
Abstract
Since somatic or somatosensory tinnitus (ST) was first described as a subtype of subjective tinnitus, where altered somatosensory afference from the cervical spine or temporomandibular area causes or changes a patient’s tinnitus perception, several studies in humans and animals have provided a neurophysiological explanation for this type of tinnitus. Due to a lack of unambiguous clinical tests, many authors and clinicians use their own criteria for diagnosing ST. This resulted in large differences in prevalence figures in different studies and limits the comparison of clinical trials on ST treatment. This study aimed to reach an international consensus on diagnostic criteria for ST among experts, scientists and clinicians using a Delphi survey and face-to-face consensus meeting strategy. Following recommended procedures to gain expert consensus, a two-round Delphi survey was delivered online, followed by an in-person consensus meeting. Experts agreed upon a set of criteria that strongly suggest ST. These criteria comprise items on somatosensory modulation, specific tinnitus characteristics, and symptoms that can accompany the tinnitus. None of these criteria have to be present in every single patient with ST, but in case they are present, they strongly suggest the presence of ST. Because of the international nature of the survey, we expect these criteria to gain wide acceptance in the research field and to serve as a guideline for clinicians across all disciplines. Criteria developed in this consensus paper should now allow further investigation of the extent of somatosensory influence in individual tinnitus patients and tinnitus populations.
Introduction
Tinnitus is the phantom sensation of sound in the absence of overt acoustic stimulation (Landgrebe et al., 2012). It occurs in approximately 10% to 15% of adults and is experienced as severely annoying by 1.6% (Baguley, McFerran, & Hall, 2013). Reported prevalence ranges can vary, depending on the way tinnitus is diagnosed and the age and gender of the assessed population (McCormack, Edmondson-Jones, Somerset, & Hall, 2016).
Tinnitus is mostly subjective, as only the patient experiences it, and it is generally described as whistling, hissing, sizzling, or ringing (Baguley et al., 2013). Typically, tinnitus is related to hearing loss or a noise trauma, where cochlear abnormalities are the initial source, and neural changes in the central auditory system maintain the tinnitus (Baguley et al., 2013).
In the 1990s, the first researchers (Hiller, Janca, & Burke, 1997; Pinchoff, Burkard, Salvi, Coad, & Lockwood, 1998) started to mention a possible influence of the somatosensory system on tinnitus complaints, but it was only in 1999 that Levine (1999) first described a hypothesis for this tinnitus subtype, which he named somatic tinnitus (ST).
ST (also called somatosensory) is a subtype of subjective tinnitus, where altered somatosensory afference from the cervical spine or temporomandibular area causes or changes a patient’s tinnitus perception.
Since Levine’s first publication (1999), several animal and human studies have found connections between the somatosensory system of the cervical or temporomandibular area and the cochlear nuclei (CN), offering a physiological explanation for ST (Lanting, de Kleine, Eppinga, & van Dijk, 2010; S. E. Shore, 2011; Zhan, 2006). According to these studies, cervical or temporomandibular somatosensory information is conveyed to the brain by afferent fibers, the cell bodies of which are located in the dorsal root ganglia or the trigeminal ganglion. Some of these fibers also project to the central auditory system. This enables the somatosensory system to influence the auditory system by altering spontaneous rates or synchrony of firing among neurons in the CN, inferior colliculus or auditory cortex. In this way, the somatosensory system is able to alter the pitch or loudness of the tinnitus (S. Shore, Zhou, & Koehler, 2007).
Sanchez and Rocha (2011) proposed a set of diagnostic criteria to help recognizing patients with ST in clinical practice. According to these criteria, ST is suspected when the medical history shows at least one of the following: (a) evident history of head or neck trauma; (b) tinnitus association with some manipulation of the teeth, jaw, or cervical spine; (c) recurrent pain episodes in head, neck, or shoulder girdle; (d) temporal coincidence of appearance or increase of both pain and tinnitus; (e) increase in tinnitus during inadequate postures during rest, walking, working, or sleeping; and (f) intense bruxism periods during the day or night (Sanchez & Rocha, 2011). In addition, Sanchez and Rocha (2011) mention that ST often changes its loudness, pitch, or localization during stimulation in the head or neck region. Others (Biesinger, Groth, Hoing, & Holzl, 2015; Ward, Vella, Hoare, & Hall, 2015) state that the presence of this somatic modulation, through voluntary movements or specific resistance tests, is very important, if not the most important criterion, in diagnosing ST. These differences in diagnostic criteria might, at least partially, explain the large differences in prevalence of ST, which vary from 16% to 83% in different studies (Abel & Levine, 2004; Levine, Abel, & Cheng, 2003; Michiels, De Hertogh, Truijen, & Van de Heyning, 2015; Ralli et al., 2017; Simmons, Dambra, Lobarinas, Stocking, & Salvi, 2008; Ward et al., 2015; Won et al., 2013).
The lack of any agreed standards for clinical assessment make it unclear how to diagnose ST. Therefore, we aimed to reach a consensus on diagnostic criteria for ST among professional experts with current experience in assessing and managing ST. To reach this goal, we conducted a systematic review of the literature, followed by a modified two-round Delphi survey and a face-to-face meeting.
Methods
We used a Delphi process to gain consensus on a set of diagnostic criteria for ST among a panel of experts (scientists and clinicians). The Delphi technique, originally developed by the RAND Corporation, is a structured process that uses a series of questionnaires or rounds to gather and to provide information on a certain topic (Keeney, Hasson, & McKenna, 2001).
Systematic Review
Overview of the “Long List” of 41 Potential Diagnostic Criteria.
Modified Delphi Survey
Panel selection
Experts in ST were identified if they were a senior (i.e., first or last) author of an included publication that had been identified in the systematic review and were able to understand written English. Responsibility for conducting and managing the Delphi process was not an exclusion criterion for panel membership. In addition, those experts were each asked to recommend other ST experts from academic or clinical fields. This process identified 18 individual experts from 10 countries (Belgium, Brazil, France, Germany, Israel, Italy, Portugal, United Kingdom, South Korea, and United States) and 16 universities or hospitals. Of those, 15 agreed to participate in the Delphi panel. Two answered they did not feel confident enough with the subject to be part of the survey and one did not respond to the invitation.
The Delphi survey
The two-round Delphi survey was managed using Qualtrics® Survey Software to support the international reach of the study. Academic and clinical experts were pooled to create a single professional stakeholder group. To promote retention of panel members, each round was open for a short time (4 weeks) and the time between rounds was kept to a minimum (2 weeks). Response rates were regularly monitored, email reminders were sent to target individuals who had yet to complete the round.
In Round 1, 15 panelists were asked to evaluate the level of importance of each potential diagnostic criterion for ST from the long list. The order of items was fixed across rounds. Participants scored each outcome domain inspired by the GRADE scale of 1 to 9 (Guyatt et al., 2011). Scoring used a Likert-type scale with additional interpretation categories; 1 to 3 indicated that the item was not essential for diagnosing ST, 4 to 6 indicated it may be present, but not essential, and 7 to 9 indicated that it was essential. Unable to score was always an option. Participants were also able to suggest additional diagnostic criteria in a free-text comment.
In Round 2, those panelists who completed at least 80% of the Round 1 survey received the same long list, plus the additional items suggested by at least one panelist. Participants were presented with graphical feedback (a bar chart) to summarize the panel results from Round 1. The purpose of Round 2 was to enable the participants to reflect on their answers, taking into account the opinion of their peers, and to score the different items again. From Round 2, a recommendation for inclusion as a diagnostic criterion for ST was predefined as at least 70% of the panelists scored 7 to 9, and fewer than 15% scored 1 to 3. Conversely, a recommendation for exclusion was at least 70% of the panelists who scored 1 to 3 and fewer than 15% scored 7 to 9.
Consensus Meeting
The 14 panelists who completed Round 2 of the Delphi survey were invited to participate in a face-to-face consensus meeting that took place on March 13, 2018, prior to the Tinnitus Research Initiative Conference 2018 in Regensburg, Germany. A group of six clinicians or academic professionals with expertise on ST attended the meeting. The panel included three clinicians (one audiologist and two ear, nose, and throat [ENTs]) and three scientists (one neurologist, one ENT, and one physical therapist). Authors 1 to 5 served on this panel. The meeting lasted 3 h, and the discussion was semistructured according to the nominal group technique (Harvey & Holmes, 2012). Participants were encouraged to voice their opinions. All strongly dissenting opinions were considered.
The starting point for the consensus discussion was guided by the recommendations from the Delphi survey. First, participants were asked to consider those items where, after Round 2 of the survey, the recommendation was for exclusion as a diagnostic criterion for ST. The remaining items were individually discussed and voted for, with voting options being include or exclude. Again the predefined definition of consensus was for at least 70% of the participants to agree.
Results
Systematic Review
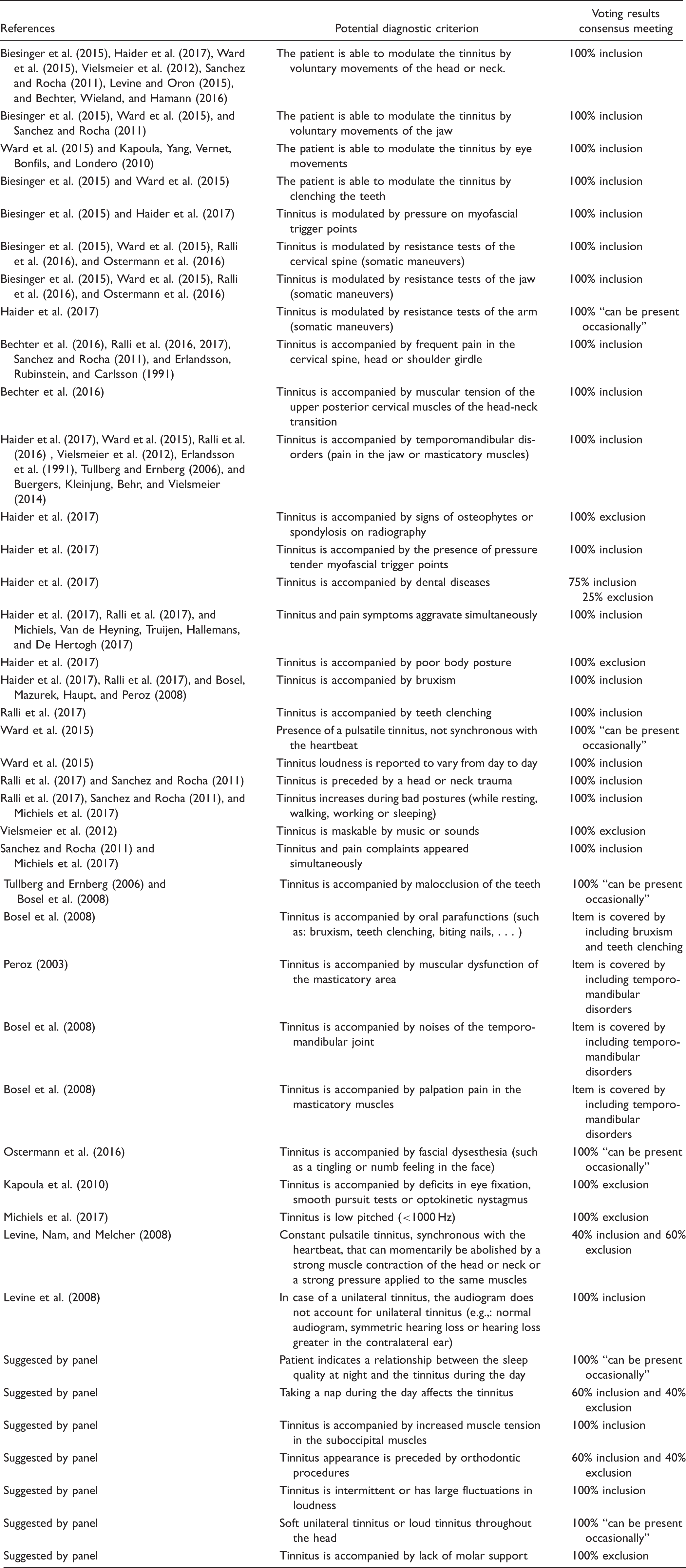
The search strategy identified 167 articles, of which 18 were eligible for inclusion. A detailed overview of the selection process is shown in Figure 1. Synthesis of the data extracted from those 18 articles related to patient assessment for ST yielded 34 potential diagnostic criteria. A list of these can be found in Table 1, along with references to the source of that information.
Overview of the inclusion process of articles in the systematic review.
Delphi Survey
Each round of the Delphi survey was open for 4 weeks, with 2 weeks in between both rounds.
Seven additional items were suggested by at least one panelist in Round 1 (see Table 1). These were added to Round 2 of the Delphi survey.
At the end of Round 2, scores for the expert panel indicated support for the inclusion of two diagnostic criteria since more than 70% of the Delphi panel members scored them 7 to 9 and fewer than 15% scored them 1 to 3 (see Table 1). Conversely, scores indicated the exclusion of six diagnostic criteria since more than 70% of the Delphi panel members scored them 1 to 3 and fewer than 15% scored them 7 to 9 (see Table 1).
Consensus Meeting
The intended goal of the meeting was to agree on a list of assessment criteria that should be present in every single patient receiving a clinical diagnosis of ST. At the start of the consensus meeting, participants urged caution that this goal would not be possible. The reasoning for this caution was that, according to their extensive clinical experience, individual patients with ST can present with a large set of different symptoms. As an alternative goal, the group instead agreed to provide a list of items that, if present, would strongly suggest an influence of the somatosensory system on the patient’s tinnitus.
The panel was first asked to consider those 2 items that had been identified as essential by the Delphi survey participants in Round 2 and 5 items that had been identified as not essential in Round 2. They agreed to, respectively, include the 2 and exclude the 5 presented items (100% agree). The remaining 34/41 items were then discussed and voted for (see Table 1 for details). In cases where at least four of the six participants voted for inclusion, a diagnostic criterion was added to the final assessment list.
Items on Tinnitus Modulation That, If Present, Strongly Suggest Somatosensory Influence of Tinnitus.

Tinnitus Characteristics That, If Present, Strongly Suggest Somatosensory Influence of Tinnitus.

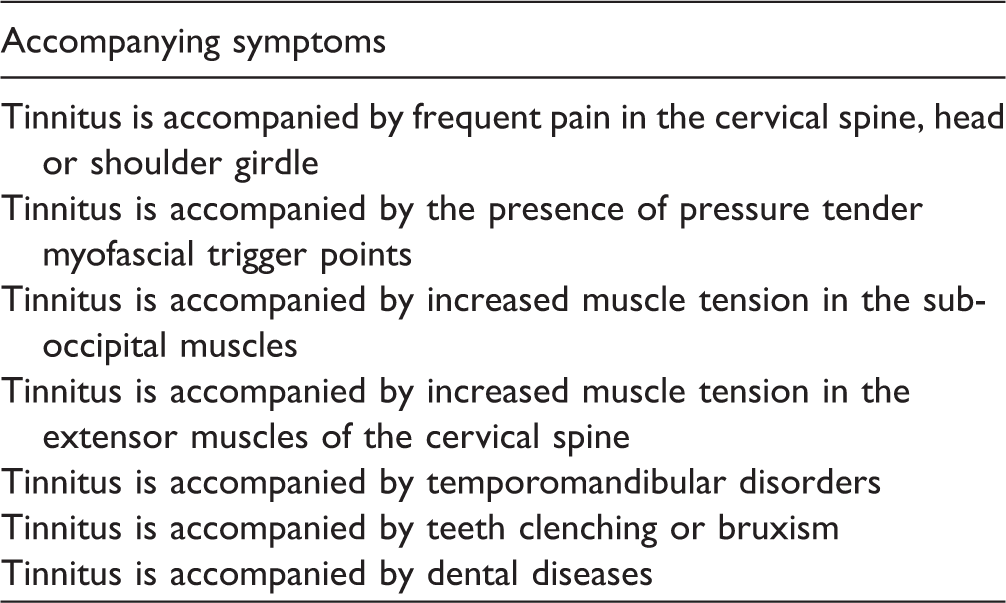
Accompanying Symptoms That, If Present, Strongly Suggest Somatosensory Influence of Tinnitus.
The second set of items (11/34 items) to be discussed were tinnitus characteristics that often exist in patients with ST. Items that were considered important to include were the simultaneous onset and aggravation of tinnitus and pain symptoms in the neck or jaw area, potentially preceded by a head or neck trauma. In addition, the increase in tinnitus during certain postures (such as bad posture during computer work or sleep) and the presence of variations in pitch, loudness, and location of the tinnitus were pointed out as items that strongly suggest ST. Another typical tinnitus characteristic is that, in case of a unilateral tinnitus, the audiogram does not account for a unilateral tinnitus. One item on this list a specific type of constant pulsatile tinnitus, synchronous with the heartbeat, that can momentarily be abolished by a strong muscle contraction of the head or neck muscles or by a strong pressure applied to the same muscles (Levine et al., 2008) caused a prolonged discussion. Due to dissenting views on this topic, there was no consensus (after voting) to either definitively include or exclude the item.
The third set of items (15/34 items) to be discussed were those symptoms that can accompany the patient’s tinnitus. Items that were considered important to include were frequent pain in head, neck, or shoulder girdle; temporomandibular disorders; pressure-tender myofascial trigger points in the head–neck region; increase in muscle tension in the neck extensor muscles; bruxism or teeth clenching; and dental diseases. The group agreed that whenever one or more of these symptoms are present, this strongly suggests an influence of the somatosensory system on the patient’s tinnitus.
In total, six items were identified as can be present in a single patient, but not systematically enough to be on the list of diagnostic criteria.
Discussion
This study aimed to reach an international consensus on diagnostic criteria for ST. Up until now, academics and clinicians have often used their own criteria to include patients in trials on ST. For the first time, experts in ST were gathered together to create a consensus statement about the diagnostic assessment of ST.
This consensus recommends aspects of tinnitus modulation, tinnitus characteristics (such as varying pitch and loudness), and accompanying symptoms that are strongly suggestive of ST in an individual patient while acknowledging that the individual presentation of the condition can vary from patient to patient.
In agreement with the diagnostic criteria given by Sanchez and Rocha (2011), the experts in ST agreed that rather than a definitive set of diagnostic features, clinical assessment should instead look for evidence of certain features that, if present, would strongly suggest an influence of the somatosensory system on the patient’s tinnitus. The list proposed in this consensus study confirms many of the same diagnostic criteria provided by Sanchez and Rocha (2011) but also adds some new items.
Implications of Our Findings for the Tinnitus Community
From the literature, many authors have diagnosed a patient with ST according to whether the patient could modulate the tinnitus by either voluntary movements or somatic maneuvers (Biesinger et al., 2015; Haider et al., 2017; Ward et al., 2015). Our consensus meeting panel recognized the importance of somatic modulation, especially by voluntary movements, for the ST diagnosis but added that the absence of this ability does not rule out ST. Hence, somatic modulation should not be used as a simple yes or no criterion for diagnosing ST. Although the use of somatic maneuvers to assess tinnitus modulation was voted in, some participants believed that the use of these maneuvers as a single criterion can potentially lead to overdiagnosis. For example, a study of Abel and Levine (2004) showed that not only were 83% of patients with tinnitus able to modulate their tinnitus through somatic maneuvers, but in addition, 65% of nonclinical healthy participants perceived a tinnitus-like sound during somatic maneuvers.
It must be noted that certain items, such as Tinnitus accompanied by frequent pain in the head, neck or shoulder girdle or Tinnitus accompanied by temporomandibular disorders, should be used with a certain prudence if they are the only criterion present in a patient. This is because tinnitus and neck or jaw problems can also co-occur without a causal relation (Michiels et al., 2015). On the other hand, when these items are combined with another criterion, such as Tinnitus and neck or jaw pain complaints appeared simultaneously or The patient is able to modulate the tinnitus by voluntary movement of the head, neck, jaw or eyes, the ST diagnosis gets stronger.
Strengths and Limitations of the Study
Our Delphi survey was completed by a relatively small number of experts, which might have influenced the decision-making. On the other hand, we were able to identify only 18 potential ST experts in our literature search, of which 14 (78%) completed both rounds. We would have liked to have all of them in our consensus meeting, but unfortunately only six were able to attend the meeting. Because there was no financing for this study, we decided to host the consensus meeting prior to the tinnitus research initiative conference to enable as many of our experts as possible to attend this meeting without extra travel costs. Several panelists, however, had other engagements at the time of the meeting. Although a larger sample of consensus meeting panelists would have been preferred, a representative sample of ST experts, from four different countries and six different institutions, was present at the meeting. This is far more than in most consensus meetings in larger scientific fields.
The multifactorial causes of tinnitus in most patients can probably explain the differences in experience. The panel members agree that cases where the somatosensory system is the main cause of the tinnitus exists but are rare. On the other hand, a large group of patients have secondary somatosensory influence on their tinnitus to a certain degree. This somatosensory influence can be combined with other influences such as increased stress levels, anxiety, or depression. All these influences can also increase a tinnitus that is strongly associated by auditory deafferentation, such as noise exposure.
Future Research Directions
Although the item concerning presence of a constant pulsatile tinnitus, synchronous with the heartbeat, reached no consensus for either in- or exclusion, the group advised that the examiner should keep in mind that in some cases such a pulsatile tinnitus can be affected by somatic maneuvers. Further research is, however, needed to describe the characteristics and treatment opportunities for these patients.
Now that a set of criteria to recognize ST is agreed upon by an international panel of ST experts, clinicians can use these criteria to determine the extent to which the somatosensory system influences an individual patient’s tinnitus. ST should not be seen as a specific category of tinnitus, but more as a factor that can influence a patient’s tinnitus in a larger or smaller degree.
The next step should be to find the most effective treatment for patients with ST. It must be noted that this most effective treatment might not be the same for all patients with ST. As in all musculoskeletal conditions, the most appropriate treatment is often a combination of treatment modalities tailored to the individual patient’s needs. Since psychological factors, such as stress, anxiety, and depression, influence both tinnitus and neck or jaw problems, it might also be interesting to investigate the effect of a combined treatment comprising physical therapy modalities and psychological techniques on tinnitus severity in future studies.
Conclusion
This study used an international Delphi survey and consensus meeting to agree upon a set of criteria that strongly suggest ST. Because of the international nature of the survey, we expect these criteria to gain a wide acceptance in the research field and to serve as a guideline for clinicians. The criteria developed in this consensus paper now allow to further investigate the extent of somatosensory influence in individual tinnitus patients and tinnitus populations.
Footnotes
Acknowledgments
The authors would like to thank everyone who worked with them on this Delphi survey and consensus meeting and the TRI-organizing team for the practical organization of our consensus meeting.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author is supported by a research grant from the ‘Fonds voor wetenschappelijk onderzoek Vlaanderen’ (FWO; T001916N). No specific funding for this Delphi study and face-to-face meeting was received.