
Abstract
This study focuses on the development of a profiling system to specify the needs of hearing-aid candidates. As a basis for the profile of compensation needs, we used a slightly modified version of the Amsterdam Inventory of Disability and Handicap, combined with the well-known Client-Oriented Scale of Improvement (COSI). The first questionnaire results in scores for six audiological dimensions: detection, speech in quiet, speech in noise, localization, focus or discrimination, and noise tolerance. The goal of this study was to determine whether the six dimensions derived from the disability questionnaire are appropriate to also categorize individual COSI targets. The results show a good agreement between eight audiologists in the categorization of COSI goals along the six dimensions. The results per dimension show that the dimension focus or discrimination can be regarded as superfluous. Possible additional dimensions were tinnitus and listening effort. The results indicate that it is possible to translate individual user needs (administered using COSI) into more general dimensions derived from a disability questionnaire. This allows to summarize the compensation needs for individual patients in a profile of general dimensions, based on the degree of disability and the individual user needs. This profile can be used as a starting point in hearing aid selection. This approach also offers a well-structured method for the evaluation of the postfitting results.
Introduction
Despite the huge number of hearing aids available on the market and the different options in terms of functionality, there is lack of a systematic approach for how to select specific hearing-aid models or at least functionalities that may contribute to an optimal compensation of hearing loss. Although diagnostic data from pure tone audiometry and speech audiometry are essential for fitting a hearing aid once selected, their role in the selection of a hearing aid itself is limited. Of course, the audiogram provides some information about the degree of gain and acoustic output levels needed and in some cases also about the style of hearing aid. However, as most hearing-aid models are appropriate for a wide range of audiograms, easily covering 50% to 80% of the audiograms in a representative audiological clinic, it is clear that the audiogram is not the only information relevant for hearing aid selection. Selection can be refined by preferences about size, design, and operational issues such as volume controls, connectivity, and options for tinnitus masking and (bi)CROS-units. But there are no systematic tools available to consider other signal-processing functionalities, despite the commercial claims that these functionalities may better distinguish between hearing aids than, for instance, the degree of gain.
To select the appropriate processing features for an individual, we need additional information about the limitations experienced by the hearing-impaired client in daily life without hearing aids or with their old hearing aids (prefitting). The largest disabilities are not necessarily those that the listener primarily wishes to solve. Therefore, it is useful to draw up an inventory that combines the disabilities experienced by the hearing-impaired listener as well as the individual objectives for rehabilitation.
Several validated questionnaires for investigating hearing disabilities are available in clinical practice and audiological research, for example, Amsterdam Inventory of Disability and Handicap (AIADH; Kramer, Kapteyn, Festen, & Tobi, 1995), Abbreviated Profile of Hearing Aid Benefit (Cox & Alexander, 1995), Client-Oriented Scale of Improvement (COSI; Dillon, James, & Ginis, 1997), Glasgow Hearing Aid Benefit Profile (Gatehouse, 1999), International Outcome Inventory for Hearing Aids (Cox et al., 2000), and Speech, Spatial, and Qualities (Gatehouse & Noble, 2004).
We intended to develop a profiling system that allows us to summarize the compensation needs of individual patients along general audiological dimensions that can be related to hearing aid properties. For this purpose, we compared existing questionnaires on the following requirements: (a) the questionnaire should be applicable as for preassessments and postassessments, (b) the number of questions should not be too high, (c) the results should be expressed as dimensions relevant for hearing aid selection, and (d) the instrument should provide a combination of general issues and more individualized issues. Although not the only possibility, we have selected to use AIADH and COSI and combined them into an integrated approach.
Disabilities Experienced by the Hearing-Impaired Listener: AIADH (or AVAB)
List of Dimensions That Are Derived From the AVAB Questionnaire to Inventory “General” Disabilities.

Note. AVAB = Amsterdam Questionnaire for Auditory Disabilities.
Individual Objectives for Rehabilitation: COSI
An important disadvantage of a questionnaire such as the AVAB is that it evaluates a fixed list of common listening situations, which may not be the situations that are the most relevant for a given patient. As an alternative for questionnaires with fixed situations, Dillon et al. (1997) proposed the COSI for the evaluation of hearing aids, in which patients are asked to define their own targets for rehabilitation. During the first visit, up to five situations are specified in which the patient would like to cope better. After a period of hearing-aid use, the patient assesses whether the targets have been met. In this way, the COSI helps the clinician to perform the usual assessment of identification of problems in a well-structured way and to identify those problems that are particularly relevant for the individual listener.
List of COSI Dimensions Proposed by Dillon et al. (1997) (First Column), the Percentages of Subjects Mentioning These Issues (Second Column, According to Dillon et al. 1997), and the Dimensions of the AVAB Profile That Are Associated With These COSI Dimensions.

Note. COSI = Client-Oriented Scale of Improvement; AVAB = Amsterdam Questionnaire for Auditory Disabilities.
Combining AVAB and COSI
As an alternative for the 16 categories proposed by Dillon et al. (1997), the 6 dimensions of the AVAB might be useful. As an example, column 3 of Table 2 illustrates a possible association between the 16 COSI dimensions and the dimensions of the AVAB profile.
If this approach proves to be applicable, individual hearing disabilities and individual compensation targets can be compared along the same dimensions and can be taken together in a six-dimensional profile summarizing the compensation needs of listeners. These dimensions cover a broad range of important auditory functionalities and can be informative in the choice of specific hearing aid functions. An advantage of using the same dimensions for AVAB and COSI is that, when using both AVAB and COSI, the COSI can help the interpretation and weighting of the AVAB results. For instance, if the AVAB reveals poor performance on one aspect, but COSI shows that this aspect is not relevant for the patient, this might not be the aspect that requires most attention in the selection of hearing aids or hearing aid functionalities. If categorization of the COSI targets can be done in a reproducible way, COSI is a valuable tool in the hearing aid prescription and evaluation process, both for clinical practice and research purposes, by being individual and general at the same time.
Goal of the Study
The goal of this study was to determine whether the six categories defined by the AVAB disability profile are appropriate to also categorize individual COSI targets. The two primary aspects of this question are (a) whether the interobserver agreement between clinicians is sufficiently high and (b) whether categories are regarded as missing or superfluous.
Methods
COSI Targets From Hearing-Aid Candidates and Hearing-Aid Users
The COSI targets used in this study were administered during regular clinical practice in the Audiological Center of the Academic Medical Center. A total number of 533 COSI targets were collected from 151 consecutive patients who visited the clinic in Fall 2014 and early 2015 for hearing aid fitting. During the first visit, pure tone audiometry, speech audiometry, AVAB questionnaire, and COSI questionnaire were administered and documented. Of these 151 patients, 103 patients were new hearing-aid users and 48 patients already had a hearing aid. Data were gathered retrospectively from the database; thus, patients and clinicians were not aware of the purpose of this study during administration of the targets. Personal information was removed to make the data anonymous.
Observers
Eight professional audiologists (six clinical physicists in audiology and two hearing aid dispensers) participated in this study. There was a wide range in experience administering the AVAB and COSI. For the purpose of this study, this was regarded to be an advantage. If inter-observer correspondence is not dependent on the level of experience, we may assume that the categorization of COSI targets is robust.
Test Procedure
Participating audiologists received a file with the 533 COSI targets and a user interface for categorization, accompanied by written instructions. To make sure that they understood what was meant by the six categories mentioned in Table 1, they first got the possibility to read all AVAB questions sorted by category. Then, they confirmed that they understood the categories and started the categorization procedure.
A user interface showed one COSI target at one time and presented two questions to be answered for each of the targets:
The first question was which AVAB category best describes the COSI target. Only one category could be assigned in the first question, and observers were forced to make a choice. However, apart from the six categories, there was an option not possible to categorize for targets that did not fit well in one of the categories. The second question was whether additional categories were required to describe the COSI target. Observers were allowed here to add one or more categories, if this was judged to be relevant for the categorization of the COSI target.
Audiologists were allowed to stop at each moment and continue at a later moment from the point they stopped. After categorizing all the 533 targets, the audiologists had the possibility to indicate whether they found the classification feasible, whether they missed categories, or whether they perceived categories as superfluous. Finally, they had the possibility to provide additional remarks.
Results
The Primary Dimension
Figure 1 indicates the distribution of all judgments (8 Observer × 533 COSI targets) regarding the primary dimension. Speech perceptions in noise and in quiet were the dimensions most frequently used as primary dimensions. In about 11% of the cases, the audiologists select the option not possible to categorize (indicated as other). Some examples of COSI targets that did not match the six dimensions were as follows: “To reduce the annoyance from my tinnitus” or “Less problems with feedback.” In other cases, the COSI targets were categorized as other, if the target was not specified in enough detail, for example, “Communication with others,” “Safety in my job,” or “Less miscommunication at home.” Figure 1 also indicates that the patterns of distribution are very similar for new users and experienced users. Figure 2 shows the number of COSI targets that were classified identically into the same primary dimension by the eight audiologists (first bar) or less (other bars). The audiologists had full agreement for the majority of COSI targets (296 out of 533).
Distribution of categories for the primary dimension, split for new users (left-hand bars; n = 103), and experienced users (right-hand bars; n = 48). COSI targets that did not match one of the six dimensions were categorized as “other.” Histograms indicating the percentages of COSI fitting targets that were indicated to the same category by eight audiologists (left-hand bar) or less (other bars).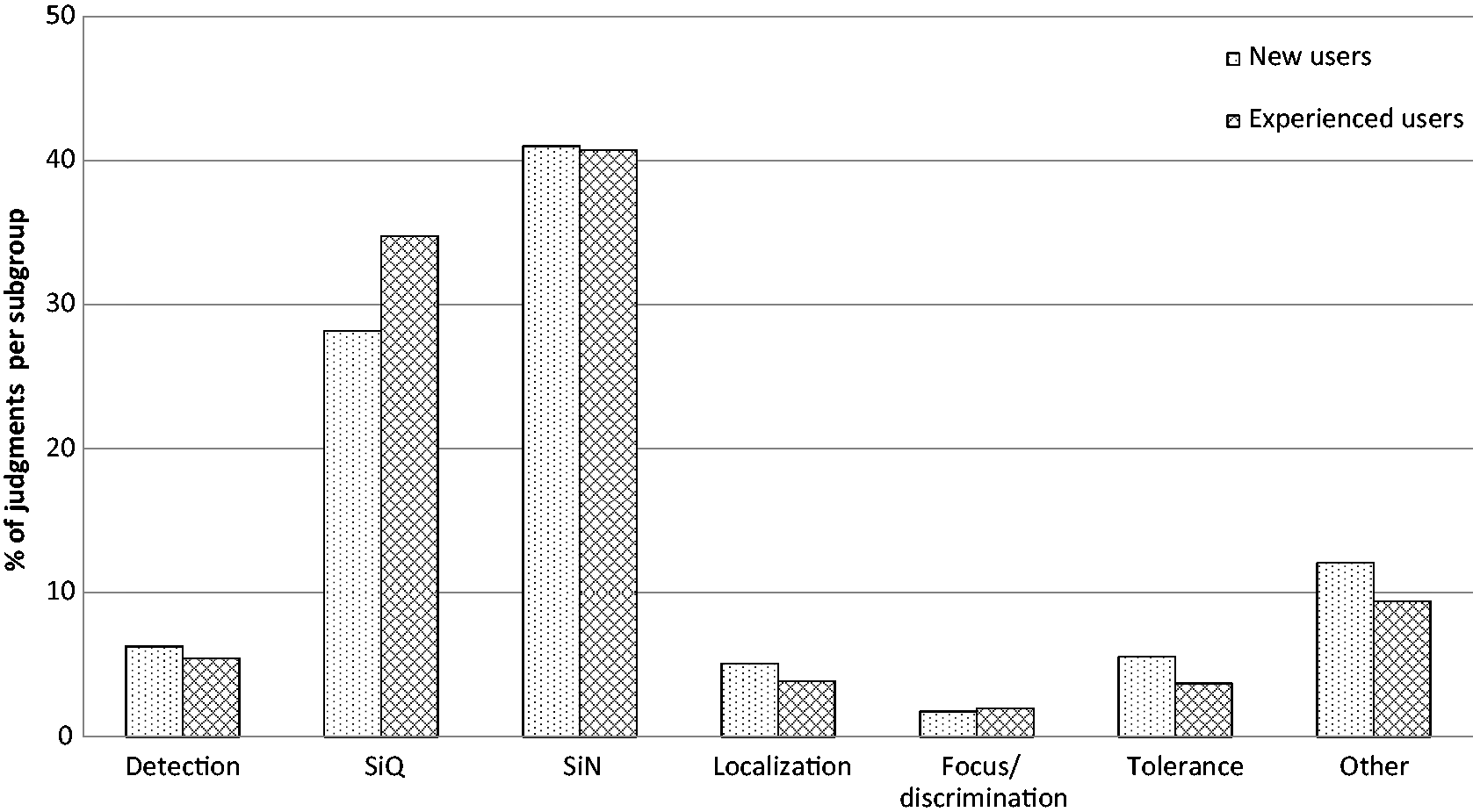

As a metric for interobserver correspondence, we calculated Cohen’s κ (Cohen, 1960). If we include all dimensions into the analysis, Cohen’s κ was .81. This may be considered as a substantial agreement (Landis & Koch, 1977). We also used two other measures for interobserver agreement such as Fleiss’ κ (Fleiss, 1971) and Gwet’s Agreement Coefficient 1 (Gwet, 2008) and found comparable results, both for the analysis of all dimensions and for subanalyses of separate dimensions (Figure 3). The analyses of the individual dimensions revealed that the correspondence in the categorization of the dimension focus or discrimination between audiologists was only weak to fair.
Metrics for inter-observer correspondence, calculated overall, and for the individual dimensions.
The Use of Additional Dimensions
As indicated, the second question for each target was whether additional dimensions were required to categorize the COSI target. Figure 4 shows that some of the audiologists used only the primary dimension in the majority of cases (e.g., Observers 2, 3, 4, and 8), while others frequently used two, three, or even more dimensions. Further analysis indicated that the combinations of dimensions that occurred most frequently are as follows:
Speech in quiet and speech in noise (for 38% of the cases where speech in quiet was selected as primary dimension and speech in noise was selected as additional dimension and for 35% of the cases where speech in noise was selected primarily and speech in noise was added as secondary dimension) Detection and localization (for 25% of the cases where detection was selected as primary dimension and localization was selected as additional dimension and for 38% of the cases where localization was selected primarily and detection was added as secondary dimension) Detection and focus or discrimination (for 15% of the cases where detection was selected as primary dimension and focus was selected as additional dimension and for 38% of the cases where focus or discrimination was selected primarily and detection was added as secondary dimension) Distribution of the number of selected dimensions per target for each audiologist.

Missing Dimensions
At the end of the session, the audiologists had the possibility to indicate whether they found the classification feasible, whether they missed categories, or whether they perceived categories as superfluous. Tinnitus was mentioned as a missing dimension by five of the eight audiologists. Other dimensions that were missing were related to speech from a distance, listening effort, music and sound quality, and the perception of loud sounds. On the other hand, focus or discrimination was indicated to be more or less superfluous.
Discussion
In this study, we found a good agreement between eight audiologists in the categorization of individually defined COSI goals into the six general AVAB dimensions and an additional category others. The agreement was very high, given the fact that the observers reported that some targets are not specific enough and that some targets do not fit well into one or more of the six dimensions. We also have to consider that the metric for interobserver correspondence was based on the choice of the primary dimension. Several COSI questions can be related to two or more dimensions, and in some of those cases, the choice of the primary dimension may be somewhat arbitrary. Even then, interobserver correspondence was found to be good, except for “focus/discrimination” as the primary dimension. The dimension focus or discrimination was identified as being superfluous. This dimension was selected as the primary dimension in less than 2% of the judgments. Among these 2%, in the majority of cases, the focus or discrimination dimension was selected by only one of the audiologists.
One factor reported to make categorization difficult was that several goals were not formulated sufficiently specifically. We collected the COSI goals retrospectively and the clinicians who administered the goals were not aware that the goals were going to be used for this purpose. For clinical practice, the short notes might have been sufficient, but for audiologists not knowing the patients and situations, goals such as “safety in my job” might contain insufficient information. The need for categorization of goals during clinical practice may encourage clinicians to ask supplementary questions in order to be able to categorize the goals well.
Zelski (2000) evaluated the agreement between three observers in categorizing COSI goals into the 16 categories defined by Dillon et al. (1997) and found a Cohen’s κ of 0.75, indicating substantial agreement. Our results suggest that categorization into the six AVAB dimensions results in comparable or even higher agreement than in the 16 dimensions defined by Dillon et al. (1997).
The study should be considered as a first step in designing user profiles for hearing aid selection. The results yielded some suggestions to combine dimensions and to add new ones. This study shows that at least five of the six dimensions tested are feasible. Future research is needed to decide whether these five dimensions can be extended with new dimensions, for example, tinnitus amelioration and listening effort. However, despite this room for improvement in the future, the study also indicates that COSI targets can be expressed reasonably well along the same dimensions as the disability profile defined by AVAB. This allows us to combine AVAB and COSI in a profile of compensation needs. Whereas AVAB yields a profile of disabilities in six dimensions, COSI can now be used as a weighting factor for the importance of the different dimensions.
This allows that for each subject, the patterns of (general) disabilities (derived from AVAB) and the patterns of (individual) needs (derived from COSI) can be combined into an integrated compensation profile. In the future, there are three major areas where such a compensation profile can be supportive:
Support in Hearing Aid Selection
The compensation profile is a means that can be helpful in the selection of hearing aids and hearing aid functionalities. The overall degree of compensation needs, represented by the sum of (weighted) AVAB scores, may be related to the minimum level of technology that is required for an adequate compensation. In addition, the profile of the compensation needs indicates which aspects deserve special attention in the selection process.
To support selection of an appropriate hearing aid based on the profile of compensation needs, hearing aid characteristics can be inventoried in hearing-aid-specific profiles, describing the potential for compensation of the hearing aid with respect to the same dimensions. For instance, a high compensation need for detection requires flexibility in amplification, but it may also require frequency transposition. A strong need for compensation for speech in noise might be an indication for the use of directionality, and a strong need for compensation for noise tolerance might indicate the need for noise reduction.
Support in Evaluation of Individual Benefit
The profiles provide a well-structured basis for the evaluation of the postfitting situation. Both AVAB and COSI can be used for pre–post comparisons. AVAB provides postfitting scores on the same dimensions as prefitting, so that the effect of the newly fitted hearing aid can directly be compared along these axes. This provides a quick overview for which dimensions the newly fitted hearing aids provide sufficient improvement and which dimensions need more attention. The COSI supports in showing which AVAB dimensions are particularly important for the individual user and also allows postfitting evaluation about the degree of change and the final ability for the individually formulated targets. Both components of evaluation form a good combination by being individual (COSI) and general (AVAB) at the same time.
Support in Collecting Practice-Based Evidence
If applied on a large scale, a profiling system may be able to collect knowledge for better hearing aid selection. The system can be used to collect practice-based evidence that may reduce the lack of evidence-based practice in hearing aid selection in current fitting practice. These data can be used to educate the clinicians more about the degree of benefit that is realistic for different groups of subjects. This knowledge will also support the aforementioned postfitting evaluation. In addition, knowledge about the relationships between the user profiles and hearing aid properties as suggested earlier can be used to update the profiling system and the coupling between the compensation needs of a patient and the compensation abilities of hearing aids.
Conclusions
This study provides a way to translate individual patterns of user needs (administered using COSI) into more general dimensions derived from a disability questionnaire (AVAB). This allows to summarize the compensation needs in general dimensions for each client, based on the degree of disability and the individual user needs. The results indicate that at least five dimensions can be reliably used for categorization of COSI targets. The focus or discrimination dimension was rarely used and showed low agreement between observers. Therefore, this dimension should be excluded. Possible additional dimensions are tinnitus amelioration and listening effort. Categorization of COSI targets in addition to the AVAB questionnaire can be used as a starting point in hearing aid selection. This approach also offers a thorough method for the evaluation of the postfitting results. Finally, if applied on a large scale, the approach could be used to collect practice-based evidence for the effect of hearing-aid use on the profile dimensions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.