
Abstract
Purpose:
We evaluated the clinical and radiological outcomes of arthroscopic repair of intratendinous partial-thickness rotator cuff tears.
Methods:
We retrospectively reviewed 30 patients who underwent arthroscopic repair of intratendinous partial-thickness rotator cuff tears from January 2010 to January 2015 in a single institute. Five outcome measures were used: a visual analog scale (VAS) pain score, the American Shoulder and Elbow Surgeons score, the shoulder rating scale of the University of California at Los Angeles, the Constant–Murley score, and range of motion (ROM). Pain was recorded using the VAS. Active ROM was measured goniometrically. Rotator cuff repair integrity was determined via magnetic resonance imaging or ultrasonography at least 6 months after arthroscopic repair.
Results:
Of the 30 patients, 29 (96.6%) returned for functional follow-up evaluation no earlier than 2 years after the operation. All functional scores exhibited significant improvements (all p = 0.000). The VAS improved from a mean of 5.8 ± 1.6 to 2.5 ± 2.6 (p = 0.000). The mean active ROM of forward flexion changed from 149.8 ± 33.8° preoperatively to 172.4 ± 9.1° (p = 0.001) at the last follow-up; abduction changed from 115.6 ± 50.3° to 171.3 ± 15.9° (p = 0.000). Postoperative radiological evaluation revealed retearing in three patients (3/28, 10.7%), including two with articular-side partial-thickness retears and one with a bursal-side partial-thickness retear.
Conclusion:
Arthroscopic repair of intratendinous partial-thickness rotator cuff tears was associated with a retearing rate of 10.7% on radiological follow-up and afforded significant clinical and functional improvements.
Introduction
Partial-thickness, rotator cuff tears are usually classified into three subtypes: bursal-side, intratendinous, and articular-side. 1,2 Several studies have reported the incidences of partial-thickness rotator cuff tears. 3 –7 Although intratendinous partial-thickness rotator cuff tears are clinically less common than other types of partial-thickness rotator cuff tears, the incidence was higher in cadaveric studies. 5 –7 No consensus on the incidence of intratendinous partial-thickness rotator cuff tears has emerged. However, intratendinous tears may be more common than previously recognized, because such tears are more difficult to diagnose than other tears given the absence of communication with the bursal or articular side of the cuff. 7,8
Although magnetic resonance imaging (MRI) is the optimal modality for diagnosis of rotator cuff tears, intratendinous tears remain more difficult to diagnose because they are concealed. 7,9,10 Only a few studies have described clinical and radiological outcomes after arthroscopic repair of intratendinous rotator cuff tears. 6,11,12
This study aimed to evaluate the clinical outcomes and tear repair integrity of patients treated arthroscopically using suture anchors to secure intratendinous partial-thickness rotator cuff tears. Our hypothesis was that the clinical outcomes of the patients with intratendinous partial-thickness rotator cuff tears would be improved after arthroscopic repair.
Materials and methods
Patient selection
We retrospectively reviewed patients who underwent arthroscopic repair of intratendinous partial-thickness rotator cuff tears from January 2010 to January 2015 in a single institute. One thousand seven hundred thirty-seven consecutive patients with rotator cuff tear were treated arthroscopically by the senior author. Among them, there were 37 patients with intratendinous partial-thickness rotator cuff tears who underwent arthroscopic rotator cuff repairs. All patients who visited the outpatient department with intratendinous partial-thickness tear were treated nonoperatively first, such as Non-steroidal anti-inflammatory drugs (NSAIDs), steroid injection, and physical therapy during minimum 6 months. Among them, patients without symptomatic improvement underwent operative treatment. We included tears limited to the tendinous areas on at least two oblique sagittal view sections on preoperative MRI (Figure 1), as confirmed arthroscopically (Figure 2). Patients with surgically verified partial-thickness rotator cuff tears, communicating with the subacromial bursa or glenohumeral joint, were excluded. In addition, we excluded patients: (1) with subscapularis tears requiring repair; (2) undergoing revision operations; and (3) with radiographically evident arthritic changes in the glenohumeral joint. Of the 37 initially included patients, 7 were excluded, 4 underwent subscapularis repair, 1 underwent a revision operation, and 2 had glenohumeral arthritis. Of the 30 included patients, 18 were male and 12 were female. The mean age at surgery was 51.8 years (range: 19–67 years). Other demographic data are listed in Table 1. This study was approved by the Institutional Review Board on Human Studies of the Ethical Committee of our hospital. The need for informed consent from all individual participants included in the study was waived (IRB no. CNUH 2019-01-032).
An intratendinous partial-thickness rotator cuff tear was revealed in the tendinous area on preoperative T2-weighted oblique sagittal magnetic resonance imaging.

Arthroscopic findings of the patient are evaluated in Figure 1. The intratendinous cuff tear did not communicate with
Demographic and surgical data.

Surgical technique
All operations were performed with patients in the beach-chair position under general anesthesia. Diagnostic arthroscopy was performed to assess rotator cuff and associated pathology. The cuff was examined carefully from both the articular and bursal sides. Subacromial decompression was performed in patients exhibiting arthroscopic evidence of subacromial impingement. Acromioplasty was limited to the removal of osteophytic bone. If the undersurface of the acromion lacked osteophytes, the inflamed bursal tissue was debrided, with minimal decortication of the undersurface and minimal release of the coracoacromial ligament.
Using a probe, we palpated the suspected area of rotator cuff on preoperative MRI using a probe to check puckering sign and then confirmed the intratendinous tear by the bubble sign. 13 –15 For 10 patients with rotator cuff tears, limited bursal-side debridement and resection of only the diseased portion of the tendon was performed, without conversion to full-thickness tears, and superficial avulsed flaps were then placed using the single-row technique (8 patients) or the in situ suture-bridge technique (2 patients). In four patients, limited articular-side debridement of only the diseased portion of the tendon was performed, without creating full-thickness tears, and tendon remnants were preserved using the transtendon technique (one patient) and the transtendon suture-bridge technique (three patients). 13,16 In 16 patients, the diseased portions of the tendon were debrided with the conversion of partial- into full-thickness tears (takedown-repair). The footprint of greater tuberosity was debrided of soft tissue to expose the cortical bone. We used Bio-Corkscrew suture anchors (4.5- or 5.5-mm-diameter depending on the tear size; Arthrex, Naples, Florida, USA) with eyelets, through which two no. 2 nonabsorbable braided sutures were threaded. The rotator cuff was repaired using the single-row technique (four patients), the double-row technique (two patients), the suture-bridge technique (nine patients) (Figure 3), 17 or side-to-side repair employing suture anchors (one patient).

Arthroscopic repair using the suture-bridge technique for the patient evaluated in Figure 1. A well-repaired rotator cuff tear is observed in both
Postoperative management
All patients received standardized pre- and perioperative care. The same treatment regimen was prescribed for all patients, regardless of the repair status of the articular-side rotator cuff. Postoperatively, we recommended the use of a shoulder-immobilizing sling with an abduction pillow and instructed all patients to maintain the shoulder at 30–40° of internal rotation and 20° of abduction. All patients performed gentle passive forward flexion (FF) arm exercises during the second postoperative week. The sling and abduction pillow was removed at 6 weeks postoperatively, and active mobilization commenced. Active, resistance-based muscle-strengthening exercises commenced at 12 weeks postoperatively using Thera-Band equipment (HCM-Hygenic Corp., Batu Gajah, Malaysia). At 3–4 months after surgery, patients were permitted to perform light activities, with participation in sports and heavy labor allowed after 6 months.
Clinical and radiological evaluation
Clinical data were collected by blinded orthopedic surgeons pre- and postoperatively at the final follow-up. MRI of the affected shoulder was performed preoperatively on all patients. Anteroposterior, supraspinatus outlet, axillary, and 30° caudal tilt views were obtained. We employed five outcome measures: a visual analog scale (VAS) pain score, the American Shoulder and Elbow Surgeons (ASES) score, 18 the Shoulder Rating Scale of the University of California at Los Angeles (UCLA), 19 the Constant–Murley score, 20 and range of motion (ROM). Pain was recorded using a VAS. Active ROM was measured goniometrically and passive ROM was not measured.
Rotator cuff integrity was explored via MRI evaluation at least 6 months after arthroscopic repair. We performed ultrasonography (US) on those who refused MRI due to the cost or claustrophobia. All MRI and US scans were evaluated by an experienced radiologist. A single musculoskeletal radiologist performed all follow-up US examinations using an IU-22 system (Philips Healthcare, Bothell, Washington, USA). A recurrent tendon defect was diagnosed when a distinct hypoechoic or mixed hyperechoic/hypoechoic defect was evident in both the transverse and longitudinal planes. A full-thickness retear was diagnosed if the rotator cuff exhibited a focal defect into which the deltoid muscle could be compressed with a probe (separating torn tendon ends), or if the cuff retracted to an extent, allowing torn ends to visualized. Tendon integrity was classified via MRI: (1) intact (sufficient thickness) or (2) insufficient/not healed/retorn (insufficient thickness was defined as a thickness less than half that of a normal cuff up to the discontinuity). 21
Statistical analyses
The paired t-test was used to compare pre- and postoperative values. SPSS software was used for all statistical analyses (ver. 12.0; SPSS Inc., Chicago, Illinois, USA); the α level was set to 0.05.
Results
Of the 30 patients, 29 (96.6%) returned for functional follow-up evaluation at a minimum of 2 years after the operation. The mean time from surgery to the final postoperative follow-up was 29.4 months (range: 24–55 months). The UCLA score improved from a mean of 21.2 ± 4.1 (range: 12–30) preoperatively to 31.1 ± 3.5 (range: 21–35) at the last follow-up. The ASES score improved from a mean of 39.8 ± 14.3 (range: 17–78) preoperatively to 72.8 ± 20.5 (range: 28–100) at the last follow-up. The Constant–Murley score improved from a mean of 57.2 ± 17.4 (range: 16–93) preoperatively to 76.0 ± 13.4 (range: 30–96) at the last follow-up. All functional scores indicated significant improvements in function and symptoms (all p = 0.000). The VAS improved from a mean of 5.8 ± 1.6 (range: 3–8) preoperatively to 2.5 ± 2.6 (range: 0–9; p = 0.000) postoperatively. The mean active FF ROM changed from 149.8 ± 33.8° (range: 50–180°) preoperatively to 172.4 ± 9.1° (range: 150–180°; p = 0.001) at the last follow-up; the extent of abduction changed from 115.6 ± 50.3° (range: 30–180°) to 171.3 ± 15.9° (range: 110–180°; p = 0.000). All functional scores, the pain score, and the ROM improved significantly after the operation (Table 2).
Preoperative findings and postoperative clinical outcomes.

VAS: visual analog scale; ASES: American Shoulder and Elbow Society score; UCLA: Shoulder Rating Scale of the University of California at Los Angeles score; Constant: Constant–Murley score; FF-ROM: forward flexion-range of motion; Abd-ROM: abduction range of motion.
aBased on separate paired t-test; p < 0.05 denotes statistical significance.
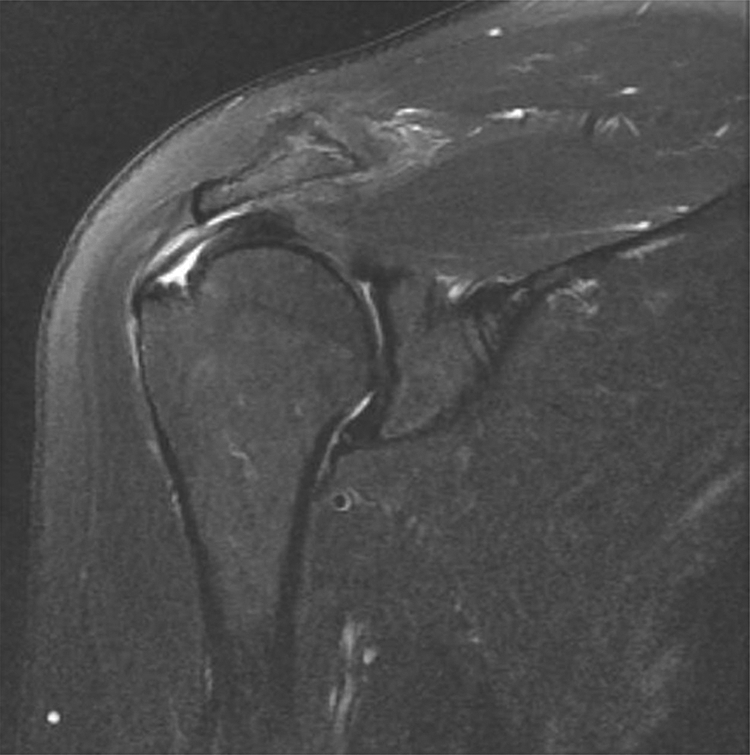
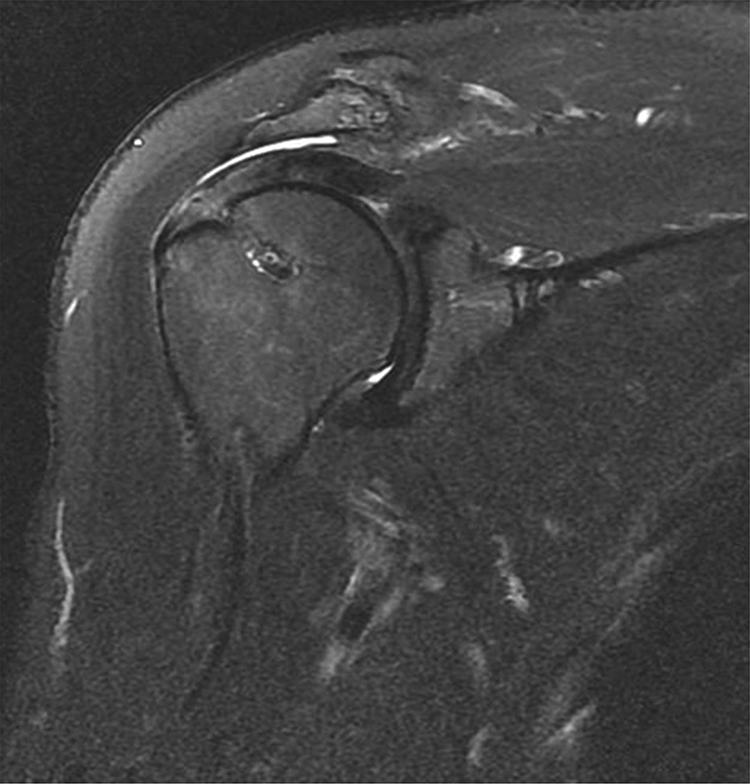
Of the 30 patients, 28 (93.3%) returned for follow-up radiological evaluation (Figures 4 and 5). Of these, 16 were evaluated via postoperative MRI and 12 via US. The mean radiological follow-up time was 11.1 months (range: 6–36 months). Retearing was evident in three patients (10.7%): two with articular-side partial-thickness retears and one with a bursal-side partial-thickness retear. Revision operations were successful. No nerve damage, deep infection, or anchor-related complication was noted.
The well-healed rotator cuff is observed in magnetic resonance imaging at 6 months after operation.

Bursal-side partial-thickness re-tearing is evident on postoperative magnetic resonance imaging after conversion to a full-thickness lesion followed by double-row repair.
Discussion
We report an 89.2% healing rate and good clinical outcomes of patients with intratendinous partial-thickness rotator cuff tears who had failed nonoperative treatment. Although many factors can affect clinical outcomes, the short-term clinical and radiological results were good after application of various arthroscopic repair techniques, performed according to the tear pattern and tendon quality.
Nineteen of thirty patients with the evidence of impingement underwent arthroscopic subacromial decompression. The procedure has been being debated up to the date. The arthroscopic subacromial decompression due to treating the only impingement would have no benefit compared with the nonoperative management program. 22 However, the subacromial decompression for patient underwent rotator cuff repair is the different issue. Advantages of subacromial decompression include resolution of impingement symptoms, improvement of arthroscopic visualization, and enhancement of healing potential by increasing the local concentration of growth and angiogenic factors released from the decompressed acromion. 23,24 In addition, in a recent randomized controlled trial, higher reoperation rate was found in the group underwent arthroscopic rotator cuff repair without acromioplasty than with acromioplasty although there was no difference in regards of functional and quality-of-life indices between both groups. 25 However, there are several cons regarding routine subacromial decompression including the American Academy of Orthopaedic Surgeons clinical practice guidelines, which does not recommend the procedure during rotator cuff repair. 26 –28 In our study, subacromial decompression was not performed routinely during the repair.
A cadaveric study on 249 supraspinatus tendons found that intratendinous partial-thickness rotator cuff tears were more common than bursal- or articular-side, or full-thickness, tears. 29 The clinical incidence of the former tear type ranges from 7.9% to 25.6%. 14,30 Thus, intratendinous partial-thickness rotator cuff tears may be more common than generally recognized. However, it remains challenging to diagnose and treat such tears effectively because, by definition, overt tendon disruption on either the bursal or articular surface of the rotator cuff is lacking. Definitive diagnosis requires recognition of a split in the tendon; the affected area may be soft or frayed, and may also exhibit edema, erosion, and/or redness. A positive “puckering sign,” or bulging of the supraspinatus tendon on shoulder elevation, is suggestive of an intratendinous, rotator cuff tear. 14,15 Lo and Burkhart et al. 13 described the bubble sign (a bulging expansion of the rotator cuff tendon following injection of saline into a suspect lesion during arthroscopic surgery); this is a useful indicator of an intratendinous tear of the rotator cuff.
Full- or partial-thickness rotator cuff tears have been extensively studied, but few data on intratendinous cuff tears are available because such tears are difficult to diagnose and treat. The need for treatment of intratendinous rotator cuff tears in patients who fail nonoperative treatment remains under-recognized. It may be that subacromial decompression alone affords favorable clinical results; intratendinous tears may heal spontaneously. However, in a longitudinal study, Yamaguchi et al. 31 found tear extensions on US in 39% of patients; the rotator cuff tendons did not heal. This work is important; rotator cuff tears do not heal spontaneously. It has long been known that rotator cuff tears retract to form adhesions, complicating surgical repair. The tendon deteriorates over time, often showing the consistency of tissue paper at the time of surgery. Fatty degeneration and muscle atrophy also develop and are probably permanent in cuff tears of long duration.
To the best of our knowledge, only a few studies have reported clinical outcomes after arthroscopic repair of intratendinous partial-thickness rotator cuff tears (Table 3). Park et al. 6 reported on outcomes and repair integrity after arthroscopic transtendon suture-bridge repair of intratendinous rotator cuff tears in 33 patients. At the final follow-up (minimally 2 years), the clinical outcomes were good and retearing attributable to inadequate cuff thickness (less than half that of a normal cuff up to the discontinuity; the Sugaya classification) developed in only two patients (6.1%). Xiao and Cui 11 reported that arthroscopic single-row repair (after limited bursal-side debridement and resection) of intratendinous tears in 33 consecutive patients improved the average UCLA and Constant scores at a minimum of 2 years of follow-up. Only 5 (8.15%) of 27 patients who underwent MRI to evaluate repair integrity exhibited partial retearing. Kim et al. 12 reported the outcomes of arthroscopic repair in 41 patients with intratendinous tears; all those who underwent arthroscopic single-row repair of full tears exhibited improved functional scores at a minimum of 2 years of follow-up. MRI performed at 9 months after surgery revealed no case with retearing.
Summary of studies evaluating outcomes after arthroscopic repair of transtendinous partial-thickness rotator cuff tears.

Here, all procedures were performed arthroscopically. We scheduled subacromial decompression only for patients showing subacromial impingement on arthroscopic examination (63.3%). We used the quality of the residual tendon and the extent of tearing to select either takedown-repair or remnant-preserving repair, plus a single- or double-row, or suture-bridge, technique.
Our study had certain limitations. First, because of the retrospective design, there was no control group against which to compare arthroscopic repair via an open rotator cuff repair procedure or conservative treatment. Second, although all US evaluations were performed by an experienced musculoskeletal radiologist, the technique is intrinsically examiner-dependent. However, US has been a valuable tool in evaluating the repaired rotator cuffs in patients with contraindications for MRI. 32 Moreover, recent studies found that US evaluations had similar diagnostic accuracies to MRI and both MRI and US are useful in the postoperative assessment of the repaired cuff. 33,34 Also, in some studies, surgeons interpreted office-based US data with high accuracy. 35,36 However, the surgeon did not examine the US data in this study, to avoid surgical bias. Third, we did not ask the radiologist to evaluate postoperative cuff integrity, which would have increased the reliability of the US data. Fourth, we included patients who underwent arthroscopic rotator cuff repair using two different techniques. However, we could not recruit the patients underwent arthroscopic rotator cuff repairs using homogenous technique because of various patterns and degrees of intratendinous tears. Nevertheless, the outcomes could not be affected by the techniques because recent systematic review reported that the repair technique (in situ repair versus repair after conversion to full-thickness tear) did not significantly affect the outcomes in partial-thickness rotator cuff tears. 37,38
Despite these limitations, our study had several strengths. First, all operations were performed by a single shoulder surgeon in one hospital, thereby reducing variability in postoperative outcomes. Second, we performed postoperative MRI or US to evaluate the integrity of the repaired rotator cuff. Third, although several surgical variables were not controlled because of the retrospective nature of the study, no patient underwent a concomitant or additional surgical procedure, such as distal clavicle resection, subscapularis repair, arthroscopic capsular release, or a revision operation necessitated by retearing; thereby reducing the variability in postoperative outcomes that might have been attributable to associated pathological conditions.
Conclusion
Arthroscopic repair of intratendinous partial-thickness rotator cuff tears was associated with a retearing rate of 10.7% on radiological follow-up and afforded significant clinical and functional improvements.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.