
Abstract
Background:
Lumbar disc herniation (LDH) represents a frequent cause of low back and lower limb pain in elite athletes, and is associated with abstention from sports activities and impaired quality of life.
Purpose:
To comparatively evaluate the visual analog scale (VAS) and Short-Form 36 (SF-36) Health Survey Questionnaire in elite athletes subjected to transforaminal endoscopic lumbar discectomy (TELD) versus conventional microdiscectomy for surgical management of LDH.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 62 elite athletes diagnosed with LDH were classified into 2 groups based on the performed intervention: microdiscectomy (Group A, n = 28 patients) or TELD (Group B, n = 34 patients). The procedure selected was based on the anatomic location of LDH. The primary outcome measure was the VAS score for lower limb pain (VAS-LP), while the secondary outcome measures were the VAS score for low back pain (VAS-BP), the SF-36 questionnaire for quality-of-life assessment, and hospitalization duration, return-to-play time, and complications. All outcome measures were evaluated at determined intervals during a 3-year follow-up analysis.
Results:
Baseline descriptive data were similar between the 2 groups. VAS-BP values were significantly higher in Group A throughout the entire follow-up. In contrast, VAS-LP and the overwhelming majority of SF-36 scores were significantly ameliorated in Group B at most follow-up checkpoints. Hospitalization duration and return-to-play time were significantly less in Group B, while the rate of return-to-play was 100% in both groups. No major perioperative complications were observed in either group.
Conclusion:
TELD represents a safe and effective alternative for the surgical management of LDH in elite athletes and may offer advantages over conventional microdiscectomy, primarily related to its minimal invasiveness. However, meticulous patient selection and the assessment of patients’ expectations are of critical importance to identifying patients suitable for the TELD procedure, given the relative inadequacy of such data in the literature to date.
Keywords
Lumbar disc herniation (LDH) represents a frequently encountered entity in current clinical practice. Recent epidemiologic data suggest that its incidence ranges from 2% to 3%. LDH is a major cause of chronic low back and lower limb pain with a remarkably negative impact on the quality of life of affected individuals.5,14 Surgical management is reserved for patients with drug-resistant sciatica or progressive neurologic deficit on the grounds of referable imaginary findings. To address this condition, a variety of surgical techniques have been performed, ranging from simple removal of protruding disc fragments (sequestrectomy) to removal of disc material in the intervertebral space under surgical microscope magnification (conventional microdiscectomy), and, more recently, removal of symptomatic fragments using full-endoscopic techniques. 5
Low back pain (LBP) is a common symptom among adult athletes, affecting >30% at some point in their careers. 20 The vast majority of these cases are presented with pain of nonspecific origin in outpatient clinics, indicating the multifactorial nature of the symptom. 21 In the setting of specific structural causes, LDH represents a frequent finding and underlying cause, with reported rates of symptomatic LDH reaching up to 75% among elite athletes, being generally greater than the nonathlete population.20,24 The increased rates can be justified by the fact that these individuals consistently subject their bodies to extreme strain, pushing their physical limits to the maximum.12,24 Sports that subject the spine to extreme torsion, shear, flexion, and compression forces are more likely be associated with LDH clinical emergence. 22
Elite athletes represent a unique patient category within the general population, primarily due to high and competing demands, the necessity for rapid rehabilitation with return to play (RTP), and, importantly, return to the previous level of athletic performance. 14 When it comes to surgical management, the selected method should be as minimally invasive as possible to avoid disruption of the posterior musculature and osseoligamentous structures’ functionality.10,11 Nevertheless, experienced LBP may be attributed to several factors, such as facet joint, vertebral endplate, disc, and nerve root functional compromise. Hence, proper clinical examination in conjunction with meticulous evaluation of imaginary findings is necessary to identify the source of pain and identify patients with LDH who may benefit from surgical intervention. 10
Despite the documented particularities and high-level requirements in the management of elite athletes with LDH, the treatment algorithm remains unclear in the current literature.8,18,22 Microdiscectomy and transforaminal endoscopic lumbar discectomy have both been described in the existing literature for the surgical management of LDH in elite athletes, with distinct outcomes on postoperative pain levels, athletes’ quality of life, RTP time, and risk of LDH recurrence.14,19,26,27 However, precise comparative data about the functional outcome of these techniques for the management of LDH in this category of athletes remain scarce in the current literature.
Hence, this study aimed to investigate the role of endoscopic lumbar discectomy versus conventional microdiscectomy in the surgical management of LDH in elite athletes, with a particular focus on exploring the theoretically favorable effect of endoscopic discectomy in reducing visual analog scale-limb pain (VAS-LP) and improving functionality in these patients. Study design, selection of elite athletes, and follow-up duration underline the originality of our investigation in the general literature framework.
Methods
Study Population and Approval
All participants enrolled in this study were diagnosed with LDH in accordance with clinical and radiological criteria, fulfilling current indications for discectomy. All operations were performed by the same experienced minimally invasive and endoscopic spine surgery surgeon (S.K.), conducted at the same tertiary center. All participants were thoroughly informed of the study's structure and purpose and provided written consent to participate. The rights of all patients were fully protected throughout their participation in this study. This study received approval from the institutional review board of our hospital (Approval No.: 1712/14.04.2022). Moreover, all aspects of the study fully adhered to the ethical principles outlined in the Declaration of Helsinki (1975 and its 2000 revision).
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) elite athletes aged 18 to 30 years; (2) symptomatic traumatic single-level LDH confirmed by magnetic resonance imaging of lumbar spine; (3) LBP with severe radiculopathy (drug-resistant radicular pain in exiting nerve root distribution over 6 weeks); (4) positive nerve root tension sign; and (5) neurological deficit (motor or sensory).
The exclusion criteria were as follows: (1) sequestered disc hernia; (2) previous surgery at the affected level or recurrent herniated disc; (3) segmental instability or spondylolisthesis; (4) vertebral fracture; (5) spinal tumor or infection; and (6) presence of associated comorbidities and morbid habits (smoking, alcohol consumption).
Methods
All participants were elite athletes, as defined by Swann et al, 25 demonstrating symptomatic LDH, which was surgically treated either with microdiscectomy or endoscopic lumbar discectomy. Overall, there were 2 patient groups based on the surgical technique used (Group A, microdiscectomy; Group B, transforaminal endoscopic lumbar discectomy [TELD]). The standard posterior approach at the affected lumbar spine level was applied to patients who underwent microdiscectomy. 15 In contrast, the transforaminal approach (via the Kambin triangle) was used for patients who underwent full-endoscopic discectomy (TELD). 14 The anatomic location of LDH was the primary characteristic that determined the performance of a particular surgery type. Central and paracentral disc herniations were managed via microdiscectomy, while foraminal and extraforaminal disc herniations were treated via TELD.
All patients underwent surgical treatment from May 2018 to May 2022. Demographic characteristics of patients in each group were retrospectively analyzed. The primary outcome was the VAS score for evaluation of lower limb pain (VAS-LP). In contrast, secondary outcomes included the VAS score for LBP (VAS-BP), the Short-Form 36 (SF-36) Medical Health Survey Questionnaire (for Health-Related Quality of Life (HRQoL) analysis), length of hospitalization, RTP time, and overall complications. Assessment was performed preoperatively and at 1, 2, 3, 4, 6, 8, 12, 24, and 36 months postoperatively.
Postoperative Rehabilitation Protocol
All enrolled participants were subjected to the same rehabilitation protocol postoperatively by the same experienced physical therapist in our department. Patients were encouraged to mobilize using a lumbar orthosis for the first 6 weeks, received analgesics (paracetamol, opioids) as needed, and began physical therapy sessions after the 15th postoperative day. The implemented protocol included exercises targeting neural mobilization, core stabilizers (transverse abdominis and quadratus lumborum), lower-limb muscle strengthening (primarily superior gluteal and quadratus femoris, with specific emphasis on affected muscles in cases of neurologic deficit), and proprioception exercises. RTP timing was determined after a thorough discussion between our department's physical therapist and the athlete's head coach.
Visual Analog Scale
The VAS is an applicable method for assessing pain intensity. All patients participating in this study were asked to mark their subjective pain level at each follow-up interval, separately for lower limb pain (VAS-LP) and LBP (VAS-BP). A 100-mm horizontal line was used in this study. A minimally clinically important difference (MCID) was defined as 9 mm. 16 Other parameters—including sex, age, and pain cause—were not considered as separate variables in the analysis.16,17
SF-36 Medical Health Survey Questionnaire
The SF-36 Medical Health Survey Questionnaire is a widely recognized tool for assessing HRQoL after spine surgery. This questionnaire comprises 36 items assessing 8 key parameters that reflect patients’ overall health: physical function (PF), role physical (RP), bodily pain (BP), general health (GH), energy, fatigue and vitality (V), social function (SF), role emotional (RE), and mental health (MH). However, no specific MCID currently exists for this tool in evaluating patients with LDH. Each patient was required to complete the questionnaire at each follow-up assessment. Upon gathering all responses, percentage-based scales were generated, with higher scores generally indicating better HRQoL. Questionnaires with <50% of responses completed were considered invalid. 30
Statistical Analysis
Collected data were analyzed with SPSS, Version 24 (IBM Corp). Continuous variables were expressed as the mean ± standard deviation, and categorical variables as percentages. The Kolmogorov-Smirnov test was used to assess normality. The Mann-Whitney U test was used to compare continuous variables in our independent samples, for non-normal distribution, in a population divided into 2 categories. The Kruskal-Wallis test was used to compare continuous variables in our independent samples, with non-normal distributions, in a population divided into >2 categories. The t test was used to compare continuous variables in our independent samples, for a normal distribution. Pearson's chi-square (cross-tabulation) was used to compare categorical variables. The LogRank test was used to compare the intervention's success distribution over time across≥2 categories in a population. The level of significance was set at P = .05.
Results
General Data and Demographics
A total of 62 patients (elite athletes) diagnosed with LDH were classified into 2 groups based on the implemented surgical procedure. Group A included 28 patients who underwent microdiscectomy, while Group B included 34 patients who underwent TELD. All patients successfully completed the 3-year follow-up period (Figure 1).

Representation of the study CONSORT flow chart. CONSORT, Consolidated Standards of Reporting Trials; TELD, transforaminal endoscopic lumbar discectomy.
The mean age of patients was 25.1 ± 3.7 years in Group A and 24 ± 3.6 years in Group B. Baseline demographic characteristics, such as age, body mass index, LDH location, and type of sport, were not statistically significantly different between groups. Basketball was the most common sport in both groups, followed by volleyball. Furthermore, the L4-L5 segment was primarily affected, and, incidentally, no patients with L5-S1 herniation were encountered. The demographic characteristics of patients are presented in Table 1.
Patient Characteristics a

Data are presented as mean ± SD or n (%). BMI, body mass index; L, lumbar vertebra; TELD, transforaminal endoscopic lumbar discectomy.
VAS Score Assessment
Regarding the VAS-LP score, preoperative VAS-LP values were 84.6 ± 5.1 for Group A and 85 ± 5.1 for Group B, while respective VAS-BP values were 54.6 ± 5.1 for Group A and 54.7 ± 5.1 for Group B. No statistically significant differences were found for either variable. The VAS-BP showed a statistically significant difference between the 2 groups at each follow-up interval, favoring Group B, with quantitative differences of 1.94 points at the 6- and 24-month assessments, respectively (P < .001). Conversely, minimal quantitative deterioration of values in each group over the 36-month interval was not statistically significant (Figure 2, Appendix Table A). Additionally, VAS-LP values were statistically significantly lower in Group A during the early postoperative period (1 month), with this finding reversed after 4 months postoperatively, when values were statistically significantly higher in Group B (Figure 3, Appendix Table A).
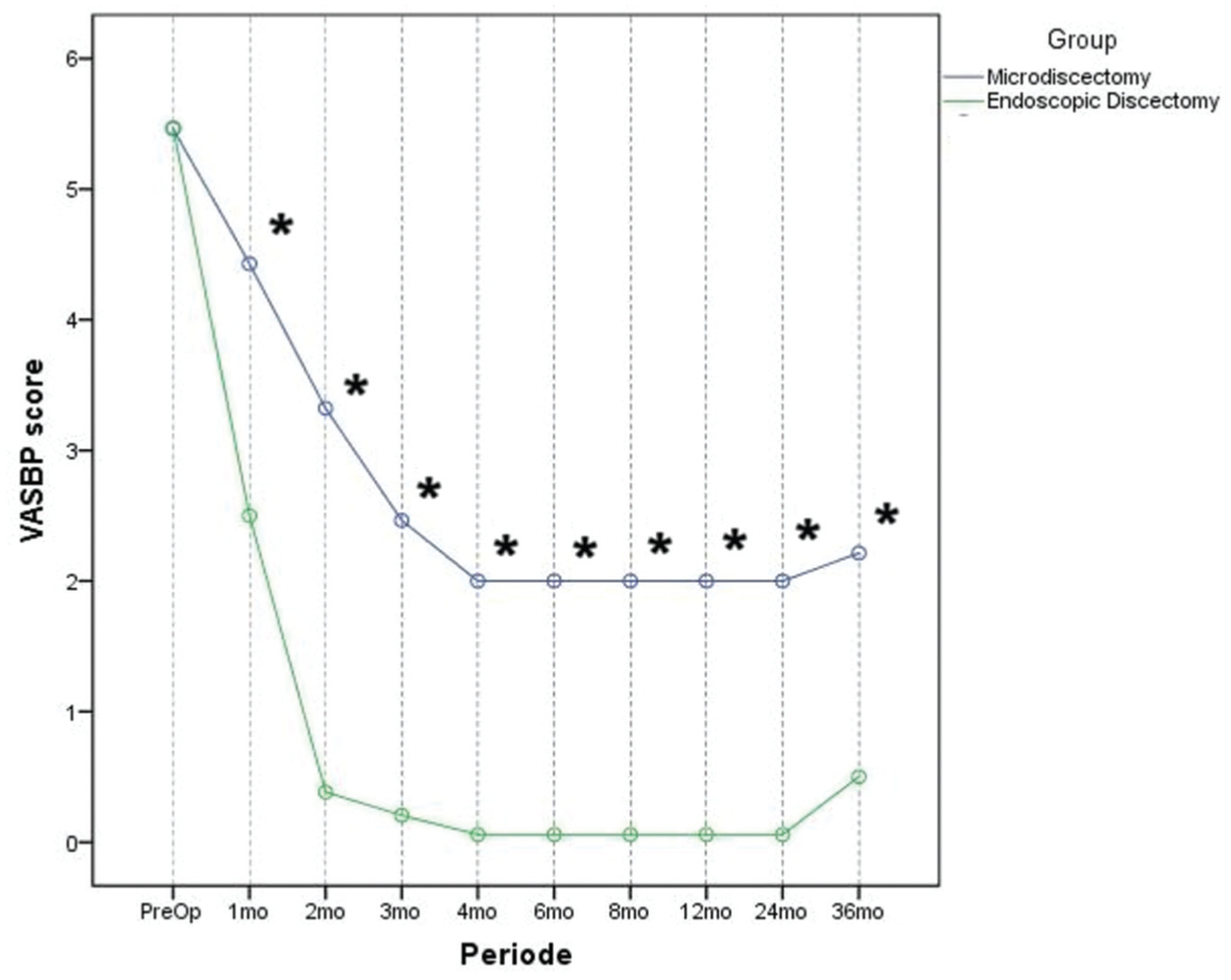
Comparative representation of VAS-BP values between the 2 groups at the follow-up. The asterisk indicates statistically significant differences. VAS-BP, visual analog scale for low back pain.

Schematic representation of VAS-LP values between the 2 groups at the follow-up. The asterisk indicates statistically significant differences. VAS-LP, visual analog scale for lower limb pain.
Evaluation of SF-36 Indices
Regarding SF-36 indices, preoperative values showed no statistically significant differences across the parameters studied. Regarding the BP index, a statistically significant difference (P < .001) in favor of Group B was observed from the first postoperative month until the final follow-up, at each interval (Figure 4, Appendix Table B).
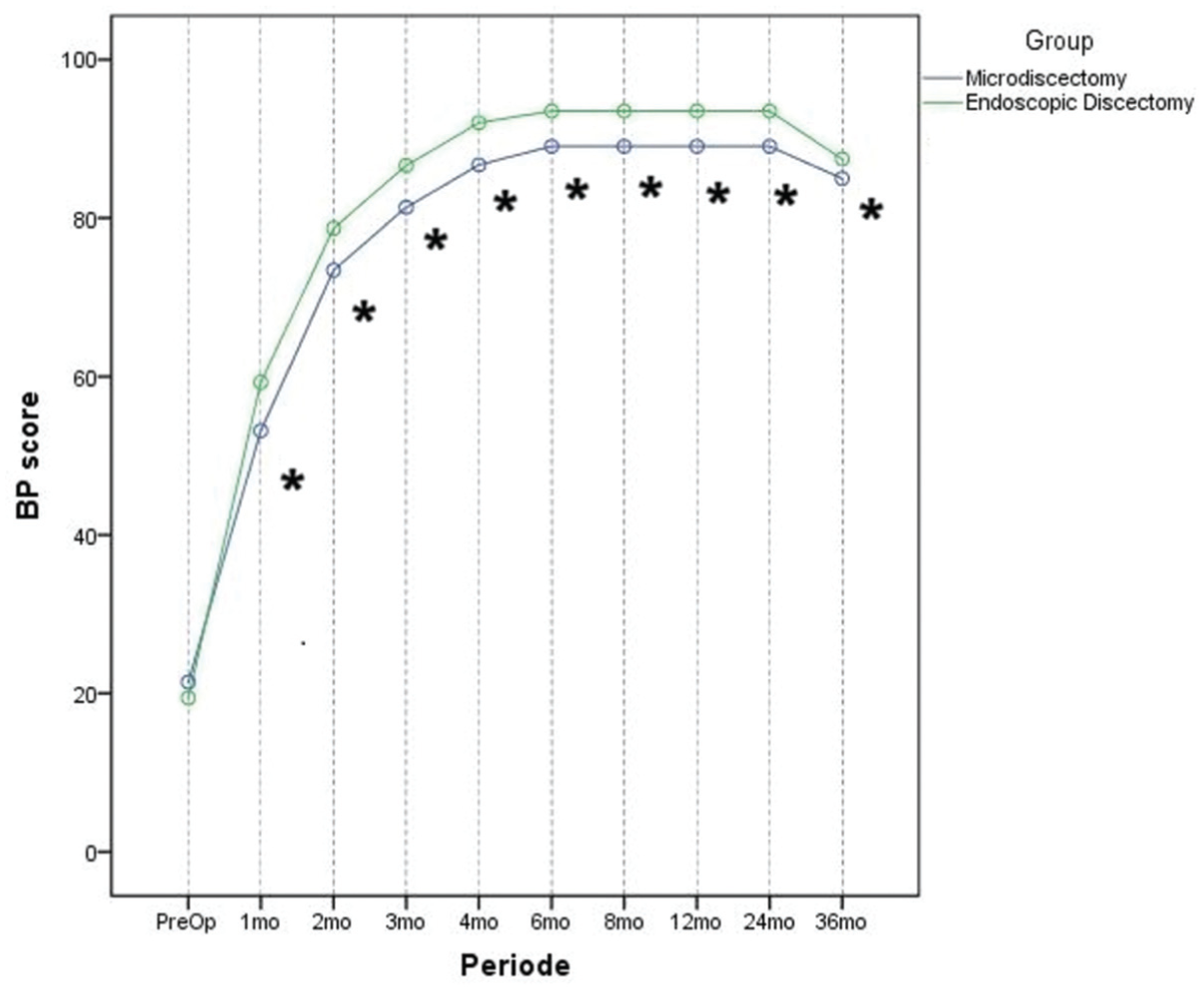
Comparative assessment of BP values during follow-up assessment. The asterisk indicates statistically significant differences. BP, bodily pain.
For RP, GH, and V, no statistically significant differences were observed in the comparative analysis between the 2 groups during the first postoperative month. However, from the second postoperative month onward, including the final follow-up (at each interval), a statistically significant difference in favor of Group B was recorded (Figure 5, Appendix Table B). No statistically significant difference was observed between the 2 groups in PF during the first and second postoperative months. However, statistically significant differences were observed from the third postoperative month onward through the final follow-up (Appendix Table B).

Representation of the V index between the 2 groups in various follow-up timepoints. The asterisk indicates statistically significant differences. V, Energy, fatigue, and vitality.
Particular attention was drawn to the changes in RE, MH, and SF during the follow-up period. Comparison of RE values between the 2 groups showed statistically significant differences from 4 to 24 months postoperatively, at each intervening time interval, with no statistical significance at the rest checkpoints. Data comparing MH between the 2 groups revealed a marginal, nonsignificant difference at the final 36-month follow-up. In contrast, statistically significant differences were observed at all other follow-up intervals (P < .001). A statistically significant difference was observed between the 2 groups in the SF parameter at 4 months postoperatively. In contrast, no statistically significant differences were recorded at any other time point (Figure 6, Appendix Table B).
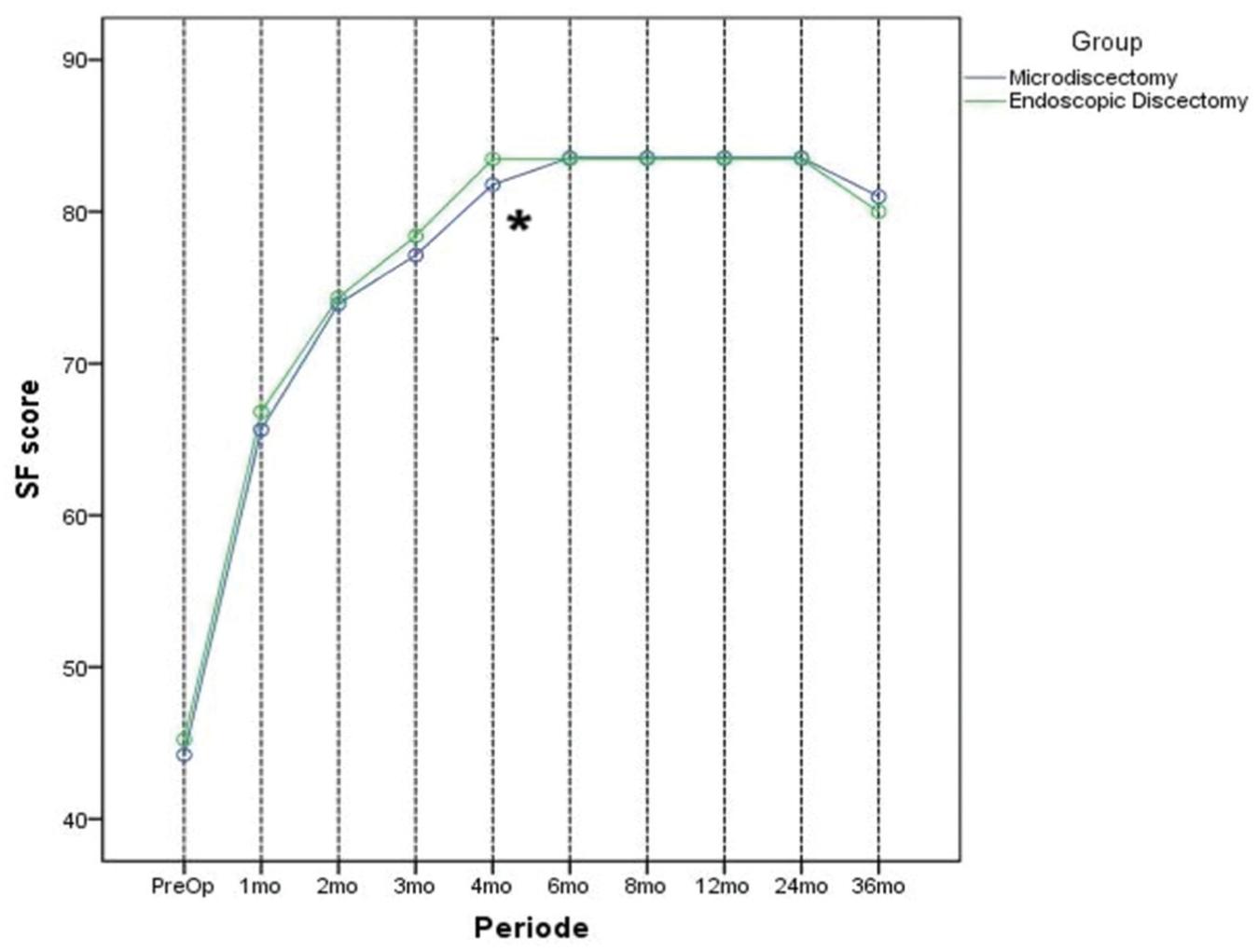
Comparative evaluation of the SF index between the 2 groups. The asterisk indicates statistically significant differences. SF, social function.
Length of Hospitalization, RTP, and Complications
The length of postoperative hospitalization for the patients was also evaluated. Specifically, the mean postoperative length of hospitalization was 17 ± 5.7 hours in Group A and 6.6 ± 0.9 hours in Group B, a statistically significant difference (P < .001). In terms of RTP time, the mean duration was 5.6 ± 0.6 months in Group A and 4 ± 0 months in Group B, with a statistically significant difference (P < .001). However, RTP rates were 100% for both groups. No major perioperative complications were observed. One patient (2.9%) in Group B featured temporary dysesthesia at the exiting nerve root distribution, which was totally resolved with conservative measures after the third postoperative month. Furthermore, 1 patient (3.6%) in Group A experienced a superficial wound infection, which was successfully managed with oral antibiotics and local wound care without the need for reoperation. Two patients in Group A (7.1%) and 3 in Group B (8.8%) experienced LDH recurrence, which was successfully managed via revision endoscopic TELD surgery in all cases.
Discussion
To the best of our knowledge, this is the first study to comparatively evaluate clinical outcomes of conventional microdiscectomy versus full-endoscopic TELD in elite athletes with LDH. Our results demonstrate that TELD represents a safe and effective alternative to microdiscectomy in selected patients, offering improved outcomes in reducing LBP and improving HRQoL, and enabling a faster return to the previous level of competitiveness with minor hospitalization and complication rates.
Surgical management of LDH in athletes has been investigated in only a few reports in the literature. In these studies, conventional microdiscectomy,1,3,4,9,22,23 microendoscopic discectomy, 29 and full-endoscopic discectomy6,14,19 were applied, with distinct functional outcomes.
Overley et al 22 published a systematic literature review and meta-analysis of available evidence to delineate the RTP rates for elite athletes after microdiscectomy for LDH. Nine studies were ultimately evaluated, totaling 558 patients. The pooled RTP rate was 83.5%. Interestingly, conservative management was not associated with a significantly different outcome. However, RTP times for the 2 groups were not reported or compared in this meta-analysis. Hence, authors concluded that prompt surgical treatment of symptomatic LDH may be beneficial for reducing RTP duration for elite athletes. 22 The same conclusion was also drawn from other meta-analyses, highlighting that the significant heterogeneity and low methodological quality limited the conclusions of these studies.23,24
In a more recent analysis, Kajy et al 9 evaluated the overall performance of elite athletes after surgical management of LDH with microdiscectomy. Enrolled patients demonstrated a high level of competitiveness and were all involved in 1 of the major American professional sports leagues. In total, 38 patients were retrospectively evaluated. Football players had the lowest RTP rate (64%), whereas ice hockey players had the highest (89%). Moreover, football players, on average, had a comparatively shorter postoperative career length of 34.8 months. Recovery time and return to preoperative performance level were the greatest for baseball players. Therefore, authors stated that microdiscectomy may be associated with a long-term decrease in an affected elite athlete's average performance, a fact that should be meticulously discussed preoperatively. 9 Nonetheless, this statement was not adopted from relative literature reports, which advocated for the beneficial role of microdiscectomy, with no particular focus, however, on postoperative career length or the mean time to return to the previous level of physical performance. 4
In a recently published study, Byvaltsev et al 1 retrospectively assessed 114 athletes with lumbar degenerative disease according to clinical and radiologic criteria and applied 4 distinct treatment methods: discectomy (microdiscectomy or endoscopic discectomy); platelet-rich plasma infusion into facet joints; artificial disc replacement; and lumbar interbody fusion. The discectomy group comprised 35 patients with a mean 5-year follow-up. The median RTP was observed after 12.6 weeks in this subgroup. In another report, Yoshimoto et al 29 found rapid RTP in the preoperative level after microendoscopic discectomy, advocating for the useful role of this technique given its minimal invasiveness.
More recently, given the evolution of full-endoscopic techniques for the surgical management of LDH, specific groups of scholars have sought to assess their utility for elite athletes. In their retrospective study, Nakamae et al 19 assessed 21 athletes with LDH who underwent TELD. Implemented outcome measures were VAS, Oswestry Disability Index (ODI), and RTP time. Results showed that VAS and ODI scores were statistically significantly improved postoperatively. Surgery was uneventful in all cases, whereas the overwhelming majority of enrolled individuals (95%) accomplished RTP at their previous performance level, on average, 9.2 weeks postoperatively. These findings suggest that TELD is a safe and effective alternative for the surgical management of LDH in athletes and is associated with rapid RTP. Findings of this study were also verified by the later published investigation of Kapetanakis et al, 14 in which the authors advocated for the safety and efficiency of TELD for the treatment of LDH in competitive elite athletes, after evaluation of HRQoL in 55 patients over a 2-year follow-up.
In another study on endoscopic management of LDH in elite athletes, Fujimoto et al 6 retrospectively examined 10 baseball players who underwent TELD, specifically focusing on the effect of timing of surgery on the postoperative course. Surgical operations were conducted preseason, during, and postseason, and patients were classified into respective groups. Analysis demonstrated that all patients returned to their previous level of professional activity at a mean of 4.6 months postoperatively. As expected, the comparative assessment demonstrated that the duration of game loss was significantly lower in the postseason group, with the majority of patients (66.6%) missing no games. 6
In our study, we conducted a comparative evaluation of TELD versus conventional microdiscectomy in 62 elite athletes with LDH. Analyzing our patient characteristics, basketball and volleyball were the most prevalent sports in the 2 groups—a finding that may be associated with the comparatively greater, repetitive axial compressive loads on the lumbar spine during these sports. 14 Furthermore, the L4-L5 segment was primarily affected in both groups, and no patients with L5-S1 pathology were present in this study. Technically speaking, this coincidence effectively enabled the implementation of TELD in these patients, since the L5-S1 level may inherently pose significant limitations to proper TELD conduction, including frequent minor foraminal dimensions, large transverse processes, and, potentially, high and steep iliac wings. 13
Hospitalization duration and RTP time were significantly shorter in the TELD group, supporting the minimal invasiveness of TELD. Analysis of these parameters demonstrates that our results are in line with those of the discussed reports,4,6 with isolated variations primarily attributable to the type of sport. 19 While we achieved 100% RTP rates with both treatments, previous studies have found that RTP rates are greater in athletes undergoing TELD for LDH rather than microdiscectomy.1,9,19,22
VAS-BP values were significantly lower in patients who underwent TELD compared with their counterparts, a difference consistently observed from the first postoperative month through the end of follow-up. Contrariwise, VAS-LP values were significantly lower in patients who underwent microdiscectomy in the first follow-up examination, a correlation that was, however, reversed after the fourth postoperative month. Regarding VAS-BP, it is generally accepted that patients who underwent microdiscectomy may experience postoperative chronic LBP. This symptom may be associated with paraspinal musculature traumatization with fibrosis, progressive degeneration of the operated disc, or segmental instability. 7 This may be responsible for the comparatively delayed RTP for patients in the microdiscectomy group. Furthermore, patients who underwent TELD exhibited long-term greater relief in lower limb pain, a fact that may be associated with adequate foraminal decompression via a minimally invasive route that reduces the potential of clinically significant epidural fibrosis and recurrence of nerve root impingement. 13 Our findings are consistent with the existing literature, particularly regarding TELD and its effectiveness in reducing low back and lower limb pain in elite athletes with LDH.14,19 However, despite the documented absence of comparative data between TELD and microdiscectomy in these patients, studies investigating the results of microdiscectomy do not routinely evaluate the VAS score, a fact that limits the comparability of performed interventions.1,9,22
Lastly, analysis of HRQoL with the SF-36 indicated that TELD patients scored significantly higher after the fourth postoperative month across all questionnaire domains except the SF. This demonstrates the beneficial role of TELD in improving the HRQoL of elite athletes in the short- and mid-term. Psychosocial parameters of SF-36 are closely related to RTP, as rapid and effective return to the previous level of sport activity may improve athletes' psychological and social status, thereby creating a vicious cycle. Again, data on the impact of TELD and microdiscectomy on postoperative HRQoL—with or without SF-36 evaluation—are extremely limited, reported only in 1 prospective investigation, in which the favorable role of TELD in HRQoL was also verified. 14
This is the first study to compare the role of TELD with microdiscectomy in elite athletes with LDH, a population defined with strict literature criteria. In our study, we found some benefits of TELD compared with microdiscectomy in elite athletes with LDH, with respect to postoperatively perceived pain and HRQoL. Furthermore, the follow-up time in our study is longer than in other reports evaluating endoscopic discectomy in athletes. In addition, beyond mere pain intensity assessment, we decided to shed light on these patients' quality of life after surgery to more precisely assess the multimodal effects of the interventions applied. These factors highlight the originality of our study within the existing literature but limit the comparability of our results with those of other studies.
Critically analyzing our results, TELD was associated with reduced hospitalization duration, more rapid RTP at the preoperative level, reduced postoperative pain, and improved overall HRQoL at the 3-year follow-up. We believe these findings should be attributed to the technique's pure minimally invasive character. Hence, TELD is strongly associated with minor skin incision, minimal intraoperative hemorrhage, epidural scarring, preservation of dorsal musculature and osseous and ligamentous structures, and overall spinal stability, as well as more rapid rehabilitation and return to daily routine.2,13 This procedure is also appropriate for revision cases, enabling more rapid rehabilitation. 28 Current data indicate that elite athletes may benefit from TELD, since early and maximal recovery is essential in this delicate population.
In general, results of this study show that TELD represents a safe and effective alternative surgical selection over conventional microdiscectomy for the surgical treatment of elite athletes with LDH. However, proper patient selection based on clinical and imaging findings—such as patient symptomatology, the anatomic location of LDH, and the surgeon's experience and familiarity with endoscopic spine surgery techniques—is a key factor for ensuring clinical success. Future research should focus on evaluating long-term TELD outcomes in larger prospective series with strict inclusion of elite athletes with LDH. Moreover, selecting patients from all sports categories and different LDH types under randomization is crucial. Data from such studies would guide clinical decision-making more efficiently by more reliably evaluating the role of TELD in these special patients.
Despite the documented consistency of our results with those reported in the relevant literature, our study is characterized by specific methodological limitations that warrant consideration. First, it is a retrospective study since a prospective evaluation was not possible for practical reasons. The design of the study may limit the validity of our results, as the limited availability of specific epidemiologic and perioperative data (eg, analgesic utilization) may act as potential confounders. Furthermore, patients with L5-S1 LDH were not included incidentally in this analysis, a fact that should also be considered when interpreting our results, given the frequent challenges in managing these cases with TELD. Second, the sample size was relatively small in both groups, consistent with previous studies. Third, an allocation process for interventions was not used in this study, as each patient was treated in a personalized manner based on clinical and imaging findings—a fact that may limit the validity of the outcomes in the setting of potential selection bias. In addition, the lack of masking of the performed intervention—a procedure not easy to perform in such an interventional study type—may be associated with underlying placebo effects that could also affect the outcome. Fourth, the implemented follow-up could also be extended to delineate mid- and long-term comparative outcomes of the 2 techniques. Fifth, the operating surgeon had extensive experience in performing TELD and microdiscectomy before the initiation of this study—a fact that may also hinder the reproducibility of results for other surgeons with less experience in endoscopic spine surgery techniques.
Conclusion
TELD represents a safe and effective alternative for the surgical management of LDH in elite athletes and may offer advantages over conventional microdiscectomy, primarily related to its minimal invasiveness. However, meticulous patient selection and the determination of patients’ expectations are critical to identifying patients suitable for the TELD procedure, given the relative paucity of such data in the literature to date.
Footnotes
Appendix
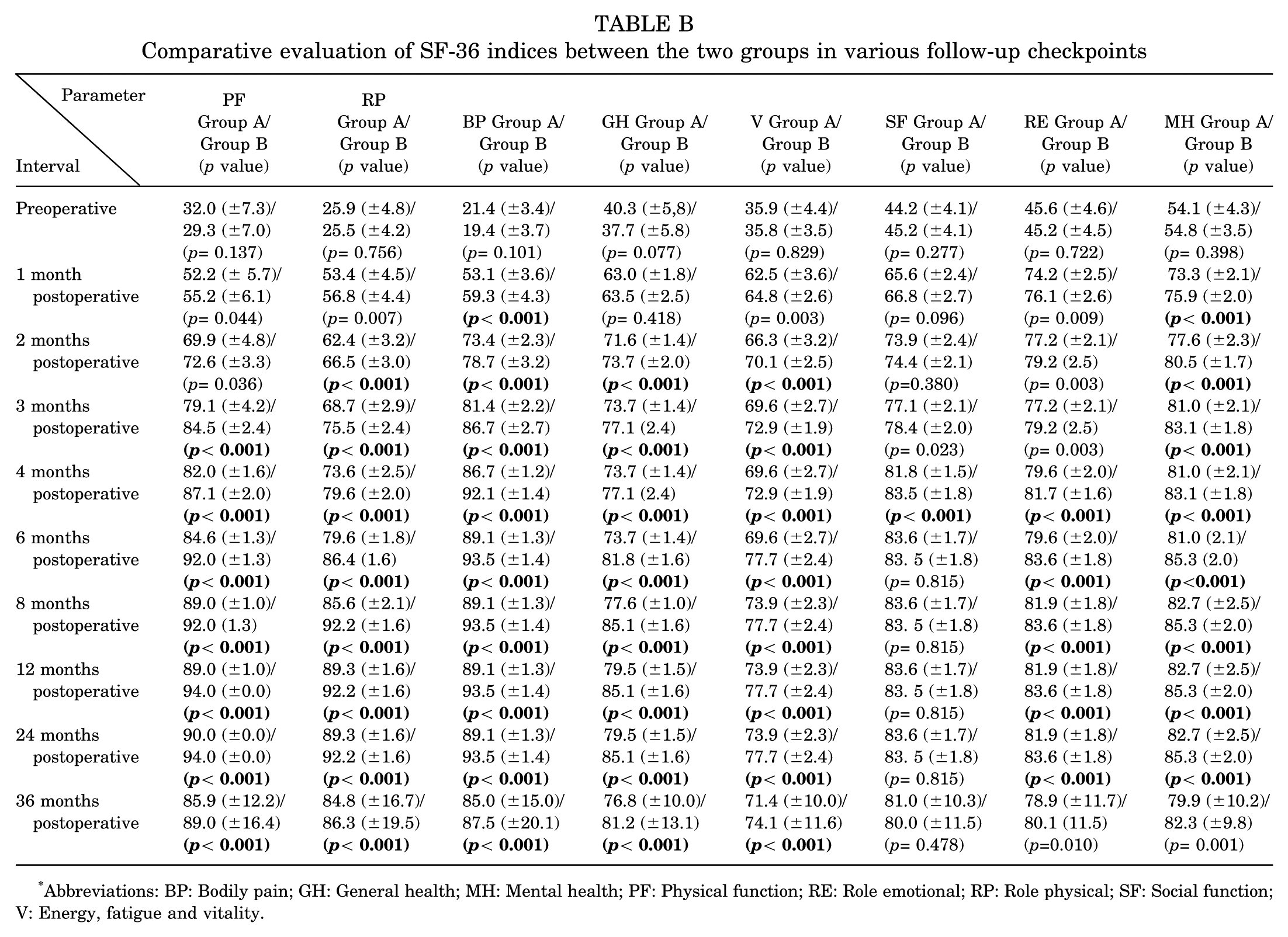
Comparative evaluation of SF-36 indices between the two groups in various follow-up checkpoints
| Parameter |
PF |
RP |
BP Group A/ Group B |
GH Group A/ Group B |
V Group A/ Group B |
SF Group A/ Group B |
RE Group A/ Group B |
MH Group A/ Group B |
|---|---|---|---|---|---|---|---|---|
| Preoperative | 32.0 (±7.3)/ 29.3 (±7.0) (p= 0.137) |
25.9 (±4.8)/ 25.5 (±4.2) (p= 0.756) |
21.4 (±3.4)/ 19.4 (±3.7) (p= 0.101) |
40.3 (±5,8)/ 37.7 (±5.8) (p= 0.077) |
35.9 (±4.4)/ 35.8 (±3.5) (p= 0.829) |
44.2 (±4.1)/ 45.2 (±4.1) (p= 0.277) |
45.6 (±4.6)/ 45.2 (±4.5) (p= 0.722) |
54.1 (±4.3)/ 54.8 (±3.5) (p= 0.398) |
| 1 month postoperative | 52.2 (± 5.7)/ 55.2 (±6.1) (p= 0.044) |
53.4 (±4.5)/ 56.8 (±4.4) (p= 0.007) |
53.1 (±3.6)/ 59.3 (±4.3) |
63.0 (±1.8)/ 63.5 (±2.5) (p= 0.418) |
62.5 (±3.6)/ 64.8 (±2.6) (p= 0.003) |
65.6 (±2.4)/ 66.8 (±2.7) (p= 0.096) |
74.2 (±2.5)/ 76.1 (±2.6) (p= 0.009) |
73.3 (±2.1)/ 75.9 (±2.0) |
| 2 months postoperative | 69.9 (±4.8)/ 72.6 (±3.3) (p= 0.036) |
62.4 (±3.2)/ 66.5 (±3.0) |
73.4 (±2.3)/ 78.7 (±3.2) |
71.6 (±1.4)/ 73.7 (±2.0) |
66.3 (±3.2)/ 70.1 (±2.5) |
73.9 (±2.4)/ 74.4 (±2.1) (p=0.380) |
77.2 (±2.1)/ 79.2 (2.5) (p= 0.003) |
77.6 (±2.3)/ 80.5 (±1.7) |
| 3 months postoperative | 79.1 (±4.2)/ 84.5 (±2.4) |
68.7 (±2.9)/ 75.5 (±2.4) |
81.4 (±2.2)/ 86.7 (±2.7) |
73.7 (±1.4)/ 77.1 (2.4) |
69.6 (±2.7)/ 72.9 (±1.9) |
77.1 (±2.1)/ 78.4 (±2.0) (p= 0.023) |
77.2 (±2.1)/ 79.2 (2.5) (p= 0.003) |
81.0 (±2.1)/ 83.1 (±1.8) |
| 4 months postoperative | 82.0 (±1.6)/ 87.1 (±2.0) |
73.6 (±2.5)/ 79.6 (±2.0) |
86.7 (±1.2)/ 92.1 (±1.4) |
73.7 (±1.4)/ 77.1 (2.4) |
69.6 (±2.7)/ 72.9 (±1.9) |
81.8 (±1.5)/ 83.5 (±1.8) |
79.6 (±2.0)/ 81.7 (±1.6) |
81.0 (±2.1)/ 83.1 (±1.8) |
| 6 months postoperative | 84.6 (±1.3)/ 92.0 (±1.3) |
79.6 (±1.8)/ 86.4 (1.6) |
89.1 (±1.3)/ 93.5 (±1.4) |
73.7 (±1.4)/ 81.8 (±1.6) |
69.6 (±2.7)/ 77.7 (±2.4) |
83.6 (±1.7)/ 83. 5 (±1.8) (p= 0.815) |
79.6 (±2.0)/ 83.6 (±1.8) |
81.0 (2.1)/ 85.3 (2.0) |
| 8 months postoperative | 89.0 (±1.0)/ 92.0 (1.3) |
85.6 (±2.1)/ 92.2 (±1.6) |
89.1 (±1.3)/ 93.5 (±1.4) |
77.6 (±1.0)/ 85.1 (±1.6) |
73.9 (±2.3)/ 77.7 (±2.4) |
83.6 (±1.7)/ 83. 5 (±1.8) (p= 0.815) |
81.9 (±1.8)/ 83.6 (±1.8) |
82.7 (±2.5)/ 85.3 (±2.0) |
| 12 months postoperative | 89.0 (±1.0)/ 94.0 (±0.0) |
89.3 (±1.6)/ 92.2 (±1.6) |
89.1 (±1.3)/ 93.5 (±1.4) |
79.5 (±1.5)/ 85.1 (±1.6) |
73.9 (±2.3)/ 77.7 (±2.4) |
83.6 (±1.7)/ 83. 5 (±1.8) (p= 0.815) |
81.9 (±1.8)/ 83.6 (±1.8) |
82.7 (±2.5)/ 85.3 (±2.0) |
| 24 months postoperative | 90.0 (±0.0)/ 94.0 (±0.0) |
89.3 (±1.6)/ 92.2 (±1.6) |
89.1 (±1.3)/ 93.5 (±1.4) |
79.5 (±1.5)/ 85.1 (±1.6) |
73.9 (±2.3)/ 77.7 (±2.4) |
83.6 (±1.7)/ 83. 5 (±1.8) (p= 0.815) |
81.9 (±1.8)/ 83.6 (±1.8) |
82.7 (±2.5)/ 85.3 (±2.0) |
| 36 months postoperative | 85.9 (±12.2)/ 89.0 (±16.4) |
84.8 (±16.7)/ 86.3 (±19.5) |
85.0 (±15.0)/ 87.5 (±20.1) |
76.8 (±10.0)/ 81.2 (±13.1) |
71.4 (±10.0)/ 74.1 (±11.6) |
81.0 (±10.3)/ 80.0 (±11.5) (p= 0.478) |
78.9 (±11.7)/ 80.1 (11.5) (p=0.010) |
79.9 (±10.2)/ 82.3 (±9.8) (p= 0.001) |
Abbreviations: BP: Bodily pain; GH: General health; MH: Mental health; PF: Physical function; RE: Role emotional; RP: Role physical; SF: Social function; V: Energy, fatigue and vitality.
Final revision submitted February 1, 2026; accepted February 10, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from our hospital's institutional review board (Interbalkan European Medical Center, Thessaloniki, Greece) (Approval No.: 1712/14.04.2022). Furthermore, written informed consent was obtained from each patient for participation.
Data Availability
Retrieved data associated with this work are not publicly published but are available on reasonable request to the corresponding author.