
Abstract
Recently, the measurement of the pupil dilation response has been applied in many studies to assess listening effort. Meanwhile, the mechanisms underlying this response are still largely unknown. We present the results of a method that separates the influence of the parasympathetic and sympathetic branches of the autonomic nervous system on the pupil response during speech perception. This is achieved by changing the background illumination level. In darkness, the influence of the parasympathetic nervous system on the pupil response is minimal, whereas in light, there is an additional component from the parasympathetic nervous system. Nineteen hearing-impaired and 27 age-matched normal-hearing listeners performed speech reception threshold tests targeting a 50% correct performance level while pupil responses were recorded. The target speech was masked with a competing talker. The test was conducted twice, once in dark and once in a light condition. Need for Recovery and Checklist Individual Strength questionnaires were acquired as indices of daily-life fatigue. In dark, the peak pupil dilation (PPD) did not differ between the two groups, but in light, the normal-hearing group showed a larger PPD than the hearing-impaired group. Listeners with better hearing acuity showed larger differences in dilation between dark and light. These results indicate a larger effect of parasympathetic inhibition on the pupil dilation response of listeners with better hearing acuity, and a relatively high parasympathetic activity in those with worse hearing. Previously observed differences in PPD between normal and impaired listeners are probably not solely because of differences in listening effort.
Introduction
Speech understanding is usually perceived as more challenging and effortful for people with hearing impairment than for normally hearing people, especially in background noise (Kramer, Zekveld, & Houtgast, 2009; Pichora-Fuller et al., 2016; Plomp & Mimpen, 1979; Rönnberg, Rudner, & Foo, 2008; Zekveld, Kramer, & Festen, 2011). Frequently experiencing effortful listening may be associated with higher levels of experienced fatigue in listeners with hearing-impaired (HI) as compared with their normal-hearing (NH) peers (Edwards, 2007; Hornsby, Naylor, & Bess, 2016). The consequences of hearing-related fatigue may include restrictions in engagement in work and withdrawal from major social roles (Kramer, Kapteyn, & Houtgast, , 2006; Nachtegaal et al., 2009).
To gain a better understanding of listening effort and approaches to the assessment of listening effort in various situations, the Eriksholm Workshop on Hearing Impairment and Cognitive Energy (Pichora-Fuller & Kramer, 2016) proposed relevant measurements ranging from self-reported questionnaires (Gatehouse & Noble, 2004) to physiological measurements like functional Magnetic Resonance Imaging (Vaden, Kuchinsky, Ahlstrom, Dubno, & Eckert, 2015), skin conductance (Mackersie & Calderon-Moultrie, 2016), and pupillometry (Koelewijn et al., 2014; Kramer, Teunissen, & Zekveld, 2016; Kuchinsky et al., 2013; Ohlenforst et al., 2017; Wang et al., 2017; Winn, Edwards, & Litovsky, 2015; Zekveld, Kramer, & Festen, 2011). Larger pupil dilation is associated with higher levels of listening effort during speech perception in noise. While measuring speech comprehension across a wide range of signal-to-noise ratios (SNRs), a recent study found that the relationship between speech intelligibility (range from 0% to 100% correct response) and the peak pupil dilation (PPD) follows an inverted U–shaped curve. The largest pupil dilation occurs when the intelligibility is around 50% correct performance and this pattern was observed in both NH and HI listeners (McMahon et al., 2016; Ohlenforst et al., 2017). When assessing the PPD during the speech-in-noise task around this 50% correct level, one may intuitively assume that HI listeners would show larger pupil dilation compared with NH listeners, as they would expend more listening effort because of their hearing deficit. However, previous studies have repeatedly reported the opposite finding in challenging listening conditions (50% intelligibility level), namely, that the PPDs are smaller in HI participants than NH controls (Kramer et al., 2016; Wang et al., 2017; Zekveld et al., 2011).
These contradictory findings may indicate that PPD during a speech in noise task might not be a pure indicator of listening effort. Other factors (that differ between NH and HI) could also have an impact on the pupil dilation response. It is possible that such-as-yet unobserved factors are related to the lower level mechanisms that control the pupil response, while previous research has mainly focused on the influence of higher level processing (e.g., listening effort). As such, we first review the basic physiological mechanism of the pupil response and its association with the autonomic nervous system (ANS). The pupil response is under the direct control of the ANS. The ANS is the involuntary nervous system that regulates both the internal environment and the sequence of basic physiological events allowing an organism to optimally adjust to environmental changes (Janig & Habler, 2000; Robertson, 2004). The ANS consists of two main branches: the sympathetic nervous system (SNS), known to govern the “fight or flight” response of the human body, which functions like the gas pedal of a car—to accelerate the body’s functioning in response to stressors, and the parasympathetic nervous system (PNS), which is in charge of the “rest and digest” response, and acts like the brake of a car—to slow the body down and recover from the stress. It has often been assumed that the task-induced pupil dilation response reflecting cognitive processing load is mainly driven by the SNS activation (Kahneman, 1973). In fact, the momentary pupil diameter reflects a balance between sympathetic and parasympathetic activation (Steinhauer, Siegle, Condray, & Pless, 2004). SNS directly controls the dilator muscle and more SNS activity means more dilational force on the pupil. PNS indirectly controls the sphincter (constrictor) muscle. Other things being equal, more PNS activity means more constrictive force on the pupil. However, the PNS control pathway passes via the Edinger–Westphal nucleus, where the activation may be affected by task-induced inhibition (Laeng, Sirois, & Gredebäck, 2012). Inhibition of a given level of PNS activity at the Edinger–Westphal nucleus means less stimulation of the sphincter muscle and thus less constrictive force on the pupil. Hence, the task-evoked pupil dilation reflects combined PNS and SNS activation (I. E.Loewenfeld & Lowenstein, 1993; Steinhauer et al., 2004). It is therefore not unreasonable to suppose that the counterintuitive findings mentioned in the previous paragraph could be because of a difference in the balance of PNS and SNS activity between NH and HI participants. To test this hypothesis, one needs to identify or disentangle the relative contributions of the PNS and SNS components in the pupil response. This is particularly crucial to those researchers who wish to interpret their pupillometry findings from the perspective of the ANS.
When studying the relative contribution of PNS and SNS activity to the pupil dilation in response to cognitive processing, it is important to note that, in darkness, PNS activity and its inhibition at the Edinger–Westphal nucleus have negligible effect on the pupil size (I. E. Loewenfeld & Lowenstein, 1993), meaning that any task-induced changes in pupil size in darkness cannot be attributed to the PNS. Steinhauer et al. (2004) exploited this characteristic to disassociate the contributions of the SNS and PNS on the pupil dilation response in a mental task. Participants performed an arithmetic task in which they continuously had to subtract seven or continuously add one. Crucially, the tasks were performed in either a dark or a light condition while the pupil dilation response was recorded at the same time. In the light condition only, there was an (expected) larger pupil dilation for the difficult task (subtract seven) compared within the easier task (add one). Steinhauer et al. therefore concluded that the additional pupil dilation in the light condition evoked by the extra processing in the difficult task was mainly associated with the parasympathetic pathway (where task-induced inhibition at the Edinger–Westphal nucleus would reduce constrictive force, resulting in greater dilation). This was confirmed by a follow-up study in which they pharmacologically blocked either the parasympathetic or sympathetic pathway. The findings from the abovementioned study indicate that it should be possible to quantify the influence of the PNS on the task-induced pupil dilation by subtracting the pupil dilation evoked by a task performed in dark from the dilation evoked by the same task performed in light conditions.
Wang et al. (2017) measured the speech reception threshold (SRT) targeting 50% correct response for a group of NH and an age-matched group of HI participants while the pupil dilation response was measured in ambient light (360 cd/m2). The results showed that NH participants had larger PPD than the HI participants during the SRT task. The Need for Recovery (NfR) and the Checklist Individual Strength (CIS) questionnaires, which are short questionnaires to evaluate daily-life fatigue, were also administered to both groups of participants. The results demonstrated that NfR and CIS—combined as a fatigue factor, and the hearing acuity factor, which was composed of pure-tone average (PTA) and Speech Intelligibility Index (SII), had independent and almost equal contributions to the PPD during the SRT task targeting 50% correct response. Higher level of fatigue and poorer hearing acuity were associated with smaller PPD. Both fatigue and hearing acuity might be connected to PNS. Based on the PNS’s role in “rest and digest” (Fink, 2000), a recent study suggested that higher NfR may be related to a higher level of PNS activity, as evidenced by the pupil light reflex (Wang et al., 2018). This suggests that individuals with higher levels of fatigue use more “brake power”—higher levels of PNS activity—to recover from fatigue. Possibly, the PNS is also associated with the relatively small task-evoked pupil dilation in HI listeners compared with NH listeners in difficult listening conditions. Increased PNS activity is suggested to be related to greater ability to unwind or recover from stress. This has been suggested by Hasson, Theorell, Liljeholm-Johansson, and Canlon (2009), who found that people with hearing loss have reduced PNS activity comparing with their NH peers. The true direction of any association between hearing impairment and PNS (whether reduced or more activated PNS) remains unclear as only a few studies have investigated this association (Wang et al., 2016). Therefore, the main focus of this article is to describe a method that aims to provide a better understanding of the influence of the PNS and SNS on the pupil dilation response during speech perception.
In Wang et al. (2017), pupil dilation was measured in light. Hence, according to the abovementioned reasoning, the pupil dilation response was driven by both SNS and PNS activity. When the same task is performed in darkness, the PNS pathway has a negligible effect on the task-induced pupil dilation (Steinhauer et al., 2004); so if we hypothesize that the difference in pupil dilation between the two groups observed in light is associated with the PNS pathway, and assume that SNS action is the same in both groups, then we should expect to see no difference in the pupil dilation response between NH and HI listeners in darkness. Going one step further, the difference in the pupil dilation between dark and light conditions should reflect effects within the PNS pathway, and how these vary between participants with better and worse hearing acuity. Because NH participants may exhibit less PNS activity (having less need to recover from stress and fatigue caused by hearing problems), we may expect participants with better hearing acuity to show larger differences between PPD in dark and light conditions than those with worse hearing acuity. In addition, as described earlier, high-level of fatigue has been found to be associated with reduced pupil dilation in light (Wang et al., 2017) and a more activated PNS (Wang et al., 2018). Therefore, we may hypothesize that participants with higher levels of fatigue will show smaller PPD differences between dark and light than those with lower levels of fatigue.
To investigate the research questions mentioned earlier, we extended the dataset reported in Wang et al. (2017), and included pupil dilation response data collected in both light and dark conditions. The pupil dilation data in light in the current article are identical to the data reported in Wang et al. (2017), and the data recorded in darkness were acquired during the same session as the light data.
The hypotheses tested in this study are summarized as follows:
Hypothesis 1 (H1): At 50% correct speech understanding, there is no difference in the PPD in dark between the NH and HI groups. Hypothesis 2 (H2): Participants with better hearing acuity show larger difference of PPD between dark and light conditions. Hypothesis 3 (H3): Participants with a lower level of fatigue show larger difference of PPD between dark and light conditions.
Methods
Participants
A total of 19 (13 women) HI and 27 (17 women) NH participants were recruited from the VU University Medical Center, local community centers and hearing aid dispensers in Amsterdam. All participants were native Dutch speakers without any history of neurological, psychiatric, or ophthalmological conditions that might alter the pupil response. The ages of the HI participants ranged from 22 to 59 years, with a mean age of 47 years (standard deviation [SD] = 10.9 years). The age range of the age-matched NH participants ranged from 21 to 58 years, with a mean age of 46 years (SD = 12.4 years). Pure tone audiometry was measured at the beginning of the test session. The NH participants had PTAs of 20 dB hearing loss (HL) or lower for octave-band frequencies between 250 and 4000 Hz. The inclusion criteria for the HI participants were as follows: They should have a sensorineural hearing loss with PTA between 35 and 65 dB HL and an air-bone gap < 10 dB between 500 and 4000 Hz. The hearing loss had to be symmetrical (the difference between the left and right ear had to be < 20 dB at one frequency or 15 dB at two frequencies or 10 dB at three frequencies across 250, 500, 1000, 2000, and 4000 Hz; see Figure 1). The study was approved by the Ethical Committee of the VU University Medical Center. All participants provided written informed consent before the test session.
Means and SDs (indicated by error bars) of the unaided pure-tone thresholds for each ear for two groups of participants.
Speech Reception Threshold Test
In the SRT test, 25 female-talker daily Dutch sentences each were selected from an open set (Versfeld, Daalder, Festen, & Houtgast, 2000) and used as the target speech. The target speech was masked by a single-talker masker that was composed of a stream of male-talker single sentences taken from the same sentence database. The masker signal was equalized to have an identical long-term average equivalent spectrum as the target female speech. For each sentence, the single-talker masker was presented 2 seconds before target speech onset and ended 3 seconds after target speech offset. Participants were asked to repeat the target sentence after noise offset and ignore the single-talker masker. Participants were instructed to repeat the sentence aloud. The experimenter then scored the sentence and a sentence was only scored as correct if the participants reproduced the sentence completely correct without any errors. The SRT test was conducted using an adaptive procedure (one-up-one-down) to estimate the SNR required for perceiving 50% sentences entirely correctly (Levitt, 1971). The noise level was fixed to 65 dB SPL for both ears and we varied the level of target speech signal during the adaptive procedure. The initial SNR was set to −10 dB and the first sentence was repeatedly presented with increasing SNRs in 4-dB steps until the participants correctly reproduced the first sentence. The succeeding sentences were only presented once with 2-dB steps depending on whether the preceding sentence was repeated correctly or not. The SRT score was calculated based on the mean of SNR of Sentences 5 to 25. For HI listeners, the SRT test was performed without their hearing aid(s) and we amplified the mixed target speech and noise signal to each ear separately in accordance to the National Acoustic Laboratories’ linear fitting procedure, revised version (Byrne & Dillon, 1986). Two conditions were presented in which different sets of sentences were used. In one condition, the SRT test was performed in darkness, and in the other condition, the SRT test was performed in ambient light.
Speech Intelligibility Index
The SII provides extra information by estimating the proportion of speech information that is both audible and usable for a listener (Hornsby, 2004). The calculation procedure was identical to the SII score stated in Wang et al. (2017). The SII was calculated based on the signal and noise levels at each participants’ SRT, so the parameter was then termed as SII@SRT. The calculation procedure was performed following the ANSI S3.5-1997 standard.
Questionnaires
The NfR questionnaire is an 11-item scale assessing the effects of fatigue caused by work and the need for recovery later. Examples of items included in the scale are as follows: “In general, it takes me over an hour to feel fully recovered after work,” or “At the end of the day I really feel worn out.” Possible responses are “yes” or “no.” The total NfR score is the number of “yes” responses divided by the total number of items, presented as a percentage (i.e., range 0–100). The higher the score, the greater the NfR felt by the respondent. Similarly, the CIS questionnaire has been used to evaluate persistent fatigue not only in the general population, but also in the working population (Beurskens et al., 2000; Vercoulen et al., 1994). The questionnaire consists of four dimensions, each with five statements. Subject needs to choose from a 7-point Likert scale for each statement. We used the total score of the 20 items in this study (i.e., range 20–140). Higher scores indicate a higher degree of fatigue, more concentration problems, reduced motivation, and less activity. Both NfR and CIS questionnaires were designed and validated in Dutch.
The Fatigue Factor and the Hearing Acuity Factor
The fatigue factor and the hearing acuity factor were calculated from factor analysis as described in Wang et al. (2017). The fatigue factor was composed of NfR and CIS scores and the hearing acuity factor was the combination of PTA and SII@SRT. These two factors were later used in the statistical analysis to investigate the relationships between fatigue, hearing acuity, and the difference of PPD between dark and light conditions.
Apparatus
The test took place in a sound-treated booth located in VU University Medical Center. Participants were asked to sit straight in a comfortable chair and fixate their eye gaze to a small white dot (luminance < 0.1 cd/m2) located in the center of a computer screen. The center of the screen was adjusted to the eye height, and the distance between the center of the screen to the midpoint of eyes was approximately 55 cm. A remote eye tracking system (SMI RED 500, SensoMotoric Instruments, Berlin, Germany) placed below the computer screen was used to record the pupil response. Pupil diameters of both eyes (only data from the left eye were used) were recorded with a sampling rate of 60 Hz and a spatial resolution of 0.03°. The ambient light intensity was controlled by an array of light-emitting diodes placed on the ceiling of the booth. The perceived light intensity was approximately 360 cd/m2 for the light condition, and 0.1 cd/m2 for the dark condition. Auditory stimuli were presented binaurally via headphones (Sennheiser, HD 280).
Procedures
Participants were asked to visit the lab twice as the presented experiment was part of a larger study (Wang et al., 2017). Data presented in the current article were collected during the second visit. A set of questionnaires, including NfR and CIS, was given to the participants during the first visit, to be filled in at home, and returned at the second visit. Before the test session, participants were told not to wear makeup or contact lenses. Coffee consumption was also not allowed on the same day prior to the test. After 5 minutes dark adaptation time, participants performed the SRT test in dark and light conditions, and the order was counterbalanced across participants. Pupil recording continued throughout each condition. In some cases, participants started to lower their eyelid and blink more often as time went on. The experimenter then reminded the participants to avoid blinking or closing their eyelids.
Pupillometry and Pupil Data Processing
A detailed specification of pupil data processing can be found in Zekveld, Kramer, and Festen (2010) and Wang et al. (2017). For each of the 25 sentences in each condition (dark/light), the pupil data collected during the first four sentences was discarded. For the pupil data collected during the remaining 21 sentences, diameters more than 3 SDs smaller than the mean diameter during each sentence, together with zero diameter values, were coded as blinks. We rejected trials of which the data contained more than 20% blinks. A linear interpolation was applied to replace the blinks in the remaining traces, and a 5-point moving average filter was applied to filter out any high frequency artifacts. The baseline pupil diameter (BPD) was defined as the average pupil diameter in a 1-second period prior to target speech onset, during the presentation of the single-talker masker (see Figure 2). The smoothed pupil dilation data during the presentation of the target speech until masker offset were baseline corrected by subtracting the BPD. The PPD was defined as the maximum pupil diameter relative to the BPD between sentence onset and masker offset.
Averaged baseline-corrected pupil responses during SRT test for 50% correct sentence recognition in both dark and light conditions: NH (normal-hearing) versus HI (hearing-impaired).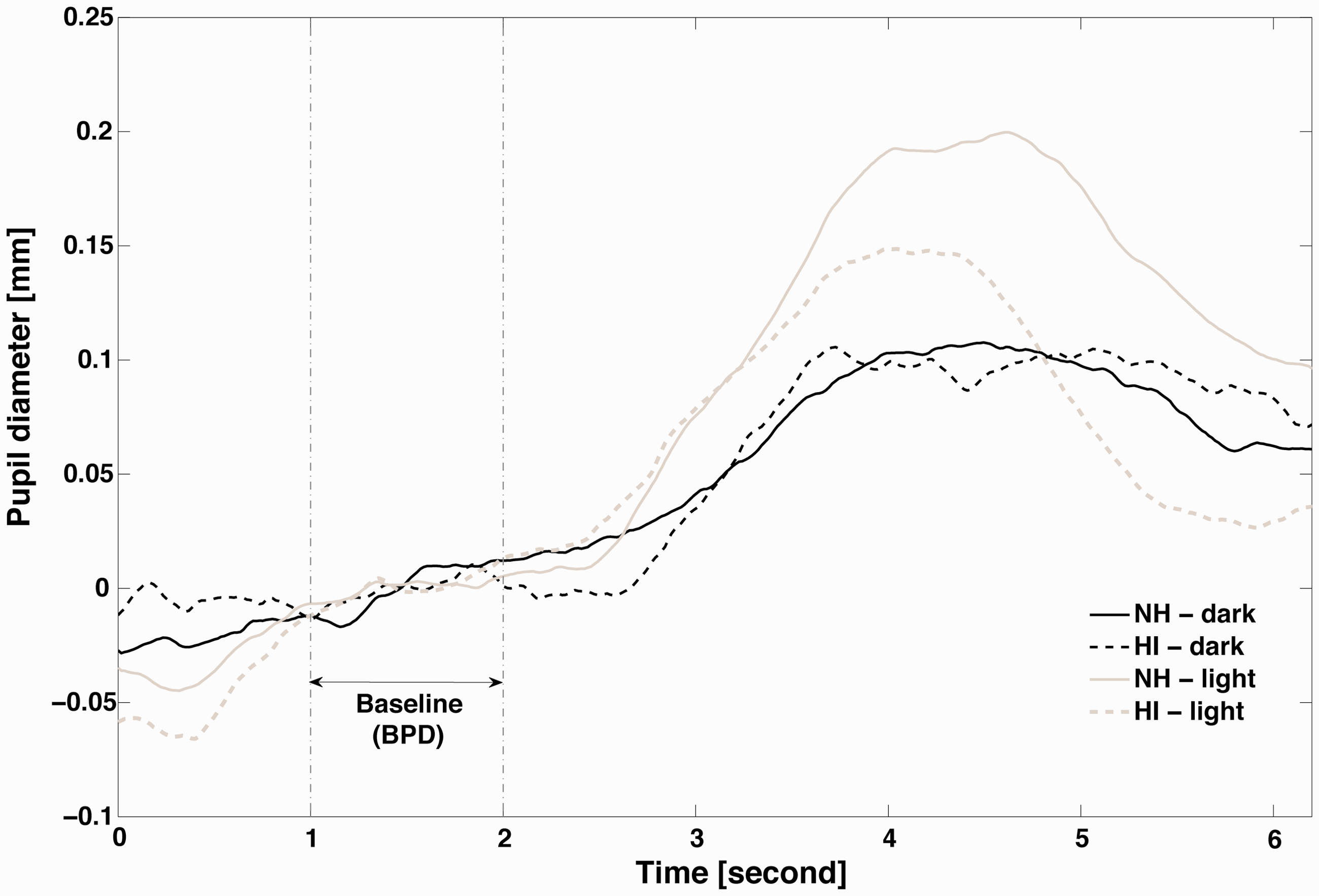
Statistical Analysis
We first ran a descriptive statistical analysis on age, NfR, CIS scores, the SRT (dB SNR), and the pupil parameters in the dark and light condition. This was followed by a planned comparison for the PPD in dark as we expected there was no significant difference between the two groups (corresponding to H1). Next, we performed a repeated-measure analysis of variance (ANOVA) using PPD in dark and light as dependent variables, hearing acuity factors and fatigue factors as covariates, to see whether there is any interaction effect between PPD condition (dark vs. light) and fatigue factor/hearing acuity factor (corresponding to H2 and H3). Finally, we ran a Spearman correlation analysis on the age, PTA, SRT, NfR, CIS scores, and pupil parameters in dark and light to provide more insight into the associations between these variables.
Results
Behavioral Data
Descriptive Statistic of Age, PTA, NfR Score, SRT Performance, and Pupil Parameters.

Note. PTA = Pure-tone average hearing threshold; NfR = need for recovery; CIS = Checklist Individual Strength; SRT = speech reception threshold; BPD = baseline pupil diameter; PPD = peak pupil diameter; SD = standard deviation; SNR = signal-to-noise ratio; HL = hearing loss; NH = normal hearing; HI = hearing impaired.
NFR and CIS Scores
The mean NfR scores were 33.0 (SD = 28.5) and 45.7 (SD = 28.9) for the NH and HI groups, respectively. The mean CIS scores were 55.7 (SD = 23.3) and 61.6 (SD = 20.7) for the NH and HI groups, respectively.
Effect of Hearing Status on PPD in Dark
To test H1, we ran a planned comparison to test the effect of hearing status (NH vs. HI) on PPD in dark. No significant difference was found between the NH and HI groups, t(44) = 0.09, p = .77, in dark. Figure 2 shows the averaged baseline-corrected pupil responses for the NH and HI groups in both dark and light. (Note that the absolute pupil diameter was always greater in dark than in light, as reflected in the differences in baseline pupil diameter shown in Table 1.)
Effects of Fatigue and Hearing Acuity on PPD in Dark and Light
To test H2 and H3, we performed a repeated-measure ANOVA using PPD in dark and light as dependent variables, and hearing acuity factors and fatigue factors as covariates. There was a significant main effect of condition (dark vs. light), such that PPD was significantly larger in the light condition than in the dark condition, F(1, 43) = 7.06, p < .012. In addition, we found significant between-subject effects of the fatigue, F(1, 43) =7.12, p < .012, and the hearing acuity, F(1, 43) = 4.39, p < .043, factors, such that PPDs were larger for participants with less fatigue and better hearing acuity. There was also a significant interaction effect of condition and hearing acuity factor, F(1, 43) = 4.87, p < .034, such that participants with better hearing showed larger differences in PPD between dark and light conditions. There was no interaction effect between condition and fatigue factor, F(1, 43) = 2.19, p < .147.
Spearman Correlation Coefficients Between Age, PTA, SRT, NfR, CIS, and Pupil Parameters
Spearman Correlation Coefficients Between Age, PTA, NfR Score, BPD, and PPD During the SRT Test in Dark and Light Conditions.

Note. PTA = Pure-tone average hearing threshold; NfR = need for recovery; CIS = Checklist Individual Strength; SRT = speech reception threshold score; BPD = baseline pupil diameter; PPD = peak pupil diameter.
Correlation is significant at the .05 level (two-tailed).
Correlation is significant at the .00625 level (two-tailed).
Discussion
In this study, the relationships between hearing impairment, daily-life fatigue, and ANS activity were examined by comparing the difference in PPD between dark and light conditions during SRT tasks targeting 50% correct response. The first aim of this study was to see if there was any difference in PPD between the NH and HI participants when measuring the pupil dilation in different light conditions, namely, light and dark. The second aim was to further examine the difference in the PPD between dark and light condition, and its association with hearing acuity and fatigue.
Pupil Dilation in Dark and Light Conditions
In our previous study (Wang et al., 2017; based on data from the same participants as the current study), we found that the pupil dilation recorded in light during the SRT task was negatively associated with fatigue and hearing acuity factors, such that people with worse hearing and higher level of fatigue showed smaller PPD. To gain a better understanding about these associations and the role of PNS, we extended the previous data set by analyzing the pupil dilation data recorded during the SRT test in a dark condition.
When the test was performed in light, NH participants showed a significantly larger PPD than the HI participants (Wang et al., 2017). However, no difference was present between the groups when testing in darkness. This finding supports our H1 (no difference in the PPD in dark between the NH and HI groups). According to Steinhauer et al. (2004), the influence of the PNS on the task-evoked pupil dilation is minimal when recording in dark. In other words, the pupil dilation response in dark is mainly driven by SNS activation. Therefore, we may infer that the contribution of SNS activation to the pupil dilation response is similar between NH and HI participants. When the same task is measured in the presence of ambient light, the effect of the PNS pathway on the pupil size also becomes apparent (Lowenstein & Loewenfeld, 1950). As such, the larger PPD observed for NH participants when testing in a light condition might indicate a smaller constrictive force via the PNS pathway for the NH group than for the HI group during the test (i.e., a more active PNS in the HI group). One may argue that the absence of a difference in pupil dilation between the two groups in dark was because of a ceiling effect on the pupil size (i.e., the pupil size had already reached its maximum and there was no room for further dilation). However, we believe this was unlikely to be the case in the current study as the pupil may dilate more than 0.5 mm when recording in dark (Steinhauer & Hakerem, 1992; Steinhauer et al., 2004). Also, the baseline pupil size was similar for the two groups in both dark and light conditions (p > .62).
The Interaction Between Hearing Acuity Factor, Fatigue Factor, and PNS as Reflected by the Difference in the PPD Between Dark and Light Conditions
We found a significant interaction effect between PPD difference across conditions (dark vs. light) and the hearing acuity factor, such that H2 was supported. People with worse hearing acuity showed a smaller difference in PPD between dark and light conditions, indicating a more activated PNS. Therefore, the current finding suggests increased PNS activity for people with hearing problems.
We did not observe any significant interaction effect between PPD difference across conditions (dark vs. light) and the fatigue factor, so H3 was not supported.
Previous studies have suggested that parasympathetic activity may be protective against the stress caused by hearing problems (Hasson et al., 2009; Horner & Higueret, 1998). A recent systematic review investigating the possible connection between hearing impairment and PNS functioning underlined the need for more research into this topic (Wang et al., 2016). Hasson et al. (2009), however, did examine this relationship and found a negative correlation between hearing problems and parasympathetic activity, which was evaluated by the high-frequency component of the heart-rate variability. The authors believed their finding indicated that people with worse hearing problems had lower levels of PNS activity and thus had a worse ability to “unwind” or recover from the stress related to their long-lasting hearing problem. These results seem to contradict the current findings, as the present results suggest increased PNS activity for people with hearing problems. There are two possible explanations for the inconsistency between the current and Hasson’s findings: (a) it is possible that heart-rate variability indicators are not assessing exactly the same dimension of PNS activity as the pupil parameters (Bär et al. 2009; Daluwatte, Miles, & Yao, 2012). (b) The sample tested in the study of Hasson included orchestra musicians. The cause of the hearing problems and the hearing-related difficulties they face in daily-life situation could be different than those experienced by the current sample of listeners with hearing loss. Nevertheless, further research is needed to better understand the relationship between hearing impairment and PNS activity.
We speculate that the current findings reveal a potential hidden confound in previous studies which compared PPD between NH and HI groups, such that the observed PPD differences at 50% correct performance reflect a mixture of group differences in PNS activity/inhibition and group differences in listening effort. More research is needed to confirm this hypothesis.
Age and Baseline Pupil Diameter
We observed negative correlations between age and BPD in both dark and light conditions. Younger participants tend to show larger BPD than the elderly participants. Previous studies have reported similar correlations between age and resting BPD (Bitsios, Prettyman, & Szabadi, 1996; Bourne, Smith, & Smith, 1979; I. Loewenfeld, 1979). For instance, Bitsios et al. (1996) found smaller resting BPD in an elderly group (median age = 69.0 years) than in a younger group (median age = 19.5 years) in dark, as well as in the presence of ambient light. Similar associations have also observed when recording pupil dilations during cognitive processing (Van Gerven, Paas, Van Merrienboer, & Schmidt, 2004; Tsukahara, Harrison, & Engle, 2016). Because the BPD is also a parameter reflecting the balance between PNS and SNS activity, the diminished BPD in elderly groups may be because of age-related changes of activity in PNS, SNS, or both systems. A systematic review has pointed out that diseases related to PNS dysfunctions, such as Parkinson and Alzheimer’s, could influence the BPD of pupil light reflex because of cholinergic deficiency (Wang et al., 2016). Further studies are needed to investigate the exact interaction between SNS and PNS activity and aging.
Conclusion
This study demonstrates the difference in pupil dilation response during a speech recognition task targeting 50% correct performance between dark and light conditions. In the dark condition, there was no difference in PPD between NH and HI participants. However, in the light condition, NH participants showed larger PPD than HI participants. Participants with better hearing acuity showed a larger difference in the pupil dilation response between the dark and light condition than participants with worse hearing acuity. Specifically, the current results may suggest relatively high parasympathetic activity in listeners with hearing loss and, therefore, it is possible that previously observed counterintuitive differences in PPD in NH versus HI may reflect differences in PNS activity unrelated to the task at hand, rather than (or as well as) differences in listening effort.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by European Commission (grant LISTEN607373) and the Oticon Foundation. Co-author G. N. was supported by grants MC_UU_00010/4 and MR/S003576/1 from the UK Medical Research Council and by a grant from the Chief Scientist Office.