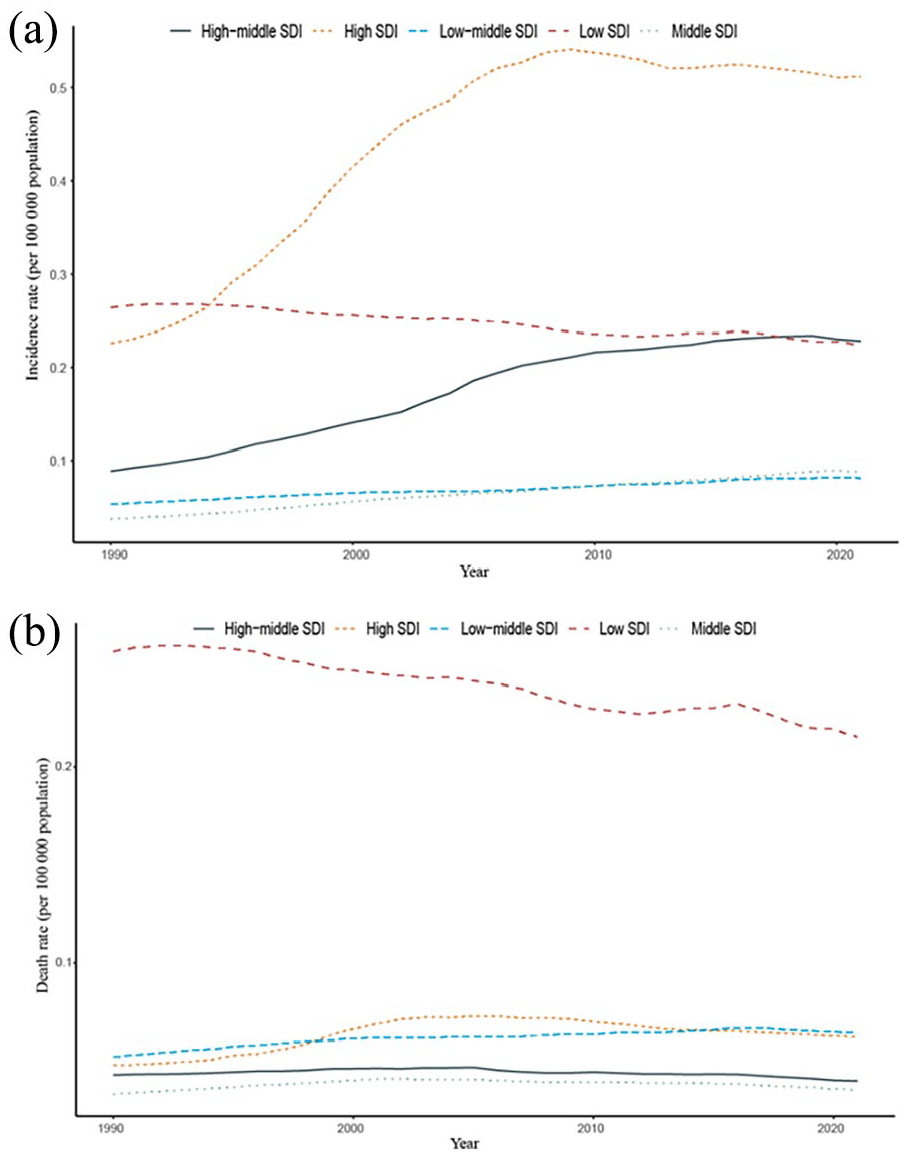
Epidemiologic trends of incidence and death rates in five SDI regions of BL from 1990 to 2021. (a) Trends in incidence rate. (b) Trends in death rate.
Mortality
The low SDI region had the highest mortality rates of BL from 1990 to 2021 compared with the other four regions (Figure 3(b)), with a death number of 1715.442 (778.405–2,617.325) in 1990 versus 2861.136 (1577.263–3907.983) in 2021 (Table 1). The mortality rates in the remaining four regions remained comparatively stable from 1990 to 2021 (Figure 3(b)). The high SDI region had the greatest EAPC (0.912; 95% UI 0.476–1.349), whereas the low SDI region had the lowest EAPC in the mortality rate (−0.621; 95% CI −0.670 to −0.572) (Supplemental Table S10).
Disability-adjusted life-years
In 2021, the low SDI region had the highest number of BL-associated DALYs (206,829; 95% UI 117,687–279,845) with a dramatic increase of 55.71% from 1990 to 2021. The high SDI region had the greatest increase (86.15%) in the number of BL-associated DALYs (Supplemental Figure S6(a)). The rate of BL-associated DALYs in the four SDI regions changed slightly, except for the low SDI region, which dropped from 18.35 in 1990 to 14.46 in 2021 (Supplemental Figure S6(b)).
Burkitt lymphoma: geographic regional trends
Incidence
Among the 21 geographic regions, Western Europe had the most cases of BL in 2021 (4504.641; 95% UI 1296.676–11,343.784), whereas Oceania had the fewest (5.184; 95% UI 1.954–9.384) (Table 1). The incidence rate of BL was highest in high-income North America (0.712; 95% UI 0.330–1.157). In contrast, the incidence rate was lowest in Central Asia (0.021; 95% UI 0.012–0.033) (Table 1). From 1990 to 2021, Central Europe had the largest increase in the incidence of BL (EAPC 4.236; 95% CI 3.588 to 4.888), whereas Eastern sub-Saharan Africa had the smallest increase (−0.786; 95% CI −0.832 to −0.740) (Table 1). With SDI lower than 0.5, the incidence rate drops every year in several regions (e.g., Eastern sub-Saharan Africa, Western sub-Saharan Africa, and Central sub-Saharan Africa), whereas it grows annually in most regions (e.g., Southern sub-Saharan Africa, Central Europe, and Southern Latin America) when 0.7 > SDI > 0.5 (Figure 4(a)). When SDI >0.7, the incidence rate in several regions started to stabilize or drop (e.g., Australasia, High-income Asia Pacific, and Central Europe, Figure 4(a)).

Incidence and death rates for BL in 21 regions from 2019 to 2021. (a) Incidence rate. (b) Death rate.
Mortality
In 2021, Eastern Sub-Saharan Africa had both the highest number of BL-associated deaths (1696; 95% UI 884–2404) and BL-associated mortality rate (0.372; 95% UI 0.182–0.586). Australasia had the smallest increase in the BL-associated mortality rate (EAPC −0.005; 95% CI −0.416 to 0.408), whereas Southern sub-Saharan Africa had the largest increase (EAPC 2.471; 95% CI 2.247 to 2.695). Among the whole range of SDI, mortality rates of several regions dropped gradually (e.g., Western sub-Saharan Africa, Eastern sub-Saharan Africa, and Central sub-Saharan Africa), while several regions increased gradually (e.g., Oceania and Southern sub-Saharan Africa) (Figure 4(b)). However, death rates of most regions increased and then went down as SDI and year time increased (e.g., Western Europe, Tropical Latin America, and High-income North America) (Figure 4(b)).
Disability-adjusted life-years
In 2021, Eastern sub-Saharan Africa had both the highest number (123,943; 95% UI 67,529–172,503) and rate (23.37; 95% UI 12.14–33.71) of BL-associated DALYs, whereas Oceania had the lowest number (298; 95% UI 105–555). Central Asia had the lowest DALYs rate (0.50; 95% UI 0.30–0.78) (Supplemental Figure S7). From 1990 to 2021, Southern sub-Saharan Africa had the largest increase in the DALYs rate (EAPC 2.70; 95% CI 2.41 to 3.00). East Asia had the largest decrease (EAPC −3.55; 95% CI −4.06 to −3.03) (Supplemental Table S11).
Risk factors for Burkitt lymphoma
The GBD database provides only one metabolic risk factor, high BMI, attributed to BL-associated DALYs. Yearly increments in the proportion of DALYs linked to high BMI have been observed worldwide (Supplemental Figure S8(a)). In 2021, High-income North America of the 21 regions had the highest attribution of high BMI, while South Africa had the smallest attribution of high BMI (Supplemental Figure S8(b)). High BMIs contribution to the burden of disease (BL) is evident in the DALYs, with the United States and the United Kingdom recording 0.06 and 0.05, respectively. Conversely, China and India demonstrated substantially lower contributions, at 0.02 and 0.005, respectively (Supplemental Figure S8(c)).
EAPCs and SDI
EAPCs differed from incidence, mortality rate, and DALYs in 2021. The EAPCs of incidence were positively correlated with SDI (Pearson’s r = 0.606; p = 0.003) (Supplemental Table S12). The correlation between EAPCs of mortality and SDI was not statistically significant; neither was that between EAPCs of DALYs and SDI (Supplemental Table S12).
BL: 0–14 years group
To summarize the age distribution of the BL burden, we divided age into four groups: 0–14, 15–49, 50–74, and 75+ years. The groups of 0–14 and 50–74 years surpassed other age groups in both BL-associated incidence and death numbers. The DALYs number (255,842.92, 95% UI 160,376.27–331,628.88) and rate (12.71, 95% UI 7.97–16.48) were apparently higher than other age groups (Table 2).
Prediction for global ASR of incidence, death, and DALYs in BL
We predicted the ASIR of episodes of BL in the next two decades using the BAPC software packages of R software. Based on the BAPC model analysis, the results demonstrated that the ASIR of BL increased from 0.24 (95% UI 0.23–0.24 per 100,000) in 2021 to 0.32 (95% UI 0.23–0.4 per 100,000) in 2041 (Figure 5(a) and Supplemental Table S13). In addition, the ASR of death prediction showed a relatively smooth trend from 2021 to 2041 (Figure 5(a)). These findings for the ASR of incidence and death in both male and female groups showed the same trends from 2021 to 2041, and notably, the incidence of developing BL was consistently much higher in males than in females (Figure 5(b) and (c)). In contrast, regarding the ASR-DALYs trend, the prediction results of the BAPC model showed a declining trend in all groups (Figure 5(d)).
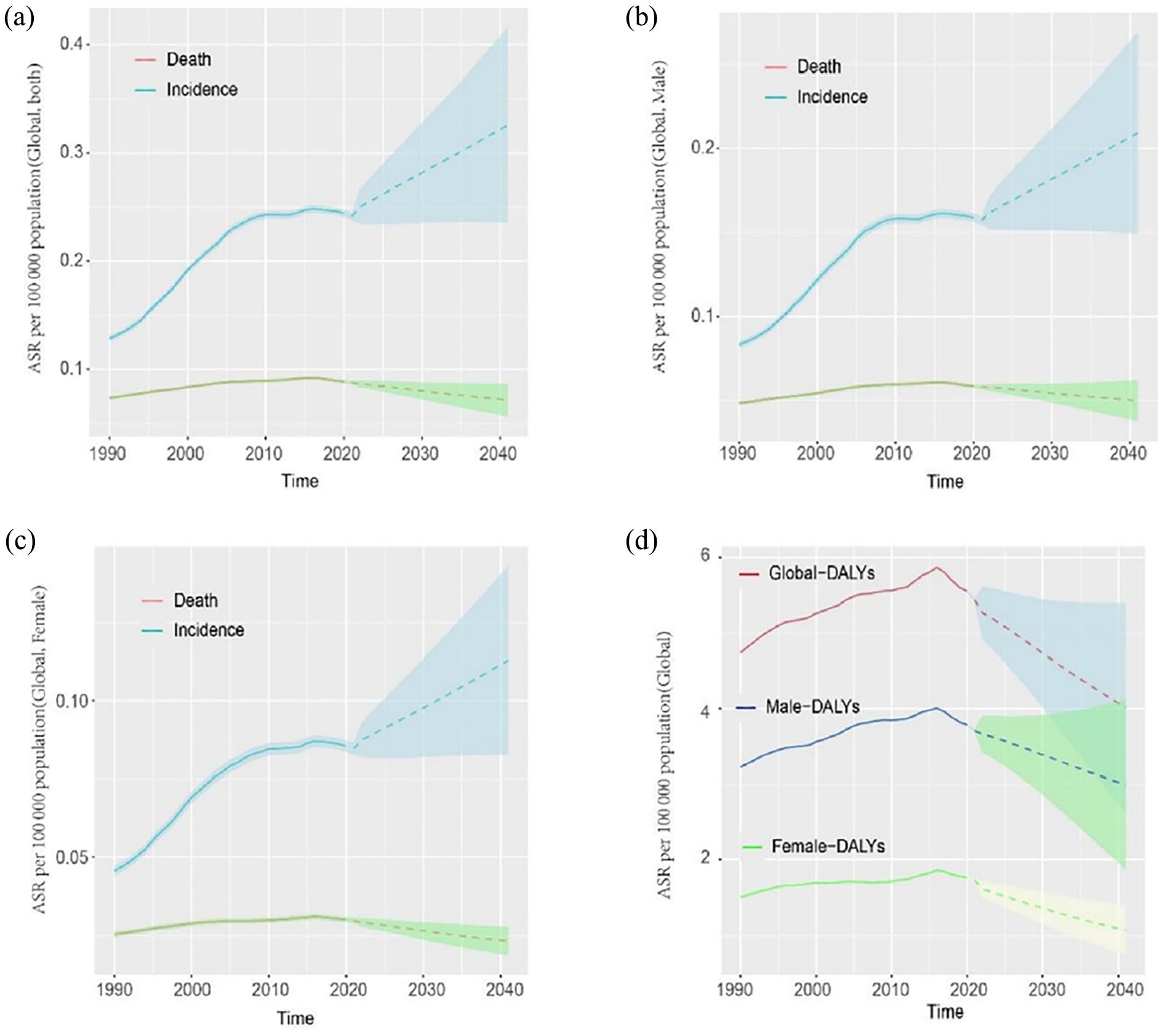
Statistics and predictions of the ASR based on BAPC model: (a) Global ASR of incidence and death; (b) male ASR of incidence and death; (c) female ASR of incidence and death; (d) ASR of DALYs.
Discussion
BL represents a significant public health challenge especially in low-middle-income regions, and the prognosis for BL that displays progression after the first-line treatment remains dismal even in western countries. 22 Therefore, its impact on incidence and mortality garners substantial research attention. In this study, we investigated BL incidence, BL-associated mortality, and BL-associated DALYs in all GBD regions and countries from 1990 to 2021. Our findings provide insights into regarding the burden of BL over the past three decades in regions and countries with varying income levels. The results indicated that the burden of BL is increasing in some regions and countries worldwide and the incidence would continue to rise in the future 20 years. A global assessment of the epidemiologic patterns of BL may help policymakers and clinicians to develop appropriate prevention and management strategies.
From 1990 to 2021, both the numbers of BL-associated deaths and BL-associated DALYs increased, which is consistent with Ying Wang’s research. 23 The global incidence rate of BL increased by 85.82%. Contrary to diabetes occurring on patients with a younger trends in children, 19 BL occurs more frequently in young (0–14 years) and old age groups (65–75 years) (Figure 1(a) and (b)). In addition, incidence, mortality and DALYs of male patient were larger than female patients almost in all age groups (Figure 1 and Supplemental Figure S3). This phenomenon was different from papillary thyroid carcinoma which favors in female patients. 24 The underling mechanism of sex-favored malignant tumor need further investigation.
SDI can be considered an index of social development, technological advancements, industrialization, and enhancements in healthcare resources. 14 Significant positive correlation between SDI and EAPCs of incidence was found (Pearson’s r = 0.606; p = 0.003) (Supplemental Table S12). The correlation between EAPCs of mortality and SDI was not statistically related; neither was that between EAPCs of DALYs and SDI. From 21 regions’ perspective, during the past three decades, the incidence rate and death rate of high SDI regions (e.g., High-income North America) decreased gradually in the past 5–10 years (Figure 4), which was presumably associated with the availability and development of better medical services in the high SDI regions. In contrast, countries in the low SDI regions (e.g., Southern sub-Saharan African) have seen an increasing BL burden in the past 5–10 years (Figure 4).
The current frontline treatment of BL is based on the use of two main chemotherapy backbones, derived from French–American–British/Lymphomes malins B (LMB84, LMB89 and LMB96) consecutive clinical trials,25 –27 and from the Berlin–FrankfurtMünster NHL90 and NHL95 regimens.28,29 Additional therapeutic methods including chemo-immunotherapy regimens, transplant, bispecific antibodies: Blinatumomab, chimeric antigen receptor T cells have garnered much interest. 22 However, these novel treatments are still in development and pose new challenges in terms of safety, cost-effectiveness, and economic burden. The data observed a steady trend in the global life expectancy of BL patients, whereas life expectancy slightly decreased in the age group of 0–14 years (Supplemental Figure S4(a)–(c)). This trend in life expectancy comes with a proportional in disease-related complications, which significantly contribute to DALYs rates.22,30
People of 0–14 years were considered the beginning of life, and 50–74 years were also the main labor in a family nowadays. On the one hand, high incidence and mortality number were the characteristics of these two groups, on the other, advanced stage, increased lactate dehydrogenase, and primary site, children less than 15 years were associated with an increased risk of treatment failure. 27 It is worthy of special attention that more attention should be paid to these two age groups.
BAPC model predict an increase in the ASIR of BL over the next 20 years (Figure 5). This trend may have been caused by the growth and aging of the global population. 31 However, this trend was different from Ying Wang’s result 23 which predicts a decline. There are several explanations to this inconsistence. First of all, it was not logical that despite the increase in incidence cases, the incidence rate has dropped, especially in the context of a rapid decrease in world population growth. 32 Second, according to our BAPC parameters and R code (Supplemental Appendix BAPC), the increasing trend can be easily repeated. We found that the ASR of DALYs did not show a steady upward trend since 1990 but fluctuated upward and then decreased. This probably result from the improvement of medical technology and economic level, and strong evidences could be found to support this phenomenon.25,26 Interestingly, ASR of death did not change dramatically from 1990 to 2021, and the trend would remain relatively stable in the future 20 years (Figure 5).
Analyses for 1990–2021 and projections for the next two decades both suggest that ASR is significantly higher in males than in females with BL. This phenomenon may be partially due to the EBV infection,9,31 alcohol consumption, and drug injection in males.
Although concerns about the burden have historically focused on HIV-related or EBV-related infections,9,33 our research shows that we may need to pay more attention to rapidly rising developing countries and countries with a rapidly changing lifestyle where people with a BMI burden is increasing. Recently, a movement announced “Healthy China 2030” by the Chinese government, aiming to facilitate appropriate diet and physical activities to reduce obesity and type 2 diabetes in the Chinese population. 34 This kind of national policy will certainly be a breakthrough for reducing BMI-related BL burden in the future.
Limitations
This study had some important limitations. First, no system has been established to classify types of BL. Second, the analysis heavily relied on the GBD database the accuracy of which is constrained by the availability of national registry data and the lack of information regarding other risk factors associated with BL, such as patients with HIV infection or EBV infection. Moreover, the real incidence of BL is likely even much higher due to underdiagnosis/registration. 35 Future studies of BL should include information that could facilitate such classification.
Conclusions
This study utilized data from GBD 2021 to delineate the burden of BL globally, regionally, and nationally, analyzing trends over a period from 1990 to 2021. Over the past three decades, the global burden of BL has gradually increased, and this burden is expected to continue increasing. Children of 0–14 years, adults of 50–74 years with BL disease, and male patients need special attention. High BMI contributes significantly to BL burden in the United States and United Kingdom, but less so in China and India. These findings highlight the importance of specific measures to deal with this growing global health problem.
Supplemental Material
sj-rar-1-smo-10.1177_20503121241313083 – Supplemental material for 1990–2041 Global burden of Burkitt lymphoma with 20 years forecast: A systematic analysis using the global burden disease of study of 2021
Supplemental material, sj-rar-1-smo-10.1177_20503121241313083 for 1990–2041 Global burden of Burkitt lymphoma with 20 years forecast: A systematic analysis using the global burden disease of study of 2021 by Chengyun Dou, Yidan Sang, Hongbo Zhu and Chuangjie Cao in SAGE Open Medicine
Supplemental Material
sj-rar-2-smo-10.1177_20503121241313083 – Supplemental material for 1990–2041 Global burden of Burkitt lymphoma with 20 years forecast: A systematic analysis using the global burden disease of study of 2021
Supplemental material, sj-rar-2-smo-10.1177_20503121241313083 for 1990–2041 Global burden of Burkitt lymphoma with 20 years forecast: A systematic analysis using the global burden disease of study of 2021 by Chengyun Dou, Yidan Sang, Hongbo Zhu and Chuangjie Cao in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all the participants for their contribution to the research.
Author contributions
Chuangjie Cao and Chengyun Dou: Conceptualization, Supervision, Writing—review & editing; Hongbo Zhu: Draft preparation, Writing—review & editing, Software; Yidan Sang: Statistic analysis, Data preparation and curation.
Data availability statement
Research data and other items supporting the results in this article are available upon reasonable request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The GBD study is based entirely on publicly available databases and does not require clinical ethics approval.
Informed consent
Not applicable.
Patient consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.