
Abstract
Background:
Variable return-to-play (RTP) rates have been reported after surgical repair of superior labral anterior-posterior (SLAP) tears in baseball players. Many studies, however, have not controlled for concomitant shoulder injuries.
Purpose/Hypothesis:
The purpose of this study was to evaluate rates of RTP and return to previous or higher performance level (RTPP) and long-term outcomes after isolated SLAP tear repair. The hypothesis was that improved outcomes would be identified compared with previous reports.
Study Design:
Case series; Level of evidence, 4.
Methods:
The records of 232 players who underwent isolated SLAP tear repair from 2004 to 2014 were reviewed. A total of 98 players who were at least 12 months out from surgery were identified. Through telephone interviews, participants completed the Western Ontario Shoulder Instability Index (WOSI) and Veterans RAND 12-Item Health Survey (VR-12) and answered scripted questions about RTP, RTPP, and current symptoms.
Results:
Of the 98 players who met the inclusion criteria, 73 (74.5%) participated. The mean age at the time of surgery was 19.8 ± 2.9 years. The mean follow-up time was 86.2 ± 25.1 months overall; it was 84.4 ± 24.4 months for pitchers and 90.3 ± 26.7 months for other position players, (P = .40). There were 10 professional, 36 collegiate, and 27 high school players. Most players perceived successful RTP (83.6%), including 80.0% of pitchers and 91.3% of other position players (P = .23). However, RTPP rates were lower, at 52.3% (n = 26) and 78.3% (n = 18) for pitchers and other position players, respectively (P = .03). Pitchers were younger at the time of surgery (19.3 ± 3.0 vs 20.8 ± 3.0 years, respectively; P = .03) and had greater perceived shoulder and general health impairments compared with other position players (P ≤ .02). Players who perceived successful RTPP had better WOSI of the healthy shoulder and individual physical, sports, lifestyle, and emotion scores compared with players who did not perceive successful RTPP.
Conclusion:
After the surgical repair of isolated type II or greater SLAP tears, other position players displayed superior RTP (91.3% vs 80.0%, respectively) and RTPP (78.3% vs 52.3%, respectively) rates than pitchers. Long-term follow-up suggests that pitchers may perceive greater long-term impairments than other position players and are less likely to return to their previous or higher performance level.
Since Andrews et al 1 initially described anterosuperior glenoid labrum tears associated with long head of the biceps brachii tendon loading forces in throwing athletes, shoulder surgeons have debated treatment options. Although nonoperative superior labral anterior-posterior (SLAP) tear treatment can be effective, 20 surgical repair and rehabilitation are recommended in younger, active patients, particularly overhead-throwing athletes. § Few studies, however, have specifically evaluated baseball players, and none have attempted to solely focus on baseball players with an isolated SLAP tear that had not progressed to rotator cuff defects or other concomitant shoulder injuries.
In a systematic review of 506 athletes after type II SLAP tear repair, Sayde et al 27 reported that of the overall patient group, 73% (range, 22%-92%) returned to their previous level of play; however, only 63% of 198 overhead athletes (including 81 baseball players) returned to their previous level of play. Gorantla et al 16 reported that the percentage of baseball players who returned to their previous level of play after type II SLAP tear repair ranged from 22% to 64%. Among baseball players who underwent SLAP repair, Fedoriw et al 12 reported that 48% (13/27) of pitchers treated surgically returned to play; however, only 7% (2/27) returned to their previous or higher performance level. For other position players who were treated surgically, 85% (11/13) returned to play, and 54% (7/13) returned to their previous or higher performance level. In a 10-year follow-up study involving 133 baseball players after SLAP repair, Gilliam et al 15 reported a return-to-play (RTP) rate of 62%; however, their study did not identify patients who solely had SLAP tears.
This wide outcome discrepancy in studies of athletes who have undergone SLAP tear repair makes it difficult to use this information to help guide patient care decision making. Diverse study participants, small sample sizes, a limited number of baseball players, and the pooling of data from patients with widely ranging concomitant shoulder injuries and surgical procedures have made it difficult to ascertain the true perceived functional status of baseball pitchers and other position players after isolated repair of SLAP tears. The purpose of the current study was therefore to advance our understanding of outcomes after isolated SLAP tear repair in baseball players, specifically pitchers compared with other position players. We hypothesized that baseball pitchers and other position players who had undergone isolated SLAP repair would have higher rates of RTP and return to previous or higher performance level (RTPP) than previously reported.
Methods
Research ethics committee approval was sought and obtained for this study. An initial cohort of 232 baseball players who underwent arthroscopic SLAP repair from 2004 to 2014 was identified for possible study inclusion. Before undergoing surgical repair, all potential study participants had participated in a comprehensive conservative rehabilitation program. The conservative treatment consisted of a 3- to 6-month course of progressive glenohumeral joint range of motion, posterior capsuloligamentous stretching, scapulothoracic stabilization, and upper extremity–core strengthening exercises administered either by a physical therapist or by a certified athletic trainer well versed in these concepts and in baseball throwing mechanics. The surgical treatment option was implemented only after it was determined that participants could not successfully return to play after comprehensive conservative rehabilitation.
All SLAP tear repairs were performed arthroscopically by the senior authors (J.A., R.O.) using an identical surgical approach and technique, as described by Wilk et al. 31 No knotless repairs were included in the study group, as knotless repair techniques had not yet achieved widespread adoption. Postoperative rehabilitation consisted of a 6- to 9-month course of progressive glenohumeral joint range of motion; scapulothoracic rhythmic stabilization; and core mobility, strength, and coordination therapeutic exercises. Phases of 1- to 6-week duration were generally adhered to, progressing from an immediate postoperative protected motion phase, intermediate moderate protection phase, minimal protection phase with the initiation of an interval-throwing program, advanced strengthening phase, and gradual return-to-activity phase. 22,31
Study Population
Patients who were not baseball players at the high school, collegiate, or professional level at the time of injury were excluded from study participation. Additionally, patients with concomitant shoulder defects such as partial- or full-thickness rotator cuff tears, anterior glenohumeral joint instability, labral tears extending outside of the 11- to 1-o’clock position, glenohumeral joint impingement, and acromioclavicular joint osteoarthritis were also excluded. Last, patients were excluded from study participation if they had not been cleared to return to competitive baseball after surgery and rehabilitation because they were less than 12 months out from surgery (n = 17) or if they had undergone any other shoulder surgical procedures such as long head of the biceps brachii tenodesis or tenotomy, subacromial decompression, or distal clavicle excision (n = 50). Of the initial cohort of 232 patients who underwent SLAP repair during the study period, 98 met the inclusion criteria, and of those patients, 73 were successfully contacted, agreed to study participation, and provided informed consent (Figure 1). This final study cohort only represented the subset of participants from a previous report 15 who had an isolated SLAP tear; we excluded those patients who also had rotator cuff or other shoulder injuries.
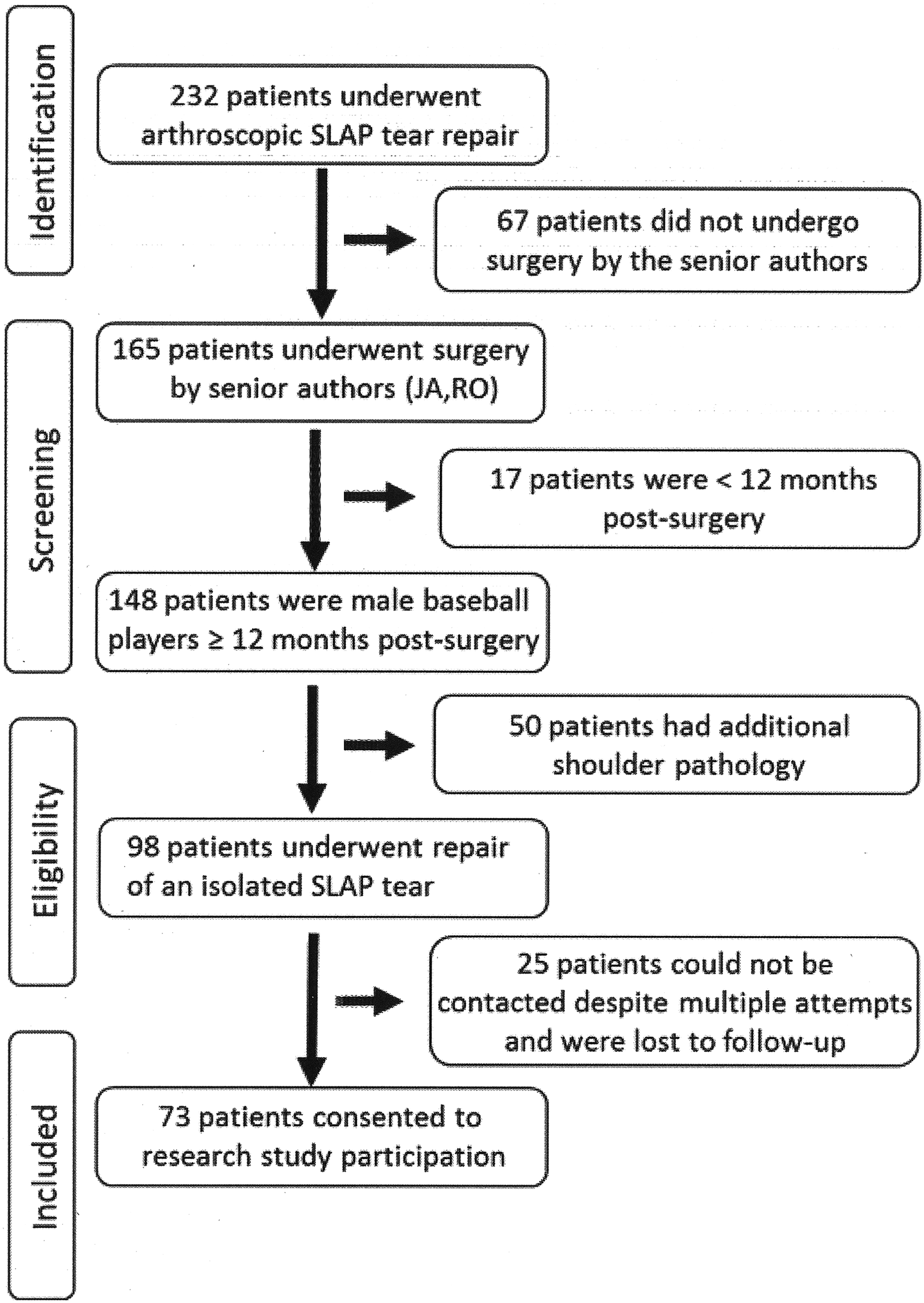
Flow diagram of study participant selection. SLAP, superior labral anterior-posterior.
Telephone Survey
The primary investigator (L.D.) contacted each study participant by telephone and asked him to verbally answer questions that evaluated outcomes after isolated SLAP tear repair. The Western Ontario Shoulder Instability Index (WOSI) 30 and the Veterans RAND 12-Item Health Survey (VR-12) 15,28 were used to assess patient perceptions of overall shoulder function in the presence of instability and general physical and mental health, respectively. Additional scripted questions were also asked to obtain patient perceptions of RTP, RTPP, and highest level of play. Patient perceptions of successful RTP were determined by their response to the following dichotomous question: “Did you return to baseball play after surgery (yes or no)?” Patient perceptions of successful RTPP were determined by their response to the following dichotomous question: “Were you able to return to play at the same or higher level (yes or no)?” Highest level of play represented patient perceptions of the most advanced level that they were able to achieve after the index SLAP repair (recreational, youth league, high school, collegiate, professional minor league, or professional major league).
Statistical Analysis
Statistical analysis was performed using SPSS version 24.0 software (IBM). Patient responses to the 2100-point WOSI score were converted to a perceived shoulder function indicator relative to the healthy shoulder, with a maximum (best) score of 100%. Individual WOSI physical, sports, lifestyle, and emotion domain scores were also determined, with higher scores representing greater perceived shoulder impairment levels. VR-12 physical and mental health subscale scores were used to determine patient perceptions of general or overall physical and mental health. The Shapiro-Wilk (2-group comparisons) and Kolmogorov-Smirnov (3-group comparisons) tests were performed to determine data normality. Because these data did not display a normal distribution, nonparametric statistical analysis was performed. A series of 1-way Kruskal-Wallis analyses of variance were used to determine the influence of baseball playing level on perceived shoulder function and general health. For all other 2-group continuous data comparisons (pitchers vs other position players, RTP, and RTPP) for perceived shoulder function and general health, we relied on the Mann-Whitney U test. Proportional frequency comparisons for RTP and RTPP between pitchers and other position players were evaluated with the chi-square or Fisher exact test. If participants stated that they did not achieve RTP or RTPP, they were asked to provide additional information, such as whether they had experienced any shoulder pain, stiffness, or weakness as contributing factors. An alpha level of P < .05 was selected to indicate statistical significance.
Results
Of the 98 baseball players who qualified for study participation, the primary investigator was able to contact 73 patients who consented to study participation (74.5% response rate). All respondents had been treated for an isolated SLAP tear. Tears were classified as type II (n = 69), type III (n = 3), and type IV (n = 1). A total of 233 suture anchors were used (mean, 3.2 ± 1.2 anchors/procedure). Most anchors were bioresorbable (n = 189); however, PEEK (n = 23) and suture-based polyester anchors (n = 21) were also used. Each anchor was double loaded. The mean follow-up time was 7.2 ± 2.1 years (range, 1.9-11.0 years). Study participants were 37.0% (n = 27) high school players, 49.3% (n = 36) collegiate players, and 13.7% (n = 10) major or minor league professional players. Regarding position, 68.5% (n = 50) were pitchers, 13.7% (n = 10) were infielders, 12.3% (n = 9) were outfielders, and 5.5% (n = 4) were catchers. The follow-up evaluation took place at a mean of 84.4 ± 24.4 months postoperatively for pitchers and 90.3 ± 26.7 months for other position players (P = .40). The mean age at the time of surgery was 19.3 ± 3.0 years for pitchers and 20.8 ± 3.0 years for other position players (P = .03). Overall, 32.9% (n = 24) of participants were either still actively playing baseball at follow-up or were otherwise engaged in overhead throwing on a consistent basis, such as coaching.
Level of Play Comparisons
Comparisons by playing level failed to reveal differences for perceived shoulder function and general health variables between high school, collegiate, and professional players (Table 1). Age at the time of surgery differed for each group, and professional athletes had a longer follow-up time compared with high school and collegiate players. Overall, 83.6% (61/73) of the participants reported RTP, and differences did not exist between playing levels. Overall, 60.3% (44/73) of players perceived RTPP, and likewise, differences did not exist between playing levels.
Comparisons by Playing Level a
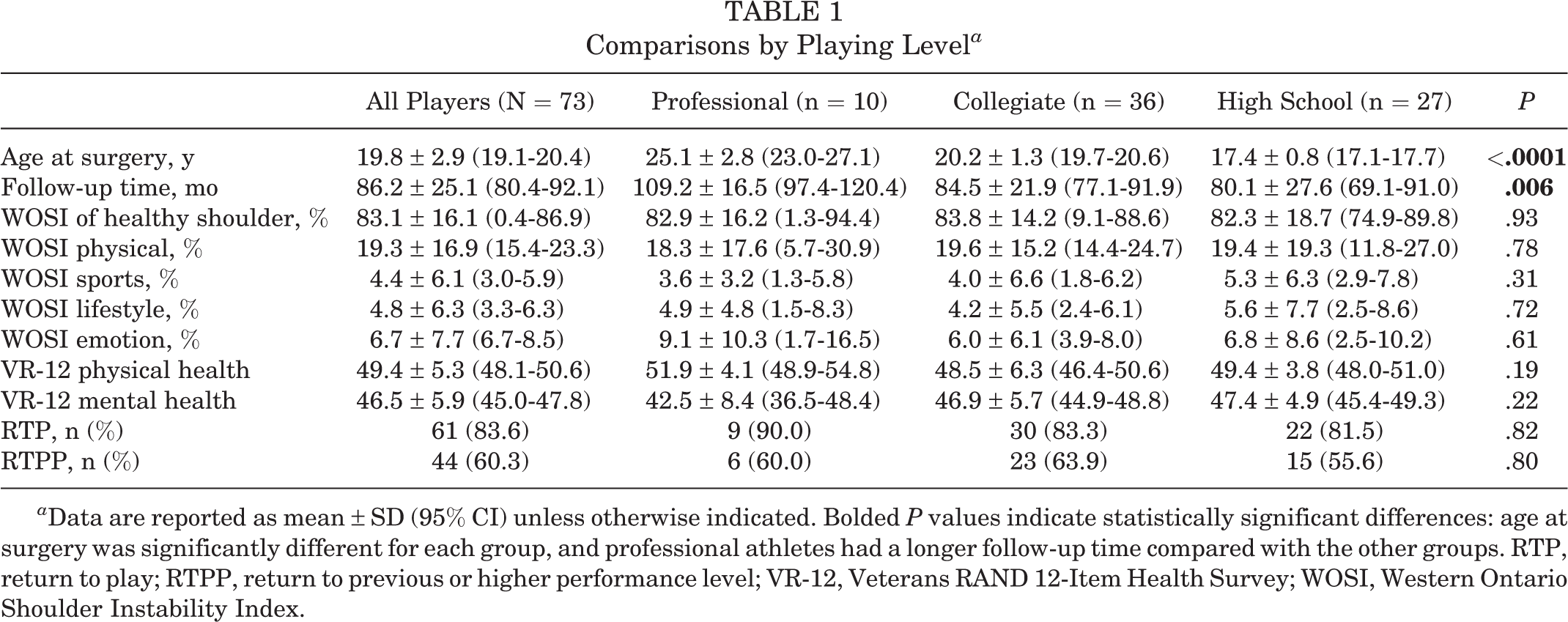
a Data are reported as mean ± SD (95% CI) unless otherwise indicated. Bolded P values indicate statistically significant differences: age at surgery was significantly different for each group, and professional athletes had a longer follow-up time compared with the other groups. RTP, return to play; RTPP, return to previous or higher performance level; VR-12, Veterans RAND 12-Item Health Survey; WOSI, Western Ontario Shoulder Instability Index.
Pitcher and Other Position Player Comparisons
Comparisons between pitchers and other position players revealed that pitchers were significantly younger at the time of surgery (P = .03), were comparable in follow-up time, had greater perceived impairments during sports function (P = .002), and had greater perceived overall physical health impairments (P = .02) compared with other position players (Table 2 and Figure 2). Although pitchers did not display a significant difference in RTP rate compared with other position players, other position players perceived a greater rate of RTPP compared with pitchers (78.3% vs 52.3%, respectively; P = .03). Of the 24 pitchers who did not achieve RTPP, the main reasons cited included shoulder stiffness or tightness (45.8%, 11/24), pain (45.8%, 11/24), and weakness (37.5%, 9/24) as the primary factors. Only 2 pitchers (8.3%, 2/24) perceived shoulder instability or laxity. Five pitchers changed to a different position when they returned to baseball. The follow-up time did not influence RTP or RTPP rates (P ≥ .50).
Comparisons by Pitchers and Other Position Players a

a Data are reported as mean ± SD (95% CI) unless otherwise indicated. Bolded P values indicate statistically significant between-group differences (P < .05). RTP, return to play; RTPP, return to previous or higher performance level; VR-12, Veterans RAND 12-Item Health Survey; WOSI, Western Ontario Shoulder Instability Index.

Pitchers perceived greater overall physical health impairments at follow-up compared with other position players (*P = .02)..
RTP and RTPP Comparisons
There were no statistically significant differences in any perceived shoulder function or general health variable between players who reported successful RTP versus those who did not. Likewise, there were no differences between these 2 groups in age at surgery or in follow-up time (Table 3). Comparisons between baseball players who perceived RTPP versus those who did not revealed multiple group differences for perceived shoulder function (Table 4). Players who perceived RTPP had better WOSI of the healthy shoulder as well as better individual physical, sports, lifestyle, and emotion scores compared with players who did not (P < .05 for all) (Table 4 and Figure 3).
Comparisons by RTP After Isolated SLAP Tear Repair a

a Data are reported as mean ± SD (95% CI). RTP, return to play; SLAP, superior labral anterior-posterior; VR-12, Veterans RAND 12-Item Health Survey; WOSI, Western Ontario Shoulder Instability Index.
Comparisons by RTPP After Isolated SLAP Tear Repair a
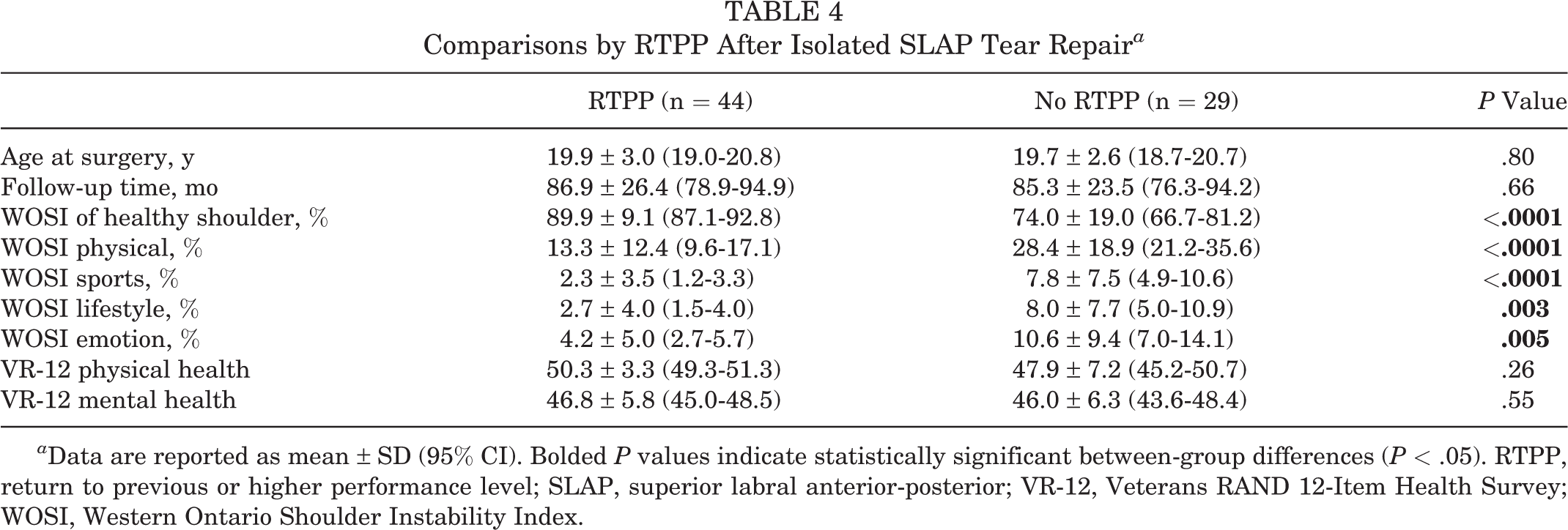
a Data are reported as mean ± SD (95% CI). Bolded P values indicate statistically significant between-group differences (P < .05). RTPP, return to previous or higher performance level; SLAP, superior labral anterior-posterior; VR-12, Veterans RAND 12-Item Health Survey; WOSI, Western Ontario Shoulder Instability Index.

Players who perceived return to previous or higher performance level (RTPP) had better Western Ontario Shoulder Instability Index (WOSI) of the healthy shoulder and individual physical, sports, lifestyle, and emotion domain scores compared with players who did not (*P < .05 for all).
Between the time of SLAP repair and the follow-up interview, 11.0% (8/73) of patients had undergone additional shoulder or elbow surgery on the same arm, including 4 revision labral tear repairs and 1 biceps tenodesis. Surgical revision was necessary in 6.8% (5/73) of isolated SLAP tear repairs. The 3 other surgeries were not directly related to the index SLAP repair (ie, ulnar collateral ligament reconstruction).
Discussion
As hypothesized, the RTP results identified by the current study were higher than those previously reported, with the exception of the study of Morgan et al, 23 which reported an 84% RTPP rate after SLAP repair. Of the 232 patients who underwent SLAP repair in the current study, 165 were operated on by the senior authors using the same technique, and 148 were baseball players who were at least 12 months out from surgery. Of this homogeneous group, an analysis of 73 study participants who underwent isolated SLAP repair revealed that overall, 83.6% of players perceived that they had achieved RTP (80.0% of pitchers and 91.3% of other position players). However, there was only a 60.3% RTPP rate, and significantly fewer pitchers perceived RTPP compared with other position players.
Morgan et al 23 reported that at 1 year after SLAP repair, 84% (37/44) of pitchers had successfully achieved RTPP, while 7 (16%) had decreased pitching velocity, control problems, shoulder stiffness, and pain. All 7 pitchers who did not successfully achieve RTPP had an undersurface rotator cuff tear that was debrided at the time of the index SLAP repair. They suggested that posterosuperior labral detachment from torsional “peel back” in these pitchers may have created secondary, progressive glenohumeral joint instability. From this suggestion, it can be more clearly understood how an untreated or poorly managed acute SLAP tear in the presence of repetitious, high overhead-throwing volume (loads, frequency) can progress to chronic rotator cuff injuries. 4,17 Progressively increasing glenohumeral joint instability shifts the primary throwing shoulder restraint from the more anatomically central labrum toward the more peripheral rotator cuff. High-volume loading of the long head of the biceps brachii tendon that occurs across the externally rotated and abducted glenohumeral joint of pitchers progressively peels the labrum away from the proximal humerus from the articular side outward. 4,9,17,25 In the presence of an incompetent superior labrum, these tensile loads transfer directly to the rotator cuff. 24,32
Levy et al 21 have shown that by ameliorating glenohumeral joint microinstability, SLAP repair significantly decreases rotator cuff tensile loads. Consideration of these glenohumeral joint pathomechanics led to the careful selection of participants in the current study to better identify the isolated effects of SLAP tear repair on perceived shoulder function and health. Therein lies the strength of the current study: the careful screening of patient records that led to the identification of a homogeneous cohort of baseball players that had been diagnosed solely with a primary, isolated SLAP tear. Compared with many previous studies, 15,16,23,27 the current study likely represents patients who were earlier in the SLAP tear progression before experiencing additional rotator cuff or labral injuries, as reported in the earlier report of Gilliam et al. 15
Although some previous studies have questioned the value of subjective assessments in overhead athletes, 3,12,16,26 we found that WOSI scores displayed significant relationships with patient perceptions of RTPP (Figure 3 and Table 4). The WOSI includes comprehensive questions related to postoperative symptoms most commonly reported by baseball players as being problematic after SLAP repair. These include shoulder or arm throbbing or aching, weakness, early fatigue, clicking or popping, motion loss, instability, concern for the shoulder getting worse, compensation by other muscles, difficulty in sleeping on the shoulder, and feeling the need to protect the shoulder or to avoid activities.
By a mean time point of 7.0 years after primary, isolated SLAP tear repair, pitchers more commonly perceived that they had not achieved RTPP compared with other position players. This important finding suggests that more frequent follow-ups may be needed among this unique and vulnerable position group to ensure that glenohumeral joint stiffness and pain have not returned after release to play. Also, the unique glenohumeral joint loading of repetitive overhead throwing may require an evolution of arthroscopic SLAP repair methods to the more frequent use of a less rigid fixation mode than is commonly used. As almost half of the pitchers in this study perceived unsuccessful RTPP because of excessive shoulder stiffness often associated with pain or weakness, more focused consideration should be given to a longer preoperative rehabilitation course in addition to an expanded evidence base for how surgical, rehabilitation, and conditioning management adequately prepares them to withstand high-volume loading needs while maintaining high performance levels over a long career. 13
Several study limitations exist. Surgical records were retrospectively reviewed for the surgical technique and the type and number of suture anchors used. In some instances, this information was not described as completely as desired. Additionally, as with any research study, potential bias needed to be controlled. 29 The meticulous patient identification methods that were used greatly helped control for selection and participation bias. Loss-to–follow-up bias may have occurred; however, the primary investigator attempted a variety of methods of reaching each potential study participant, and the 74.5% response rate represented a large proportion of the patient pool that qualified for study participation. Potential interviewer bias was controlled by strict adherence to the standardized survey questions and advance scripted additional questions related to shoulder symptoms before patient interviews. Given that patients were interviewed between 1.9 and 11.0 years after surgery, varying levels of recall bias likely existed. This may have been particularly true for professional baseball players, whose follow-up took place a mean of 2.1 years and 2.4 years later than collegiate and high school players, respectively. Last, these data represent solely subjective, perceived shoulder function and general health information. No objective or performance-based tests contributed to this report.
Conclusion
After the surgical repair of isolated type II or greater SLAP tears, other position players displayed superior RTP (91.3% vs 80.0%, respectively) and RTPP (78.3% vs 52.3%, respectively) rates compared with pitchers. Long-term follow-up suggests that pitchers may perceive greater long-term impairments and are less likely to return to their previous or higher performance level compared with other position players.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: L.D. has received educational support from Arthrex and Smith & Nephew, research support from DJO, and hospitality payments from Alpha Orthopedic Systems, Medacta, Medical Device Business Services (DePuy), and Stryker. F.C. has received educational support from Smith & Nephew and Zimmer Biomet, research support from DJO, and hospitality payments from Conformis and Zimmer Biomet. R.O. has received consulting fees from DePuy, speaking fees and an honorarium from Halyard Health, and hospitality payments from Arthrex and Halyard Health. J.A. has received speaking fees from Arthrex and Halyard Health. AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Baptist Health System Institutional Review Board.