
Abstract
Background:
Shoulder instability is a significant cause of disability in pitchers. The advent of advanced pitch-tracking technology now provides an opportunity to investigate the mechanical factors associated with these injuries on a large scale in Major League Baseball (MLB).
Purpose/Hypothesis:
The purpose of this study was to identify preinjury advanced analytic and pitch-tracking metrics associated with surgically treated shoulder instability in MLB. It was hypothesized that pitchers requiring surgery would demonstrate distinct preinjury profiles in advanced performance analytics and Statcast data compared with matched controls.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
MLB pitchers who underwent primary capsulolabral repair from 2017 to 2024 (n = 35) were identified using public web sources used in previous studies. Each case was matched 2:1 with uninjured control pitchers (n = 70) based on age, role, handedness, season, and total pitch count. Advanced analytic and various pitch-tracking metrics were compiled from MLB-sponsored databases commonly used in player evaluation and prior research. The statistical analysis included unpaired t tests to compare groups and binary logistic regression to identify risk factors.
Results:
MLB pitchers who underwent capsulolabral surgery demonstrated superior preinjury performance metrics (including the FanGraphs version of wins above replacement [fWAR], fielding independent pitching [xFIP], expected earned run average [xERA], Stuff+, and walks plus hits per inning pitched) and pitch characteristics (including fastball velocity and spin rate), along with a more medial release point compared with controls. Binary logistic regression identified both Stuff+ and a medial release point as independent factors associated with surgery. Notably, the composite Stuff+ metric demonstrated a stronger association than velocity or spin rate alone in the final model (P < 05 for all significant factors).
Conclusion:
Several modern advanced analytic and pitch-tracking metrics were looked at as potential risk factors for shoulder instability in MLB pitchers for the first time. Pitchers who underwent capsulolabral surgery were more likely to throw harder with higher spin rates and a more medialized release point than matched controls. Overall, MLB pitchers who were more effective and had superior Stuff+ were at the highest risk for shoulder instability requiring surgical intervention. These findings point to a potential trade-off in modern pitching; the pursuit of elite performance is linked to a greater likelihood of injury.
The modern game of baseball is defined by data. From amateur showcases to major league front offices, advanced tracking technologies have transformed how pitchers are evaluated, developed, and managed. 29 The widespread adoption of PITCHf/x in 2007, followed by TrackMan radar in 2017, and the current Hawk-Eye optical system in 2020, has produced a continuous, high-resolution record of every pitch thrown in Major League Baseball (MLB) competition. 29 These systems now quantify kinematics including velocity, spin, movement, arm angle, release extension, and release position with precision, generating an unprecedented view of the pitching motion. 40 As a result, analytics once confined to biomechanic laboratories are now available on a league-wide scale, fueling a generation of pitchers who train and compete according to measurable performance metrics.
Amid this analytical revolution, injury rates have continued to rise despite pitch counts never being lower. 33 The resources available to help pitchers throw harder, spin the ball faster, and generate more movement are greater than at any previous point in the sport's history.8,41 The economic and competitive impact of upper-extremity injuries has therefore intensified,28,39 prompting years of investigation into risk factors and workload management strategies.1,6,19,31,32 Yet despite these interventions, both shoulder and elbow pathologies remain leading causes of lost playing time. 14 This disconnect between technological advancement and injury prevention underscores a critical gap: the same metrics and technology used to optimize performance may also hold the key to identifying early signs of breakdown.
Most large-scale pitch-tracking studies to date have focused on the elbow, particularly ulnar collateral ligament (UCL) injuries.6,9,23,24,26,38,48 Using public Statcast data, investigators have linked increased velocity, spin rate, command, overall pitching ability, and pitch-type specific differences to elevated UCL-surgery risk.6,9,23,24,26,38,48 These works have established an important analytic framework connecting in-game mechanics to medical outcomes. However, shoulder pathology, especially injuries of the labrum and capsule, has received far less attention within this realm, despite accounting for roughly 17% of all pitcher injuries. 7
The glenoid labrum deepens the socket and stabilizes the humeral head, but repetitive overhead throwing subjects it to extreme rotational and shear forces, particularly during late cocking and deceleration phases of the throwing motion.4,36 Over time, these stresses can lead to attenuation of the capsule and tearing of the labrum.4,30,36 Although nonoperative management is initially preferred, professional pitchers often require arthroscopic repair, and surgical outcomes remain guarded; only 40% to 60% regain their prior performance,15,42 and rehabilitation from surgery commonly exceeds a year. 16 These clinical realities highlight the need for objective, data-driven indicators capable of detecting early mechanical deterioration or potential risk factors before irreversible injury that requires surgical intervention occurs.
The present study leverages MLB's Statcast infrastructure and other composite analytic metrics (Stuff+, Location+, Pitching+, FanGraphs wins above replacement [fWAR], expected fielding independent pitching [xFIP]) to explore pitch-tracking signatures preceding shoulder capsulolabral surgery. By extending this advanced-analytics methodology beyond the elbow to the shoulder, this work aims to define any potential advanced analytic or pitch-tracking risk factors for shoulder instability treated operatively and thus inform future efforts toward evidence-based injury prevention in professional baseball.
Methods
Study Design and Ethical Considerations
This investigation was designed as a case-control study to identify potential advanced analytical and performance predictors of shoulder labral or capsular injury among MLB pitchers. The study compared a cohort of injured athletes with a matched cohort of uninjured controls. As it did not qualify as human participants research per 45 Code of Federal Regulations Part 46.102, this investigation was classified as exempt from institutional review board oversight at our institution.
Case Identification and Cohort Assembly
The case group consisted of MLB pitchers who underwent primary shoulder capsulolabral repair between March 1, 2017, and December 1, 2024. Potential cases were initially identified by reviewing injured list designations for shoulder-related conditions during this time frame, cross-referencing FanGraphs and Spotrac injury databases.11,44 Verification of both the diagnosis and the surgical management was performed through public news reports and official team announcements. To minimize bias, 3 independent reviewers (M.R.D., N.F., and M.A.M.) carried out this classification process, with disagreements resolved through consensus discussion, yielding an initial pool of 39 pitchers. To be included in the final case cohort for the primary analysis, pitchers were required to have ≥2 consecutive seasons of qualifying preoperative performance data at the MLB level, defined as throwing a minimum of 100 tracked pitches per season. The application of this criterion resulted in a final case cohort of 35 pitchers. A separate consideration was made for the analysis of 3 advanced metrics (Stuff+, Location+, and Pitching+) and arm angle, which have only been publicly recorded since 2020. To maximize statistical power for these variables, the 2-season data requirement was waived, resulting in a subanalysis cohort of 21 cases and 42 controls for the season preceding surgery (T1) and 22 cases with 47 controls for the index surgical season.
Control Identification and Cohort Assembly
A matched-control cohort was assembled at a 2:1 ratio (n = 70), employing an established methodology from prior case-control studies of UCL injuries in MLB pitchers.23,24 To account for recognized covariates in pitching-related injury risk, each control was matched to a case by the season of surgery, age at the index year, handedness, pitcher role (starter vs reliever), and total pitch count. To be eligible, controls were required to have no history of shoulder surgery and to have thrown ≥100 tracked pitches in each of the 2 analyzed seasons, thereby ensuring comparable data availability with the case cohort.
Data Sources and Collection
Data were aggregated from several publicly available and well-validated baseball databases, primarily Baseball Savant, Brooks Baseball, and FanGraphs. These platforms compile and report statistics, advanced performance metrics, and Statcast tracking data. Statcast, which is installed in all MLB stadiums, uses high-resolution optical cameras and radar-based tracking technologies to capture every pitch. 29 Parameters measured by Statcast include pitch velocity, spin rate, release point coordinates, and horizontal and vertical movement. 40 An analytical data set was constructed in a structured Excel workbook with separate sheets for cases and controls at each time point: the index season (year of surgery) and the 3 preceding seasons (T1, T2, T3). Demographic and descriptive data included age, height, weight, body mass index (BMI), handedness, pitcher role (starter or reliever), and draft position. Average workload and performance data consisted of annual pitch counts and advanced sabermetric measures of overall value and effectiveness, including fWAR), xFIP, and skill-interactive ERA, as reported by FanGraphs.
Mean pitch-tracking data included fastball velocity, slider velocity, and curveball velocity. Pitch usage was measured as the percentage of total pitches that were fastballs, sliders, curveballs, or changeups. Spin rate was recorded as the rotational velocity of the baseball upon release, expressed in revolutions per minute (rpm). Release point variables included extension, defined as the distance in feet from the pitching rubber to the point of release toward home plate, as well as horizontal and vertical release positions, which represent the spatial coordinates of the ball at release relative to the center of the rubber. Arm angle was defined as the horizontal angle, measured in degrees, between a horizontal line parallel to the ground and a line parallel to the pitcher's throwing shoulder and the ball at release (Figure 1).

Illustration of pitch release kinematic measurements. Pos X represents the horizontal release position, a measure of the horizontal distance of the ball at release from the center of the rubber. Pos Z represents the vertical release position, which is the height of the ball compared with the rubber. Arm angle is the horizontal angle between a horizontal line parallel to the ground and a line parallel to the pitcher's throwing shoulder and the ball at release.
Ball movement was also measured, with horizontal and vertical movement representing deviations in inches from a theoretical nonspinning trajectory. For analytical consistency, all horizontal movement metrics, along with horizontal release position, were normalized for pitcher handedness by using absolute values, while vertical movement, which is independent of handedness, retained positive and negative values. Approach angle was measured as both vertical approach angle and horizontal approach angle above average. These variables describe the trajectory of the pitch as it enters the strike zone and are normalized for release point and handedness, providing a standardized measure of pitch path. Finally, advanced composite metrics were included in the data set, specifically Stuff+, Location+, and Pitching+, which are proprietary statistics reported by FanGraphs beginning in 2020 and widely valued throughout the league (Table 1). These scores provide composite evaluations of pitch quality (Stuff+), command (Location+), and overall pitching effectiveness (Pitching+), with a value of 100 representing roughly the league average.
Definitions of Commonly Used Advanced Analytics in MLB a

MLB, Major League Baseball; UCL, ulnar collateral ligament. Stuff+, Pitching+, and Location+ are all scaled similarly to IQ: a score of 100 is graded out as approximately league average. Table reproduced with permission from Mastroianni MA, Kunes JA, El-Najjar DB, et al. Advanced analytic and pitch-tracking metrics associated with UCL surgery in Major League Baseball pitchers: a case-control study. Orthop J Sports Med. 2025;13(2):23259671241302432.
Statistical Analysis
Comparisons between cases and controls were performed at 2 primary time points: the season immediately prior to surgery (T1) and the index season. Continuous variables were reported as mean ± SD and compared using 2-sample Welch t tests. Categorical variables were assessed with Fisher exact test. These comparisons were conducted as unpaired analyses, meaning the matching procedure was not explicitly modeled in the hypothesis tests. While a 2:1 matched design was used to assemble the cohort and ensure baseline comparability, an unpaired analysis was retained for the primary comparisons to maximize statistical power and avoid the data loss associated with incomplete case-control sets in a conditional model.
To evaluate longitudinal preinjury trends, pitching metrics were analyzed across the 3 preoperative seasons (T3−T1). For each pitcher with ≥2 available preoperative data points, a simple least squares regression was performed to calculate an individual slope representing the average rate of change per season for each metric. These slopes were then compared between cases and controls using Welch t tests.
To identify independent predictors of injury, a multivariable logistic regression model was constructed using T1 data. Author judgment was used to exclude certain variables related to each other (eg, Pitching+ is influenced heavily by Stuff+ and Location+), to minimize collinearity while capturing clinically relevant metrics. Because fastball velocity, spin rate, and Stuff+ are closely interrelated measures of pitch quality, we first ran a preliminary model including only these variables to determine which demonstrated the strongest independent association with injury risk. The variable showing the most robust relationship was then carried forward into the final multivariable model with additional mechanical and usage metrics. Adjusted odds ratios (aORs) and their 95% CIs were calculated and reported for interpretable increments of each predictor. The logistic regression models, which included the post-2020 metrics Stuff+ and Location+, were necessarily run on this smaller subanalysis cohort. A complete case analysis was performed, resulting in final models derived from 22 cases and 47 controls.
Statistical Analysis and Software
All statistical analyses were performed using R (Version 4.3.1), with the dplyr, tidyr, broom, and flextable packages. A 2-sided P value <.05 was considered statistically significant for 2-sample t tests, whereas a threshold of P < .10 was used in the logistic regression model to identify potential predictors of injury.
Results
Demographics and Baseline Characteristics
A total of 35 cases and 70 matched controls were included in the primary analysis. There were no statistically significant differences between the case and control cohorts with respect to age, height, weight, BMI, draft position, or career MLB seasons. The groups were perfectly matched for handedness and pitcher role, as per the study design. Baseline workload metrics, including innings pitched and total pitch count in the season prior to the index year (T1), were also similar between groups (all P > .10), as detailed in Table 2.
Demographics and Baseline Characteristics of MLB Pitchers Undergoing Capsulolabral Surgery Compared with Matched Controls a

Data are presented as mean ± SD or percentage. BMI, body mass index; MLB, Major League Baseball; T1, season prior to injury. P values were calculated using 2-sample Welch t tests for continuous variables and Fisher exact test for categorical variables. All between-group comparisons (case vs control) were not significant (P > .05).
Performance Metrics and Advanced Analytics
Analysis of the 3 plus metrics (Stuff+, Location+, Pitching+) included 21 cases and 42 controls for T1 and 22 cases and 47 controls for the index surgical season, secondary to our loosened inclusion criteria in a limited sample size secondary to these metrics only being available since 2020. Analysis of advanced performance metrics revealed significant differences between groups. In the season before surgery (T1), cases had a lower earned run average (ERA) than controls (3.90 ± 1.37 vs 4.98 ± 2.32; P < .01) and maintained an advantage in the index season (3.96 ± 1.87 vs 4.78 ± 1.78; P = .03). FIP was also superior among cases at T1 (3.92 ± 0.91 vs 4.50 ± 1.34; P = .01), though this difference did not persist in the index season. Similarly, cases demonstrated higher fWAR values at T1 (0.95 ± 1.11 vs 0.50 ± 0.95; P = .045), while expected ERA was significantly lower (3.91 ± 0.92 vs 4.57 ± 1.28; < .01). Of the advanced Statcast-based metrics, Stuff+ was markedly higher in cases at both T1 (105.85 ± 10.00 vs 97.33 ± 10.59; P < .01) and the index season (102.95 ± 9.57 vs 96.77 ± 10.72; P = .02). In contrast, Location+ and Pitching+ did not differ significantly at either time point (Table 3).
Advanced Performance and Analytical Metrics in Capsulolabral Surgery Cases Versus Matched Controls a
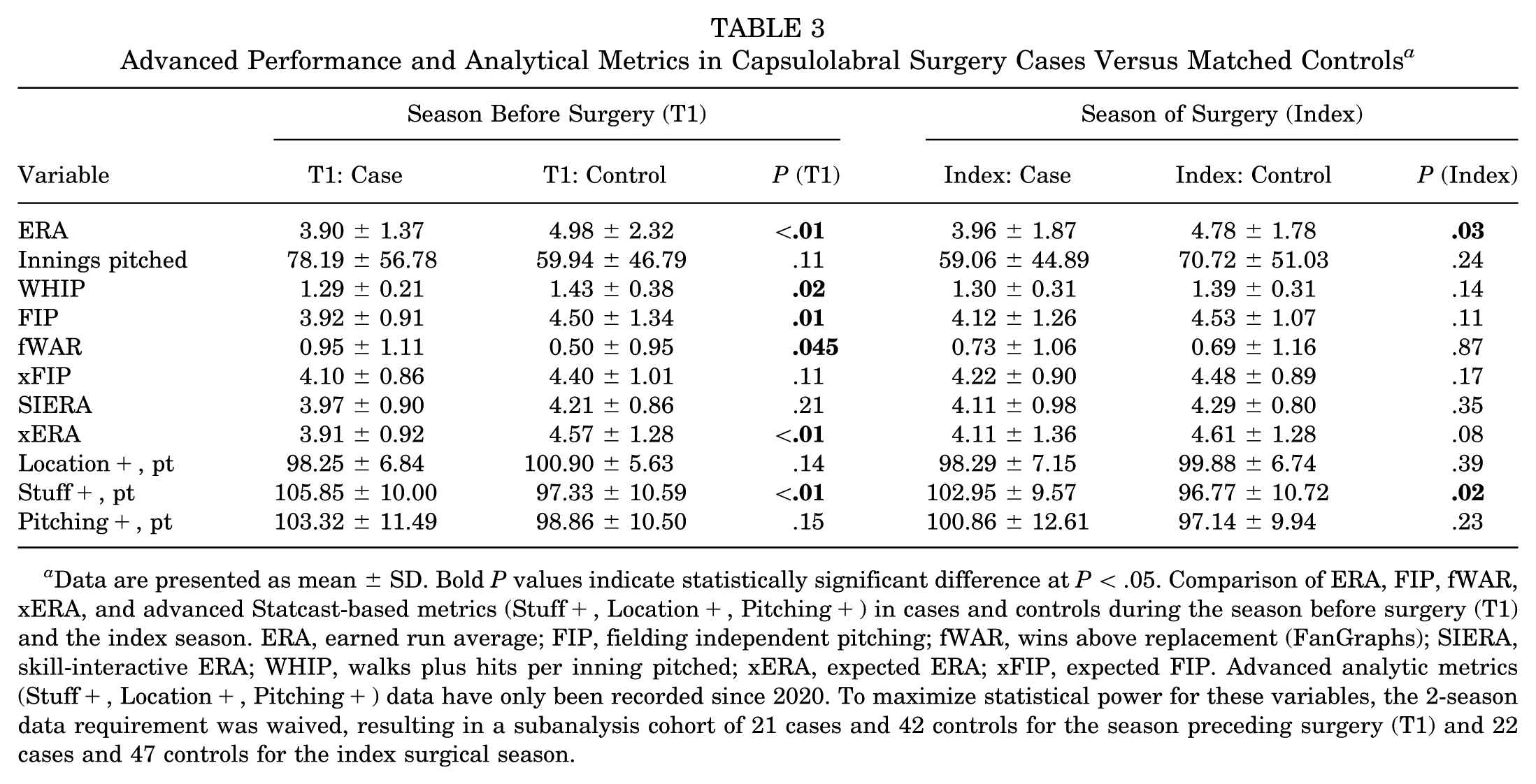
Data are presented as mean ± SD. Bold P values indicate statistically significant difference at P < .05. Comparison of ERA, FIP, fWAR, xERA, and advanced Statcast-based metrics (Stuff+, Location+, Pitching+) in cases and controls during the season before surgery (T1) and the index season. ERA, earned run average; FIP, fielding independent pitching; fWAR, wins above replacement (FanGraphs); SIERA, skill-interactive ERA; WHIP, walks plus hits per inning pitched; xERA, expected ERA; xFIP, expected FIP. Advanced analytic metrics (Stuff+, Location+, Pitching+) data have only been recorded since 2020. To maximize statistical power for these variables, the 2-season data requirement was waived, resulting in a subanalysis cohort of 21 cases and 42 controls for the season preceding surgery (T1) and 22 cases and 47 controls for the index surgical season.
Pitch-Tracking Characteristics
Pitch-tracking variables demonstrated key differences between cohorts. At T1, cases had significantly higher average fastball velocity compared with controls (94.33 ± 2.23 mph vs 93.35 ± 2.08 mph; P = .03), though this difference diminished by the index season. Spin rate was also greater in cases at T1 (2293.43 ± 190.34 rpm vs 2200.60 ± 198.40 rpm; P = .02), with a nonsignificant trend persisting into the index season (P = .06). Horizontal release position (release pos X) was more medial (closer to the body) in cases compared with controls at both T1 (1.69 ± 0.59 feet vs 1.97 ± 0.58 feet; P = .02) and the index season (1.63 ± 0.70 feet vs 1.91 ± 0.53 feet; P = .04). Other variables, including slider and curveball velocity, usage percentages, release extension, arm angle, and ball movement parameters, did not differ significantly between groups (Table 4).
Statcast Pitch-Tracking Metrics in Capsulolabral Surgery Cases Versus Controls a
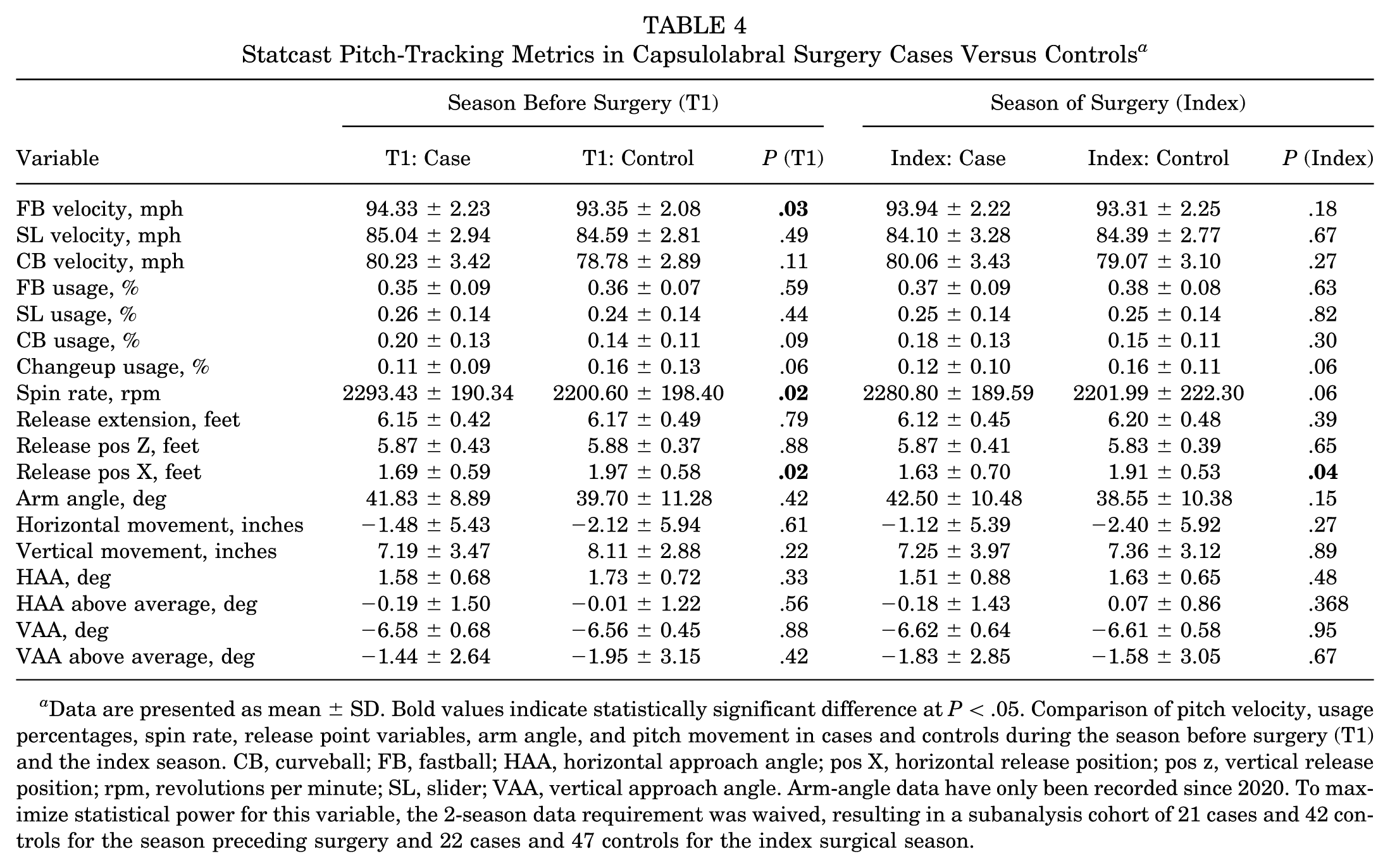
Data are presented as mean ± SD. Bold values indicate statistically significant difference at P < .05. Comparison of pitch velocity, usage percentages, spin rate, release point variables, arm angle, and pitch movement in cases and controls during the season before surgery (T1) and the index season. CB, curveball; FB, fastball; HAA, horizontal approach angle; pos X, horizontal release position; pos z, vertical release position; rpm, revolutions per minute; SL, slider; VAA, vertical approach angle. Arm-angle data have only been recorded since 2020. To maximize statistical power for this variable, the 2-season data requirement was waived, resulting in a subanalysis cohort of 21 cases and 42 controls for the season preceding surgery and 22 cases and 47 controls for the index surgical season.
Longitudinal Preinjury Trends
Longitudinal slope analysis from T3 to T1 did not reveal significant differences in per-season changes for most variables. Cases trended toward greater increases in curveball usage compared with controls (Δ per season 0.03% ± 0.05% vs −0.00% ± 0.05%; P = .057) and toward less favorable vertical approach angle changes (−0.02°± 0.18° vs −0.14°± 0.26°; P = .07), although these did not meet the threshold for statistical significance. Similarly, controls demonstrated a nonsignificant trend toward greater improvement in Location+ (Δ 5.74 ± 7.58 points vs 0.89 ± 7.06 points; P = .07). No other workload, velocity, spin, or performance metrics differed between groups over this preinjury interval (Table 5).
Longitudinal Slopes of Pitch-Tracking and Performance Metrics (T3–T1) a

Data are presented as mean ± SD. Longitudinal slopes of pitch-tracking and performance metrics from T3 to T1 were calculated for capsulolabral surgery cases and matched controls. ERA, earned run average; FB, fastball; FIP, fielding independent pitching; fWAR, wins above replacement (FanGraphs); HAA, horizontal approach angle; pos X, horizontal release position; pos z, vertical release position; pt, point; rpm, revolutions per minute; SIERA, skill-interactive ERA; Stuff+, Pitching+, and Location+, PitchingBot advanced run prevention metrics; VAA, vertical approach angle; WHIP, walks plus hits per inning pitched; xERA, expected ERA; xFIP, expected FIP.
Preliminary Logistic Regression
The preliminary regression compared fastball velocity, spin rate, and Stuff+ to evaluate which was the stronger predictor of capsulolabral surgery. Stuff+ showed the greatest effect size and approached statistical significance (P = .06), suggesting it better captures underlying risk than velocity or spin alone (Table 6). This variable was therefore included in the subsequent multivariable model alongside mechanical and usage metrics.
Multivariable Logistic Regression Model for Predictors of Capsulolabral Surgery a
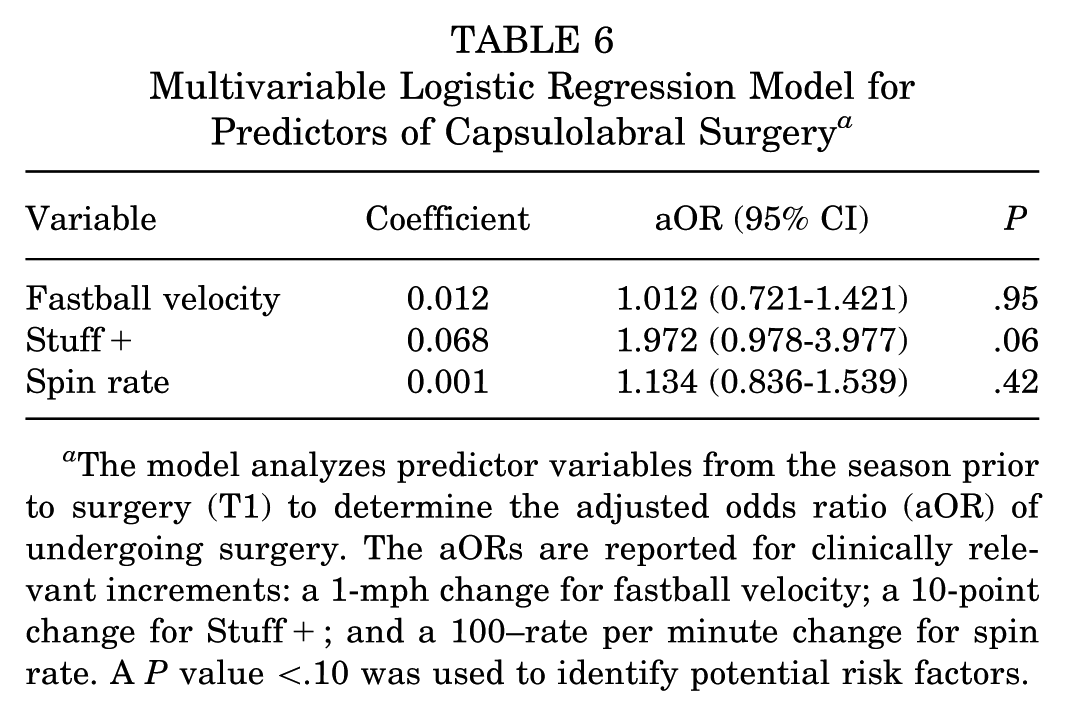
The model analyzes predictor variables from the season prior to surgery (T1) to determine the adjusted odds ratio (aOR) of undergoing surgery. The aORs are reported for clinically relevant increments: a 1-mph change for fastball velocity; a 10-point change for Stuff+; and a 100–rate per minute change for spin rate. A P value <.10 was used to identify potential risk factors.
Multivariable Logistic Regression
In the full multivariable logistic regression model using T1 data, 2 variables demonstrated notable associations with capsulolabral surgery risk. A more medial horizontal release position was significantly associated with increased odds of surgery (aOR, 0.86 per 0.1 feet; 95% CI, [0.74-0.99]; P = .03). Higher Stuff+ was also a significant independent predictor, with greater values associated with increased odds of surgery (aOR, 2.07 per 10-point increase; 95% CI, [1.10-3.88]; P = .02). Full results of the multivariable model are presented in Table 7.
Multivariable Logistic Regression Model for Predictors of Capsulolabral Surgery a
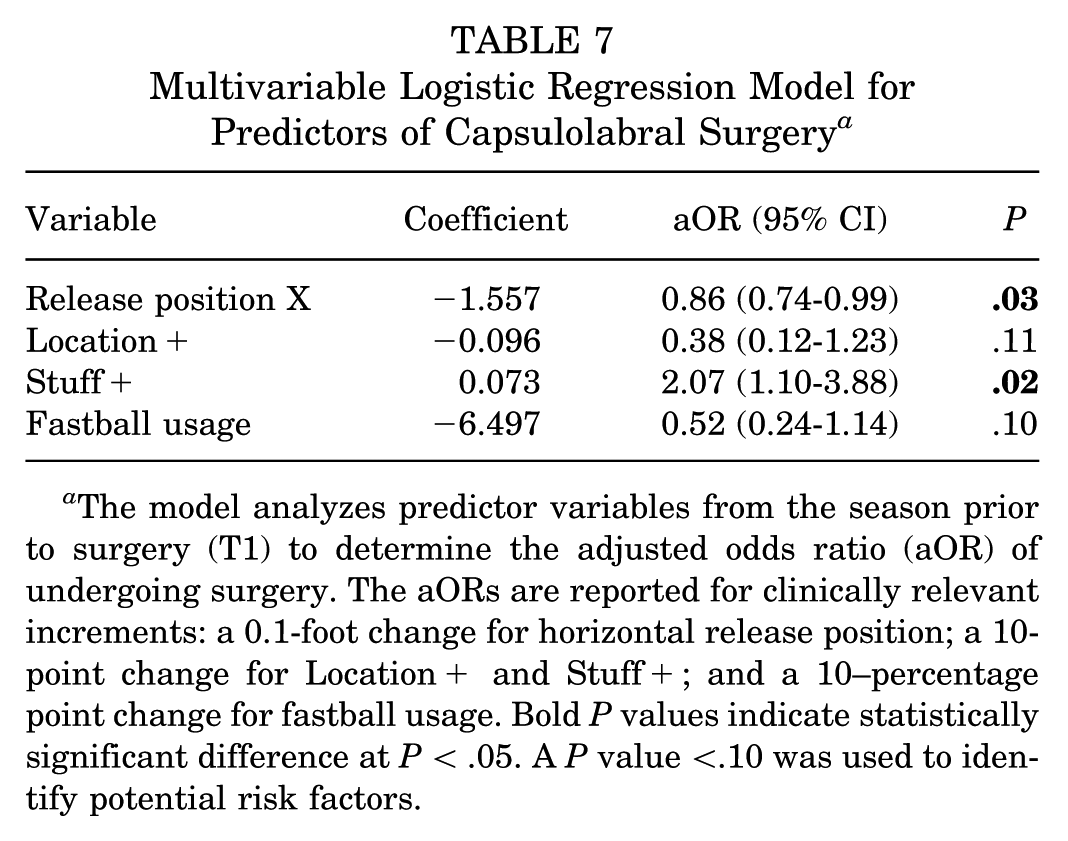
The model analyzes predictor variables from the season prior to surgery (T1) to determine the adjusted odds ratio (aOR) of undergoing surgery. The aORs are reported for clinically relevant increments: a 0.1-foot change for horizontal release position; a 10-point change for Location+ and Stuff+; and a 10–percentage point change for fastball usage. Bold P values indicate statistically significant difference at P < .05. A P value <.10 was used to identify potential risk factors.
Discussion
Several modern advanced analytic and pitch-tracking metrics were looked at as potential risk factors for capsulolabral injuries requiring repair in MLB pitchers for the first time. Pitchers who underwent capsulolabral surgery were more likely to throw harder with higher spin rates and a more medialized release point than matched controls. Injured pitchers exhibited significantly lower ERAs, superior FIP metrics, and higher player value. Overall, MLB pitchers who were more effective and had superior Stuff+ were at the highest risk for capsulolabral injuries requiring surgical intervention. These findings suggest that the very analytical metrics now driving player development and evaluation throughout the MLB, and the physical capabilities required to achieve elite scores in performance metrics, may themselves represent risk factors for debilitating shoulder injury.
The modern era of baseball has been defined by an explosion of advanced analytics that have reshaped how pitchers are evaluated and trained. Statcast and similar systems now capture every measurable aspect of pitch behavior, fueling the rise of composite “plus” metrics that integrate velocity, spin, movement, release, and other beneficial physical attributes into a single run value–based score. 27 These models, developed through machine learning and validated on large sets of pitches, have rapidly become a benchmark for both player evaluation and development. Recently, Mastroianni et al,25,27 expanded these analytics into injury research, demonstrating that pitchers who ultimately underwent UCL reconstruction possessed higher velocity, superior command (Location+), and higher overall performance (Pitching+) compared with uninjured controls, with velocity emerging as the dominant risk factor. That association reinforces decades of biomechanical work linking fastball velocity to greater elbow valgus stress,2,5,12,13,31 yet it also highlights how performance optimization and injury risk can coexist within the same domain.
Our findings parallel this broader “performance paradox” but identify a potentially distinct risk signature for the shoulder. Whereas elbow injuries appear most closely tied to pure output magnitude, measured by how hard a pitcher throws, our regression analyses revealed that Stuff+, rather than velocity or spin alone, was the strongest predictor of capsulolabral surgery. Spin can be affected by a variety of factors including arm speed and angle, release point, and grip. Spin rate has been shown to be primarily driven by arm and shoulder rotational velocity,40,48 while spin axis, direction, and efficiency is largely driven by forearm pronosupination.4,20 In baseline comparisons, all 3 variables were elevated among injured pitchers, but once entered together, the composite measure outperformed its individual components. This pattern likely reflects the differing biomechanical demands of the 2 joints. The elbow functions primarily as a hinge transmitting valgus stress, 45 where torque scales directly with velocity.21,41 The shoulder, by contrast, is a highly mobile ball-and-socket joint that relies on coordinated trunk and scapular motion, rotator cuff control, and precise sequencing to maintain stability under extreme rotational velocities.46,47 Achieving elite pitch shape and movement, the components rewarded by Stuff+, may require complex mechanical adjustments that amplify cumulative stress across these stabilizing structures. These data also suggest that overlaps may exist in risk factors or maladaptive behaviors preceding shoulder and elbow injury, and targeted interventions may lead to concurrent injury risk reduction in both throwing extremity joints.
This distinction carries important implications. Stuff+ quantifies not only how fast a pitch is thrown but how unusually it moves, by rewarding outlier spin axes, seam-shifted wake effects, and deceptive release orientations. 27 The modern developmental focus on maximizing “stuff” thus represents a biomechanical challenge as much as a performance goal. While these adaptations enhance competitiveness, our findings suggest that pursuing increasingly complex pitch characteristics may synergistically impose higher mechanical and neuromuscular demands on the shoulder. A 2024 comprehensive MLB report on pitcher injuries—developed in collaboration with team physicians, athletic trainers, orthopaedists, and biomechanists—echoed these concerns, highlighting that the league-wide emphasis on developing greater so-called stuff has likely contributed to the persistent rise in pitcher injuries. 33 Collectively, these findings support the idea that the same pitch characteristics that enhance effectiveness may also introduce mechanical instability at the shoulder, underscoring the need for studies integrating performance analytics with biomechanical monitoring to establish safer limits of optimization.
The finding of a more medial release position in pitchers who later required capsulolabral surgery identifies a visible kinematic difference, but its underlying meaning remains uncertain. Because horizontal release can be affected by where a pitcher stands on the rubber, stride direction, and trunk or arm orientation, 38 this observation likely reflects an interplay of multiple mechanical factors rather than a single motion fault. Prior research has also produced conflicting results regarding its relationship to injury: some studies have linked a more medial release to increased UCL risk,24,48 whereas others have shown either no association, 24 or an opposite trend toward greater risk with more lateral release points. 38 The lack of consistency across studies suggests that horizontal release position is a proxy capturing complex whole-body motion patterns, and that its contribution to injury risk likely depends on how it interacts with other mechanical variables.
One feature distinguishing this analysis from prior work was the inclusion of Statcast's arm-angle metric, a recently introduced anatomically grounded measure of throwing orientation. 40 While acute UCL injuries have been linked to abrupt drops in arm angle, 9 and chronic injuries to greater pitch-to-pitch variability, 26 this study found no between-group differences in this measure. The combination of a more medial release point but similar arm angles between groups suggests that the difference arose not from changes in arm slot itself, but from altered trunk mechanics, particularly contralateral trunk tilt. When a pitcher leans the torso toward the glove side during delivery, the entire shoulder complex shifts toward the midline,22,35 moving the release point medially without necessarily changing arm angle. This pattern has become common in velocity-focused training, as increased trunk lean has been associated with higher pitch speeds, but it has also been shown to elevate shoulder and elbow loading forces and association with injury risk.3,17,35,43,49,50 The interplay between trunk tilt and arm slot therefore provides a more comprehensive framework for interpreting these findings. Interestingly, Escamilla et al, 11 found that pitchers with moderate trunk tilt experienced the greatest shoulder and elbow torques, even exceeding those of extreme overhand or sidearm deliveries. This reinforces that isolated kinematic variables, such as release position or arm angle alone, cannot reliably explain injury risk without considering their combined mechanical context. The present results should thus be viewed as evidence that certain trunk-arm coordination patterns may manifest as measurable release differences, but the precise causal pathways remain unclear. Future studies integrating motion capture biomechanics with large-scale tracking data and injury histories are needed to clarify how these variables interact to influence shoulder stress and to determine whether observable changes in release position can serve as early indicators of pathologic adaptation.
Notably, several variables investigated showed no association with capsulolabral injury risk despite receiving substantial attention in injury prevention discourse. Pitch count showed no difference between groups, nor did we detect differences in release extension, approach angles, or pitch movement patterns. The absence of workload effects does not diminish the importance of load management; substantial evidence supports pitch count restrictions in reducing injury risk broadly, especially for young athletes,18,20,25,34,37 but suggests that how a pitcher throws may matter as much as volume. Similarly, our longitudinal analysis revealed no significant differences in season-to-season changes for most variables, with cases and controls showing similar trajectories in velocity, spin, and performance metrics leading up to surgery. This suggests that cross-sectional characteristics, what a pitcher throws, may be more predictive than rates of change; however, larger prospective studies with higher temporal resolution, particularly monitoring offseason training periods where dramatic improvements often occur, are needed to definitively address this question.
Practical applications emerge from these findings, as they arrive at a pivotal moment in baseball's evolution. While shoulder capsulolabral surgeries are still relatively uncommon compared with elbow UCL surgery, pitch tracking and other motion capture systems can play key roles in identifying trends indicative of or leading to injury. Modern training facilities employ high-speed cameras, force plates, and motion capture systems providing real-time feedback on how mechanical adjustments affect measurable metrics, enabling pitchers to experiment with different release points, grips, and body positions while observing immediate changes in pitch characteristics. Teams might implement enhanced monitoring for pitchers exhibiting elevated Stuff+ scores or excessive medialization of release position. Strength and conditioning programs might emphasize rotator cuff endurance, scapular stabilization, and posterior shoulder strengthening for high-risk populations. Most fundamentally, these findings suggest that injury prevention strategies must evolve alongside the analytical revolution transforming player development, moving beyond simple workload management toward comprehensive consideration of how biomechanical demands interact with individual tissue tolerance to determine injury risk. Whether targeted interventions can mitigate risk while preserving performance gains remains unknown and represents a critical avenue for future research.
Limitations
This study's findings must be interpreted within the context of its methodological constraints, which are inherent to its retrospective design and public data sources. A primary consideration is that the investigative framework, being retrospective in nature, does not permit the establishment of causal relationships between the identified mechanical factors and the subsequent incidence of injury. This limitation is compounded by our reliance on publicly available injury reports, which, while providing a valuable population-level data set, introduces several specific challenges. The timing of injury onset was necessarily approximated from these reports and may not precisely coincide with the actual symptomatic onset experienced by the athlete. Similarly, this also made it difficult to discern whether cases had more insidious and atraumatic onset of symptoms or if there was an acute traumatic injury. We also assume that our matched controls are asymptomatic and uninjured based off the lack of injury reports confirmed in the media. Furthermore, this data source did not afford access to granular surgical or clinical details, such as the specific location and severity of the labral tear, degree of bone loss, or the technical details of the procedures performed. It is also critical to recognize that the pitching metrics derived from Statcast data are exclusively representative of external kinematics. These data do not capture the internal joint loading, muscle activation patterns, or direct ligamentous strains that constitute the true pathomechanical pathway to injury. Consequently, the mechanical alterations we report should be understood as correlates of injury risk rather than as direct measurements of excessive tissue stress. Furthermore, our multivariable regression models were limited by a reduced sample size. The key composite metrics, Stuff+ and Location+, have only been publicly available since 2020, restricting the cohort for these model cases and controls with complete data. This smaller sample reduces the models' statistical power and widens their confidence intervals, and the findings should be interpreted with this constraint in mind. Given this study only included professional baseball players, the generalizability of our findings may be difficult to apply across all baseball levels where access to pitch tracking is not as obtainable. Finally, the absence of clinical information, such as reported levels of pain, fatigue, or functional limitations, precluded our ability to correlate these objective mechanical deviations with the subjective complaints that are foundational to clinical evaluation and management. While this gap currently restricts the direct translation of our findings into clinical practice, the identification of objective mechanical markers represents a critical preliminary step. Future research directions that successfully integrate these kinematic profiles with athlete-reported outcomes and data from wearable sensor technologies will be essential to bridge this divide and more directly link external mechanics with internal loading and symptomatic progression.
Conclusion
Pitchers who underwent capsulolabral surgery were more likely to throw harder with higher spin rates and a more medialized release point than matched controls. Overall, MLB pitchers who were more effective and had superior Stuff+ were at the highest risk for shoulder instability requiring surgical intervention. These findings suggest that the very analytical metrics now driving player development and evaluation throughout the MLB, and the physical capabilities required to achieve elite scores in performance metrics, may themselves represent risk factors for debilitating shoulder injury.
Footnotes
Final revision submitted December 28, 2025; accepted January 2, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.A. is a paid consultant and receives royalties from Arthrex; he also serves as the head team physician of the New York Yankees. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Columbia University Medical Center.