
Abstract
Background:
Baseball players are vulnerable to stress-related injuries due to the biomechanics required to perform successfully, and stress fractures can occur via overuse. Baseball players can also sustain traumatic fractures via collision. Rib fractures are among the most common injuries of the chest in professional baseball players, yet literature is lacking regarding the characteristics of these injuries and the subsequent missed time and effect on performance.
Purpose:
To evaluate in professional baseball players (1) the epidemiologic characteristics of rib fractures, (2) the differences between traumatic and stress rib fractures, (3) the effect of rib fracture on performance, and (4) the return-to-sport (RTS) time and rate after rib fracture.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The Major League Baseball Health and Injury Tracking System database was utilized to obtain fracture data between 2011 and 2022. The authors analyzed differences in stress and traumatic fractures across position groups and compared time missed and performance data for each fracture type.
Results:
A total of 121 fractures (54 stress, 57 traumatic, and 10 not specified) were identified: 42 MLB players and 79 Minor League Baseball players. The mean time missed for rib stress fractures was significantly higher at 98.13 ± 11.19 days compared with traumatic fractures (47.44 ± 6.23 days) (P < .001). Pitchers missed more time (99.93 ± 84.94 days) than infielders (42.83 ± 41.71 days) (P < .001). When assessing the effect of rib fractures on performance, position players had lower on-base percentage (P = .008) upon RTS as compared with before injury. In pitchers, a longer RTS time correlated with fewer innings pitched upon RTS .
Conclusion:
Professional baseball players who sustain rib stress fractures have a longer RTS time than those who sustain traumatic injuries. Athletes needed approximately 14 and 7 weeks to RTS after stress and traumatic fractures, respectively. Pitchers who sustained stress fractures had the longest RTS time at 17.6 weeks. Position players experienced significant decline in 1 out of 15 performance metrics indicating a minimal decline in performance upon return.
Rib fractures are among the most common injuries of the chest in the athlete, and there are several studies in the literature describing the incidence of rib fractures in multiple sports. Typically, athletes who play contact sports (American football, rugby)9,15,17 sustain traumatic, acute fractures while athletes who play noncontact sports (rowing, golf)12,14,18 sustain atraumatic, stress-related fractures. Traumatic fractures are typically caused by collisions and usually have acute pain in the thorax, notable popping or clicking, and in some instances, difficulty breathing or inability to return to play. The fracture fragments can be palpable in the chest wall.15,17 Stress fractures are typically related to overuse and can be caused by repeat excessive loading, leading to inflammatory changes and pathophysiologic bone remodeling. 19 Athletes who sustain stress fractures typically present insidiously with vague discomfort or tightness in the chest wall or shoulder that may only occur briefly during throwing or hitting. They can have tenderness over the chest wall, posterior thorax, or supraclavicular fossa.8,13,24 Because of the unclear presentation, rib stress fractures are often misdiagnosed as other shoulder/truncal injuries such as intercostal muscle strains, abdominal muscle strains, or rotator cuff impingement.8,24 In fact, in some cases, provocative testing for thoracic outlet syndrome can be positive in athletes who have rib stress fractures. 13 In both traumatic and stress injuries, initial radiographs can fail to identify fractures, and diagnosis is only made after advanced imaging (magnetic resonance imaging, computed tomography).8,13,17
Baseball itself is unique in that athletes can sustain both traumatic fractures via collision (hit by pitch, contact with other players or the boundary) or stress fractures via overuse. Overhead athletes, such as baseball pitchers, are susceptible to excessive loading due to the biomechanics required to perform successfully.3,7,9,23,24 Additionally, baseball players have been found to sustain rib fractures in several different locations, including the first rib and the lower posterior ribs, and while both pitching and batting.7,8,13,23,24
The Major League Baseball (MLB) Health and Injury Tracking System (HITS) database is a centralized MLB database that standardizes the tracking of player injuries across all professional baseball. 20 Conceived in 2010, all injuries and treatments are included and are linked to injury tracking codes. The database is an excellent resource for epidemiologic studies involving professional baseball injuries and has been utilized in several recent publications including but not limited to acromioclavicular joint injury, ulnar collateral ligament injury, forearm flexor injury, chest and abdominal muscle injury, hamstring strain, and general fractures.1,2,6,10,11,16,21,22,25 To date, there is no single study that details the epidemiology and performance following rib fractures in professional baseball.
The purpose of this study is to determine in professional baseball players (1) the epidemiologic characteristics of rib fractures, (2) the differences between traumatic and stress rib fractures, (3) the effect of rib fracture on performance, and (4) the return-to-sport (RTS) time and rate after rib fracture. We hypothesized that in professional baseball players, (1) both traumatic and stress fractures would be identified, (2) there would be more traumatic fractures than stress fractures sustained, (3) there would be no decline in performance level upon RTS, and (4) there would be full RTS after rib fracture with stress injuries requiring a longer time. These data will be utilized to counsel both professional and amateur baseball players who are both at risk for and who sustain rib injuries, especially regarding their postinjury ability to return to competition.
Methods
This study is a retrospective analysis of data contained in the MLB HITS database. After approval from the MLB research committee, deidentified HITS data from all MLB and Minor League Baseball (MiLB) thoracic rib fractures 2011 to 2022 were reviewed and included the following: diagnosis, month and year of injury, injury mechanism, body side and region of injury, event level of play, player age, position, throwing and batting hand, days missed due to the injury, and pre- and postinjury performance data. Data that were not available included imaging (radiographs, magnetic resonance imaging, computed tomography) and professional baseball service time. Dominant side was defined as an athlete’s throwing arm. Activity/injury mechanism and player position were analyzed to determine if specific athletes were at additional or less risk for injury. RTS was defined as the participation in ≥1 professional baseball game at the same level played in before injury; days missed was utilized as a surrogate for RTS. Performance after RTS was determined using pre- and postinjury performance metrics such as weighted runs created and wins above replacement. Innings pitched and plate appearances were used as surrogate measures for games per season.
Inclusion criteria for this study included any MLB or MiLB player who was diagnosed with a thoracic rib fracture. The players were separated by mechanism of fracture into stress, traumatic, or not-specified categories utilizing the column titled “Mechanism of Injury.” Stress fractures were identified using keywords “rotation/torsion,”“non-contact,” and “overuse gradual onset.” Traumatic fractures were categorized using keywords “fall/dive” and “contact with x” where x represented several values including “ground,”“ball,”“person,” or “boundary.” Duplicate entries were excluded from analysis.
Statistical Analysis
All continuous variables were assessed for normality using the Shapiro-Wilk test. Variables meeting normality assumptions were analyzed using parametric methods, including 1-way analysis of variance with Bonferroni-adjusted post hoc tests for comparisons across >2 groups, independent-samples t tests for comparisons between 2 groups, and paired-samples t tests for within-participant comparisons of pre- and postinjury performance metrics. For variables that violated normality assumptions (Shapiro-Wilk; P < .05), nonparametric methods were employed to confirm findings, including Mann-Whitney U tests for 2-group comparisons and generalized linear models with appropriate distribution and link functions for multigroup analyses, followed by Bonferroni post hoc assessments. Categorical variables, such as the frequency of rib injuries by batting or throwing laterality, were compared using chi-square tests, and associations between days missed and performance measures were evaluated using Spearman rank correlation for nonnormally distributed data. Statistical significance was set at P < .05 for all analyses.
Results
A total of 127 players were identified from 2011 to 2022. After applying the inclusion and exclusion criteria and removing duplicates and 1 outlier (based on days missed), a total of 121 players were included for analysis. The demographic information for all included players is displayed in Table 1, which also displays the demographic information for those players with performance statistics available ≥1 year preinjury and 1 year postinjury. The number of rib fractures sustained per year is displayed in Figure 1. There were no significant trends noted in rib fractures per year. The number of rib fractures sustained by month is displayed in Figure 2. Of the total 121 fractures, 114 (94%) occurred during baseball season (including spring training and the playoffs [March through October]).
Demographics of Professional Baseball Players With Thoracic Rib Fractures

Infield positions include catcher, first base, second base, third base, short stop, and infield.
Outfield positions include left field, center field, right field, and outfield.
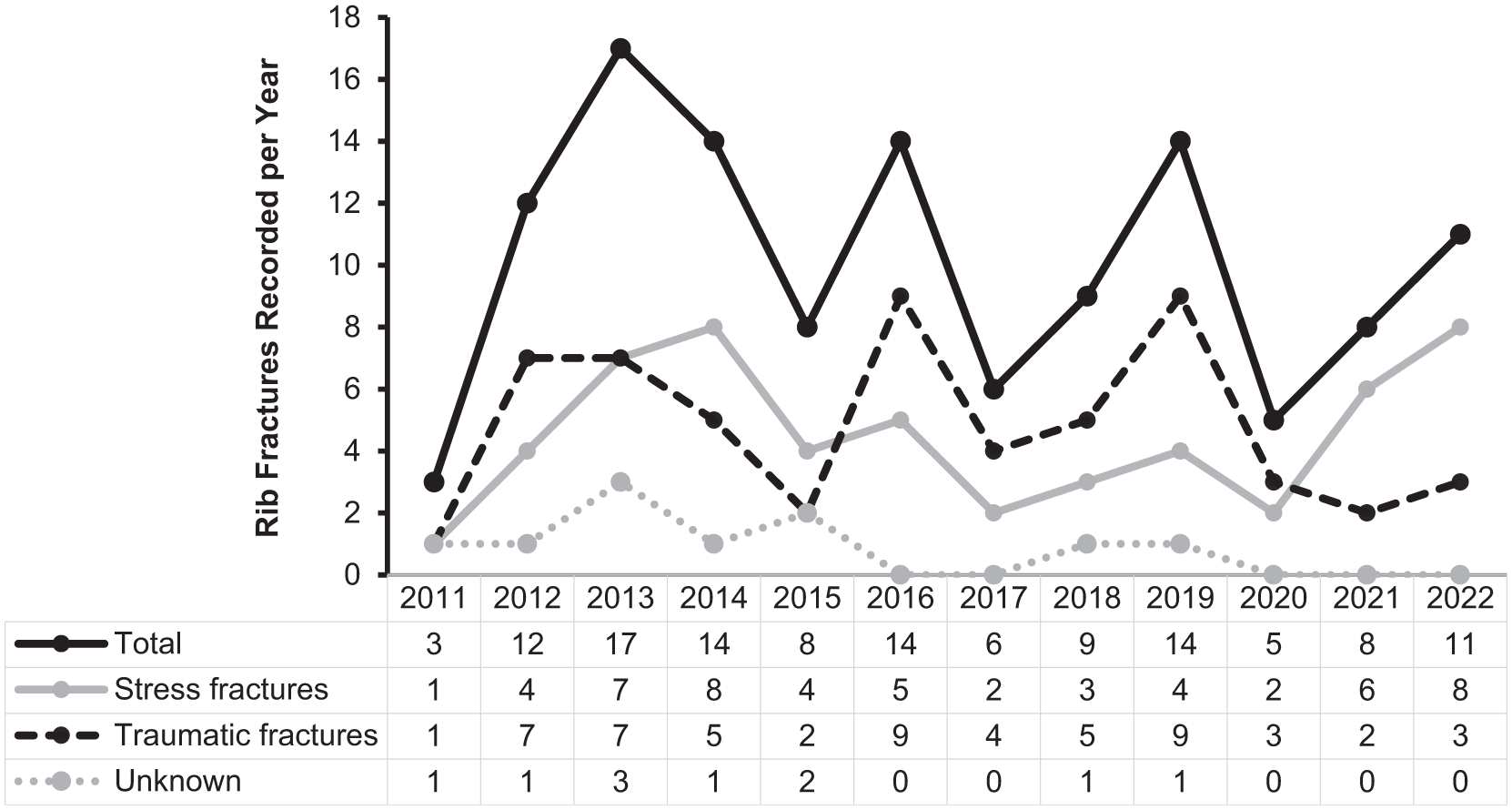
Number of rib fractures per year. Data are presented by year (2011-2022) for numbers of total, stress, traumatic, and nonspecified rib fracture injuries within Major League Baseball.

Number of rib fractures by month. Data are presented by month for numbers of total, stress, traumatic, and nonspecified rib fracture injuries within Major League Baseball.
Table 2 denotes the age and number of days missed for all professional baseball players, the professional baseball players with statistics pre- and postinjury, and MiLB and MLB professional baseball players. MiLB players (23.63 ± 3.96 years) were younger than MLB players (28.93 ± 3.54) (P < .001) and missed more time (83.66 ± 77.30 days) than MLB players (47.74 ± 47.75 days) (P = .002).
Age and Days Missed by Level of Play a
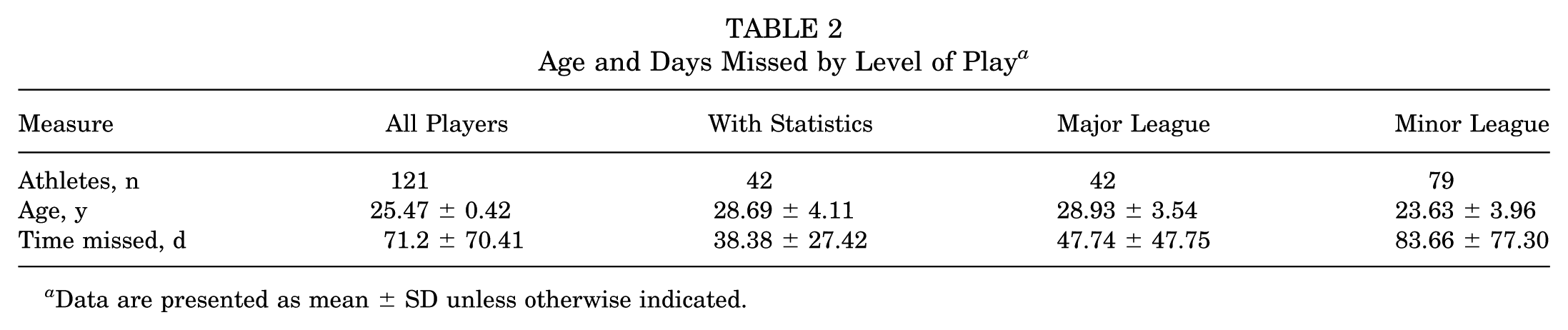
Data are presented as mean ± SD unless otherwise indicated.
The professional baseball players were then categorized by position. Table 3 displays a further breakdown of the athletes by position grouping, including age, days missed, and injury mechanism. All position groups were the same age and pitchers missed more time (99.93 ± 84.94 days) than infielders (42.83 ± 41.71 days) (P < .001). A chi-square analysis was conducted using positional groups and fracture type: pitchers who sustained rib fractures were more likely to sustain stress fractures (n = 28; 65.1%) than traumatic fractures (n = 9; 20.9%) (P < .001), and outfielders who sustained rib injuries were more likely to sustain traumatic fractures (n = 30; 69.8%) than stress fractures (n = 11; 25.6%) (P < .001).
Demographics Broken Down by Position a

1B, first base; 2B, second base; 3B, third base; C, catcher; CF, center field; IF, infield; LF, left field; OF, outfield; RF, right field; RP, relief pitcher; SP, starting pitcher; SS, short stop.
There was a significant difference in days missed between pitchers and IF (P < .001).
The P value of days missed between OF and IF was 0.418. The P value between OF and pitchers was 0.010.
Percentage of given injuries among specified position group.
Pitchers were more likely to sustain stress fractures (P < .001).
OF were more likely to sustain traumatic fractures (P < .001).
The professional baseball players were also stratified based on dominant arm. A player’s throwing arm was used as an analog for his dominant side. Table 4 displays this information, in addition to batting side for position players and injury mechanism for all-comers. It also lists the time missed based on dominant arm and injury mechanism. Pitchers who threw right-handed (n = 33; 76.7%) had a higher proportion of stress fractures (n = 21; 63.6%). Outfielders that were right-handed (n = 37; 86.0%) had a higher proportion of nondominant side injuries of any kind (n = 24; 64.9%). Although they were comparisons of interest, the current sample size was not statistically powered for further comparison of injury mechanisms within each side (right/left, dominant/nondominant).
Fracture Distribution by Arm Dominance and Player Position

Data are presented as n (%) or mean ± SD. Batting side not analyzed for pitchers.
Pitchers underwent an additional level of stratification, breaking down dominant arm into left- and right-handed throwing along with left- and right-sided injuries (Table 5). Pitchers who threw right-handed and had left-sided (nondominant) injuries had a higher proportion of stress injuries than traumatic injuries (72.2% vs 11.1%). The same stratification for position players is available in the Appendix Table.
Injury Location in Pitchers a

Data are presented as n (%). n (%) is based off of the column directly to the left.
In addition to time missed based on level of play (Table 2) and mechanism of injury combined with dominant arm (Table 4), overall time missed based on fracture type was measured and is displayed in Table 6. Professional baseball players who sustained stress fractures (98.13 days) missed more time than those that sustained traumatic fractures (47.44 days) (P < .001).
Days Missed by Fracture Type

There was a significant difference in days missed between stress fractures and traumatic fractures (P < .001).
Pitchers missed significantly more days after a stress fracture vs a traumatic fracture (P < .001).
The mechanism of injury for traumatic fractures was characterized and is broken down by position in Table 7. Infielders and pitchers had more fractures caused by contact with the ball (55.5% each), while outfielders sustained a higher proportion of fractures caused by contact with the boundary or the ground (60% total; 30% with each mechanism). In total, the largest number of traumatic fractures (n = 57) were caused by contact with the ball (n = 22; 38.6%), followed by contact with the ground (n = 14; 24.6%), with a person (n = 11; 19.3%), and with the boundary (n = 10; 17.5%).
Mechanism of Traumatic Fracture a

Data are presented as n (%).
There were 42 professional baseball players for whom performance statistics were obtained for ≥1 season before injury and 1 season after injury. Of these, 30 were position players and Table 8 displays the statistical measures of those players before and after sustaining rib fractures. Both traditional measures of performance (batting average, hits, home runs, etc) and newer, sabermetric driven measures of performance (batting average on balls in play, weighted runs created plus, weighted on-base average) were analyzed. Position players who had rib fractures had a lower on-base percentage (preinjury, 0.32 ± 0.04; postinjury, 0.30 ± 0.05) (P = .008). This significant decline in 1 out of 15 performance metrics indicates a minimal decline in performance upon return to competition.
Statistical Measures of Position Players Before and After Rib Fracture
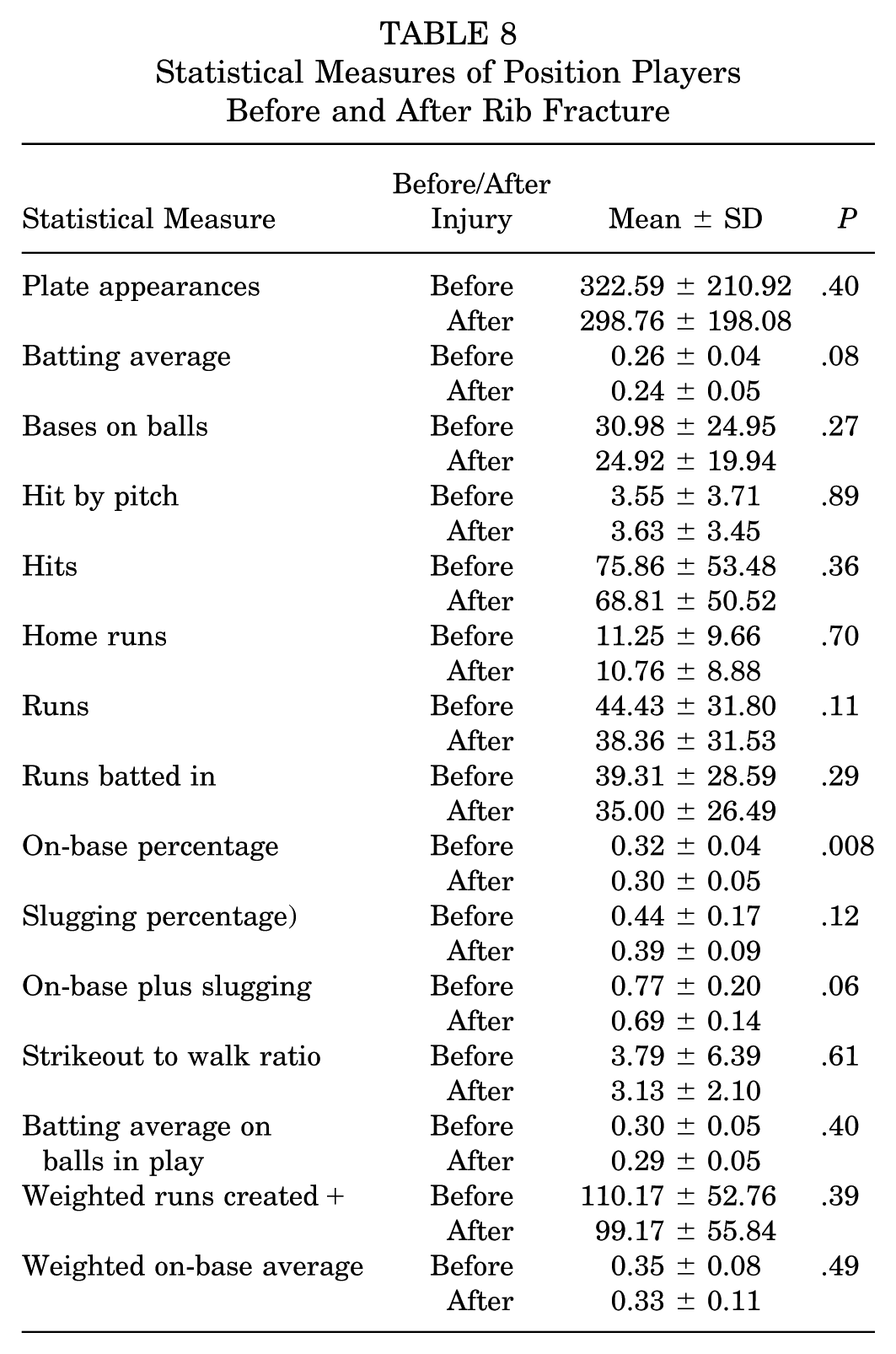
Table 9 displays the statistical measures of the 12 pitchers before and after rib fracture. Traditional measures of performance include earned run average and wins, while sabermetric measures include wins above replacement. There was a moderate negative correlation (R = −0.625; P= .03) observed between innings pitched and the number of days missed.
Statistical Measures of Pitchers Before and After Rib Fracture

Discussion
This study was able to answer the hypotheses as defined above. Utilizing the MLB HITS database, both traumatic and stress fractures were identified in professional baseball players who sustained rib injuries. There was no difference in the number of traumatic versus stress fractures sustained. There was a minimal decline in performance among positional players upon RTS with a lower on-base percentage after rib fracture. Nearly all (121 of 122) players returned to the sport within 1 year of injury.
A total of 121 rib fractures were identified during this 12-year period, of which there was a near-even split between traumatic (n = 57) and stress (n = 54) fractures; 10 were unspecified. Of these fractures, 42 were sustained at the major league level and 79 were sustained in the minors. Positionally, there was also a nearly equal distribution, with the infielder group experiencing 35 fractures and both pitchers and outfielders experiencing 43 fractures each. There were no significant trends based on year of injury, and most rib fractures occurred during the season. There were no traumatic fractures sustained in the offseason (November–February), which is understandable given the difference in intensity during the season versus the offseason.
Rib fractures led to a significant amount of time missed for athletes, with a mean of 71.2 ± 70.41 days missed. All 121 included players had a defined amount of time missed, which was also used as an analog for RTS. Players sustained injuries in all months of the year, including in the offseason, suggesting that “days missed” is the time it takes to return to participation in baseball activities. The 1 player that was excluded as an outlier missed a total of 1326 days and could have had other unknown circumstances leading to extended time away from baseball. The time missed was significantly different between MLB and MiLB players. This might be due to numerous potential factors that may merit additional study.
Baseball players who sustained rib stress fractures missed significantly more time than those who sustained traumatic injuries, and pitchers who sustained any rib fracture missed significantly more time than position players. Additionally, pitchers were more likely to sustain stress fractures than position players. There may be several reasons for these differences. Pitchers have a significantly higher volume of overhead throwing than their position player counterparts, leading to more stress on the kinetic chain.3,5 Further, symptoms are often vague and nonspecific, leading to difficulty in diagnosis of rib stress fracture; additionally, athletes often attempt to play through injury.7,8,24 Because stress fractures are caused by overuse, they require a prolonged recovery time with additional biomechanical modification to ensure that reinjury does not occur upon RTS. Comparatively, because traumatic injuries typically occur after an acute blow to the chest, athletes are generally allowed to RTS once pain is controlled and no mechanical changes are required. In one study, American football players were allowed to RTS once sufficient analgesia was obtained with anesthetic blocks and protective padding. 17 While there are no specific published guidelines for RTS in baseball players, case reports suggested that pitchers who sustained rib stress fracture are treated with a period of relative rest, pain management, and activity modification for 4 to 6 weeks until all pain has subsided followed by a graduated throwing program, with RTS by 8 to 10 weeks.8,24
Performance metrics were obtained for ≥1 full season before and after injury in 42 professional baseball players. Of the 30 position players, the only statistically significant finding was a decrease in on-base percentage. While these numbers suggest a slight decrease in production after injury, the small sample size affects the validity, and the other performance data suggest that position players who sustain rib fractures are able to return to their previous levels of play. In the even smaller sample of 12 pitchers, the only significant finding was a negative correlation between days missed and innings pitched. While the small sample size hinders the analysis, it stands to reason that if a pitcher misses more time due to an injury, he would be used by his team in a more limited role to limit the chance of aggravation or recurrence.
It is important to utilize the findings in this study to counsel baseball players in the context of thoracic injuries as a whole. The kinetic chain utilized for throwing places significant stress on the muscles of the abdomen (internal and external oblique, rectus and transversus abdominus) and chest (pectoralis major and minor, serratus anterior, internal and external intercostals), which can lead to muscular strains or tears.3,5,24 One proposed mechanism of rib stress fracture notes countering pull of the serratus anterior and external oblique on the affected rib, leading to microtrauma and eventually fracture. One must also consider the next link in the kinetic chain; 2 separate reviews of abdominal injury in baseball found that athletes missed between 20 and 30 days after sustaining an abdominal strain, which is less than half that of those who were found to have rib stress fractures in our analysis.1,4 This information is important to disseminate in the diagnosis of core injuries in baseball players.
Limitations
There are several limitations to our study. While the HITS database is a standardized tool with significant oversight, data are entered by multiple different sources such as athletic trainers and team physicians with inconsistency in reporting and accuracy. Each team could utilize different rehabilitation and RTS protocols, which can also limit consistency. Days missed was used as a surrogate for RTS, but each team could have a different definition for RTS, be it return to baseball activities, return to full practice, or return to game. It was also unclear whether the days missed for injuries at the end of the season were “in season” days missed or overall days missed, but this is mitigated by the fact that offseason injuries were included in the data set. While fractures were described as stress or traumatic, imaging findings were not provided. There could be differences in coding between different levels of medical training, leading to different or missed diagnoses of rib fracture. Because of this, it is unclear if every rib fracture was cataloged into the HITS database, and some rib fractures could have been missed in the data set. Missing data are more likely to be from the inaugural 2010 and 2011 seasons, when HITS was first implemented, as an internal audit revealed up to 18% of player records were missing ≥1 variable of data. 20 HITS does not specify the exact location of the rib fracture (eg, first vs fifth rib); therefore, trends in the data based on which rib was injured were not analyzed. The performance data are also limited because not every player had statistics available for their pre- and postinjury seasons, leading to a decrease in power of the statistical analysis. Being a retrospective analysis reliant on a central database, errors in data entry could be present. Additionally, the severity of injuries was unknown, and the complete context of injury was limited based on the data provided.
Conclusion
Rib fractures in professional baseball players represent a significant source of missed playing time, with stress fractures resulting in notably longer recovery periods than traumatic fractures. Athletes needed approximately 14 and 7 weeks to RTS after stress and traumatic fractures, respectively. This study demonstrates that pitchers, particularly those with stress-related injuries, are at heightened risk for prolonged absence (17.6 weeks) due to the biomechanical demands of overhead throwing. While nearly all athletes returned to sport in ≤1 year, position players experienced a minimal but statistically significant decline in 1 out of 15 recorded performance metrics (on-base percentage). Clinically, these findings emphasize the importance of accurate diagnosis and tailored rehabilitation strategies, especially for stress fractures, which may require biomechanical adjustments and extended recovery protocols. Understanding the epidemiology and effect of rib fractures can aid clinicians, trainers, and team personnel in optimizing return-to-play decisions and managing athlete expectations regarding performance outcomes after injury.
Footnotes
Appendix
Fracture Measures in Position Players Based on Throwing and Batting Arm

| Outfielders | |||||
|---|---|---|---|---|---|
| Throwing Arm | N (%) | Injured Side | N (%) | Injury Mechanism | N (%) |
| Right | 37 (76.7) | Right | 12 (32.4) | Stress | 5 (41.7) |
| Traumatic | 7 (58.3) | ||||
| Left | 24 (64.9) | Stress | 6 (25.0) | ||
| Traumatic | 16 (66.7) | ||||
| Not Specified | 2 (8.3) | ||||
| Not Specified | 1 (2.7) | Traumatic | 1 (100) | ||
| Left | 6 (23.3) | Right | 4 (66.7) | Traumatic | 6 (100) |
| Left | 2 (33.3) | ||||
| Batting Side | N (%) | Injured Side | N (%) | Injury Mechanism | N (%) |
| Right | 28 (65.1) | Right | 8 (28.6) | Stress | 5 (62.5) |
| Traumatic | 3 (37.5) | ||||
| Left | 19 (67.9) | Stress | 6 (31.6) | ||
| Traumatic | 11 (57.9) | ||||
| Not Specified | 2 (10.5) | ||||
| Not Specified | 1 (3.6) | Traumatic | 1 (100) | ||
| Left | 15 (34.9) | Right | 8 (53.3) | Traumatic | 15 (100) |
| Left | 7 (46.7) | ||||
| Infielders a | |||||
| Batting Side | N (%) | Injured Side | N (%) | Injury Mechanism | N (%) |
| Right | 25 (71.4) | Right | 12 (48.0) | Stress | 7 (58.3) |
| Traumatic | 4 (33.3) | ||||
| Not Specified | 1 (8.3) | ||||
| Left | 13 (52.0) | Stress | 3 (23.1) | ||
| Traumatic | 9 (69.2) | ||||
| Not Specified | 1 (7.7) | ||||
| Left | 6 (17.1) | Right | 2 (33.3) | Stress | 1 (50.0) |
| Trauma | 1 (50.0) | ||||
| Left | 4 (66.7) | Stress | 2 (50.0) | ||
| Trauma | 2 (50.0) | ||||
| Switch | 4 (11.4) | Right | 1 (25) | Stress | 1 (100) |
| Left | 3 (75) | Stress | 1 (33.3) | ||
| Traumatic | 2 (66.7) |
All infielders throw right-handed; only batting measures analyzed.
Acknowledgements
The authors acknowledge and thank the Office of the Commissioner of Major League Baseball, Dr. Gary Green, the Major League Baseball Players Union, and the Houston Astros organization for their support in this work. Similarly, they would like to thank the athletic trainers of Major and Minor League Baseball for their dedication to patient care and continual data collection and entry into the HITS database.
Final revision submitted September 29, 2025; accepted October 27, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.