
Abstract
Background:
Early cocking phase pitching mechanics may affect risk of upper extremity injury requiring surgery in professional baseball players.
Purpose:
To assess the occurrence of inverted-W arm positioning and early trunk rotation in Major League Baseball (MLB) pitchers and to determine whether this throwing position is associated with upper extremity injury requiring surgery.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
For 250 MLB pitchers in the 2010 season, 15 to 20 pitches from the start and end of an outing were reviewed using slow-motion game video for presence of an inverted-W position and early trunk rotation. Previous or current incidence of upper extremity injury requiring surgery for each player was determined using the MLB injury database, minor league injury records, available collegiate data, and publicly available online injury databases. Upper extremity surgery associated with an injury was considered to result from pitching.
Results:
Consensus between investigators was achieved for 99% of players for inverted-W positioning (248 players) and in 97% of players for early trunk rotation (243 players) for videos reviewed independently. Rate of surgery with and without inverted-W position was 28 of 93 (30%) and 42 of 155 (27%), respectively. Rate of surgery with and without early trunk rotation was 37 of 111 (33%) and 30 of 132 (23%), respectively. Using a Cox proportional hazards model for risk analysis using the measured number of innings pitched at time of surgery as an approximate index of exposure and adjusting for age and fastball speed at time of surgery, early trunk rotation was associated with significantly increased risk of shoulder and/or elbow surgery with hazard ratio estimate of 1.69 (95% CI, 1.02-2.80). Presence of the inverted-W position was not associated with significantly increased risk (hazard ratio, 1.30; 95% CI, 0.79-2.14).
Conclusion:
The inverted-W throwing position was not associated with significantly greater risk of upper extremity injury requiring surgery in MLB pitchers. Early trunk rotation was associated with significantly elevated risk of injury requiring surgery.
Potential energy is gathered in the early cocking phase of the throwing motion 5,9 –11 and released in the late cocking/early acceleration phase. The repetitive nature of pitching and the extreme forces generated makes these athletes highly susceptible to injury and has led to a reported 50% incidence of pain sufficient to prevent professional pitchers from throwing at some point in their careers. 9 The inverted-W, defined as hyperabduction of both the throwing and nonthrowing shoulder combined with internal rotation, 7 occurs shortly after hand separation during the early cocking phase of the throwing motion and has been associated anecdotally with injury risk in pitchers. 7 Compared with a standard throwing motion, the throwing arm in this position has to travel a greater distance to arrive in the vertical position by the time the trunk begins rotating toward home plate. Failure of the throwing arm to arrive in the vertical position before the trunk begins to rotate has been postulated to cause excessive forces in the arm. 10 Furthermore, rotation of the trunk ideally occurs after planting of the lead foot in this phase of the throwing motion. 1 Early trunk rotation dissipates some of the potential energy needed to generate a given throwing velocity and has been shown to increase valgus torque at the elbow. 1 It is not known whether the inverted-W position or early trunk rotation is associated with injury requiring surgery in professional baseball players.
Biomechanical and observational studies have reported on factors that may put the shoulder and elbow at risk of injury. A recent study of high school baseball pitchers found that participants with greater contralateral trunk lean showed adverse effects on the throwing arm, such as higher peak elbow varus moment. 8 Aguinaldo and Chambers 1 found that pitchers who rotated their trunk toward home plate later in the pitching cycle generated lower torque in the throwing arm. DiGiovine et al 4 showed that pitchers with less shoulder abduction at stride foot contact after the early cocking phase have decreased valgus stresses at the elbow, whereas elbow valgus stresses were increased with increasing degrees of shoulder abduction. In a study of youth baseball pitching mechanics, Davis et al 3 found decreased humeral internal rotation torques and elbow valgus loads during a fastball pitch when more of the “correct” biomechanical parameters were observed. Bushnell et al 2 used 3-dimensional motion analysis to study fastball velocity and rates of injury in 23 professional pitchers. They found that pitchers with higher fastball speed had a statistically higher incidence of clinically apparent elbow injury. No study has yet assessed the association between pitching mechanics and injury requiring surgery in a larger group of professional players.
The purpose of this study was to determine whether inverted-W arm positioning (hyperabduction with internal rotation of the throwing arm) or early trunk rotation was associated with upper extremity injury requiring surgery for starting Major League Baseball (MLB) pitchers from a single season.
Methods
A total of 250 starting MLB pitchers for the 2010 season were included in the study and were assessed for presence or absence of the pitching positions being investigated. Data on upper extremity injury associated with surgery during the professional career were collected through the end of the 2010 regular baseball season. Institutional review board approval for the study was obtained.
Video for each pitcher was analyzed for inverted-W positioning and early trunk rotation. The inverted-W position was defined as the elevation of 1 or both elbows above shoulder level in the early cocking phase of the throwing motion (Figure 1). Early trunk rotation was defined as trunk rotation before the stride foot hit the ground and occurrence of nonvertical arm position at initiation of trunk rotation (Figure 2).

Hyperabduction with internal rotation during early cocking phase.

Early trunk rotation during early cocking phase.
These pitching mechanics were studied in 15 to 20 pitches from the start and end of an outing using game film recorded from a conventional center field vantage point. Pitches from the start and end of an outing were reviewed to determine whether throwing position was consistent throughout the outing. The standardized center field vantage point provided a clear view of the angle of the arm.
The senior investigator (W.A.D.) and 1 other investigator (D.L.D.) reviewed the films independently and were blinded to each other. These investigators are associated with medical care of an MLB team and are familiar with professional baseball pitching. Identification of the inverted-W position was based on visual identification of gross hyperabduction of both the throwing and nonthrowing shoulder combined with internal rotation shortly after hand separation during the early cocking phase of the throwing motion. Identification of early trunk rotation was based on gross identification of timing of trunk rotation in relation to planting of the lead foot. Investigators used slow-motion playback to assess whether inverted-W positioning and early trunk rotation were present in the early cocking phase. The 2 investigators determined the percentage of players where they had consensus on presence or absence of the positions being evaluated and then reviewed the remaining videos to determine whether they could come to consensus on additional players.
We then identified the incidence of shoulder or elbow injury requiring surgery during the professional career for each MLB pitcher through the end of the 2010 regular baseball season based on publicly available online MLB injury databases. Upper extremity injury requiring surgery was the endpoint for this study. For each player, we used publically available online major and minor league data and collegiate data where applicable to determine innings pitched up to the time of injury requiring surgery. The amount of work a pitcher had completed up to the time of upper extremity injury requiring surgery was based on professional and collegiate innings pitched. These data are often used by medical and executive staff to determine player workload and can provide background information regarding player health. We excluded surgeries not related to the upper extremity and any upper extremity surgery resulting from injury identified as resulting from a nonbaseball event. For the purposes of this study, upper extremity surgery associated with an upper extremity injury was considered to represent injury resulting from pitching.
Statistical Analysis
The association between surgery and pitching mechanics status was examined with multivariable Cox proportional hazards regression models, using the measured number of innings pitched as an approximate index of exposure and adjusting for average measured fastball speed and age at the beginning of the 2010 season. All statistical analyses were conducted using R statistical software (v 2.13.0; R Foundation for Statistical Computing).
Results
The mean player age was 27 ± 4 years based on age at upper extremity surgery for players with surgery and age at the end of the regular 2010 baseball season for players with no surgery. The 2 investigators achieved consensus on pitchers in 88% (220/250) of players screened for the inverted-W position and in 86% (215/250) of players screened for early trunk rotation. After additional review of the videos where consensus was not reached, we achieved consensus in 99% of players for the inverted-W position (248 players) and in 97% of players for early trunk rotation (243 players).
Each player showed the same mechanics in all pitches in the outing reviewed. The rates of surgery are shown in Table 1. Upper extremity surgery in players was performed in 78 of 250 pitchers (31%) in the shoulder (n = 24), elbow (n = 53), and wrist (n = 1).
Rate of Upper Extremity Surgery
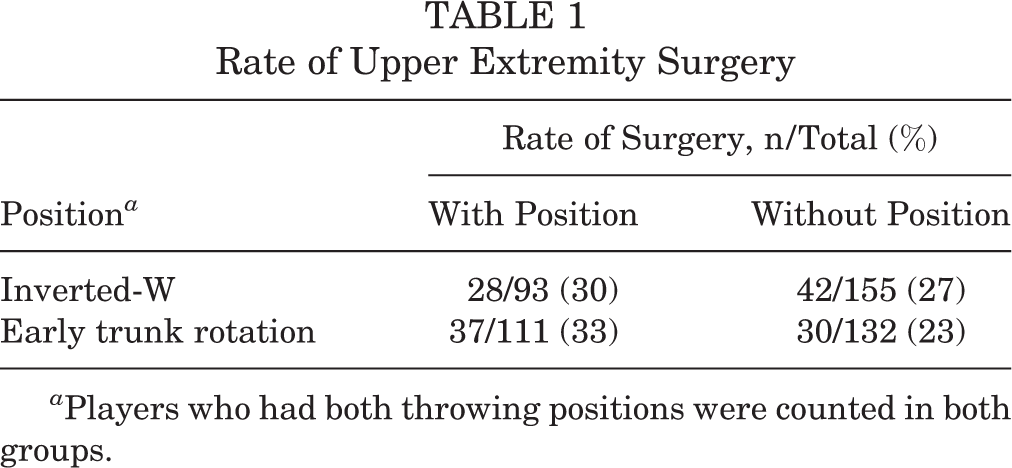
a Players who had both throwing positions were counted in both groups.
Using a hazards model for risk analysis with the measured number of innings pitched before surgery as an approximate index of exposure and adjusting for age and fastball speed at surgery, 2 inverted-W positioning was not associated with significantly increased risk of surgery using risk analysis (hazard ratio estimate, 1.30; 95% CI, 0.79-2.14). The presence of early trunk rotation was associated with significantly increased risk of surgery (hazard ratio, 1.69; 95% CI, 1.02-2.80).
Discussion
Based on video analysis of MLB pitchers and on surgery data from publically available databases, significantly elevated risk of injury requiring surgery was found with early trunk rotation but not with the inverted-W throwing position. Our findings suggest that early trunk rotation raises concerns that warrant the attention of athletes and physicians and that the inverted-W throwing position does not represent a clear area of concern for possible injury with the intense, repetitive stresses of throwing.
The current findings add surgery risk data to biomechanical and observational studies that have reported on factors that contribute to adverse biomechanics and may put the shoulder and elbow at risk of injury in the throwing motion. A recent study of 72 high school baseball pitchers found that participants with greater contralateral trunk lean threw with greater velocity, but also showed higher peak throwing arm elbow varus moment, higher peak shoulder rotation moment, and lower torso forward flexion angles. 8 Mihata et al 6 simulated posteroinferior capsular tightness and resulting glenohumeral internal rotation deficit in cadavers with the shoulder abducted at 90° and at maximum external rotation (simulated late cocking phase). These investigators found significantly increased glenohumeral contact pressure, significantly decreased impinged area of rotator cuff tendon, and significant posterior shift of the humeral head with shoulder internal impingement. Aguinaldo and Chambers 1 found higher torque values about the elbow with lower maximum shoulder external rotation and lower elbow flexion in the late cocking/early acceleration phase of the throwing motion. They also reported lower torque in the throwing arm in pitchers who rotated their trunk later in the pitching motion. DiGiovine et al 4 showed that pitchers with less shoulder abduction at stride foot contact had decreased valgus stresses at the elbow, whereas elbow valgus stresses were increased with increasing degrees of shoulder abduction. Davis et al 3 found decreased humeral internal rotation torques and elbow valgus loads during a fastball pitch in youth players when more of the “correct” biomechanical parameters were observed.
As described by Tullos and King, 10 the cocking phase of the throwing motion begins at the end of the wind-up when the hands separate and continues to the moment before acceleration when the shoulder is in maximum external rotation. Averaging only 1.5 seconds in duration, this phase is divided into early and late cocking and comprises almost 80% of the pitching motion. 9 The cocking phase provides the biomechanical preparation for the acceleration phase of the throwing motion, where the greatest forces are expended. It is possible that injury requiring surgery occurs significantly more frequently with early trunk rotation because the throwing arm cannot safely or efficiently take advantage of the potential energy generated in the cocking phase of the throwing motion. Because the throwing arm does not get into the ideal position in time, it is possible that the acceleration phase of the throw may then involve a sudden late whipping action of the throwing arm with increased torque on the shoulder and elbow.
The methodology used in this study could be employed to assess possible injury and surgery risk associated with a given throwing practice. The ability to assess large groups of players at a given point in time offers a valuable addition to available data. Prospective studies offer the benefit of close observation of injury associated with a given practice over time, but for practical reasons, these studies are limited to smaller groups of players. In a study of 23 professional pitchers, Bushnell et al 2 used 3-dimensional motion analysis and assessed maximum pitch velocity. By following these pitchers over the next 3 seasons, these investigators found a statistically higher incidence of injury to the throwing elbow in pitchers with higher fastball speeds. Although the current methodology does not have the scientific rigor of a prospective study, it has the practical potential to systematically assess possible injury risk in a relatively large number of players. The throwing positions assessed in this study involved gross movement patterns easily identified on video by experts in the sport. Because official databases were used, no subjectivity was involved in determining whether surgery to the upper extremity had occurred. The methods used in this study could be improved in future investigations by use of independent observers to rate the videos. The current methods do not establish causality and do not eliminate possible outside factors influencing injury risk to these players, but they provide a useful basis for alerting players and teams to a need for further more detailed study of injury and surgery potential.
There were a number of limitations to this study. Because this was a retrospective study, we were limited to use of available data. However, we were able to obtain essential data such as major and minor league innings pitched, average fastball speed, and time from start of professional career to injury. A prospective analysis would provide useful detail on the exact type and quantity of pitches thrown and might accurately predict risk of injury requiring surgery. The findings apply only to starting pitchers and cannot be extrapolated to relief pitchers. We focused on starting pitchers to examine risk of injury requiring surgery with a consistent pitching load, and we assumed that pitchers had the same throwing mechanics over time, based on anecdotal observations in the profession. We did not attempt to determine whether there was a specific angle of hyperabduction beyond which injury risk may increase, nor did we have access to innings pitched or upper extremity surgery data for the precollegiate or preprofessional period of players’ careers. Pitching workload before a player reached the professional level may have had an impact on injury risk. In addition, we may not have had adequate power to identify significantly increased risk of injury requiring surgery with the inverted-W position, although we evaluated a large number of pitchers. We did not have adequate power to assess injury risk for players with both the inverted-W position and early trunk rotation. Finally, we did not assess lost playing time associated with injury that did not result in surgery.
Using video analysis and publicly available injury databases, we found significantly elevated risk of upper extremity injury requiring surgery with early trunk rotation but not with the inverted-W throwing position.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: W.A.D. received an unrestricted educational grant from Arthrex Inc, from which funds were used to support this study.
Acknowledgment
The authors thank Reginald E. Dunn, MA, of MedStar Sports Medicine Research Center for statistical analysis; Brian Mata, MD, for expert review of the manuscript; and Lyn Camire, MA, ELS, of MedStar Union Memorial Hospital for editorial assistance.