
Abstract
Background:
Fractures are a significant cause of missed time in Major League Baseball (MLB) and Minor League Baseball (MiLB). MLB and the MLB Players Association recently instituted rule changes to limit collisions at home plate and second base.
Purpose:
To evaluate the epidemiologic characteristics of fractures in professional baseball and to assess the change in acute fracture incidence secondary to traumatic collisions at home plate and second base after the recently instituted rule changes.
Study Design:
Descriptive epidemiology study.
Methods:
The MLB Health and Injury Tracking System (HITS) database was used to access injury information on MLB and MiLB players to analyze fracture data from 2011 to 2017. Injuries were included if the primary diagnosis was classified as a fracture in the HITS system in its International Classification of Diseases, Ninth Revision, codes; injuries were excluded if they were not work related, if they occurred in the offseason, or if they were sustained by a nonplayer. The proportion of fractures occurring due to contact with the ground or another person in the relevant area of the field—home plate or second base—in the years before rule implementation was compared with the years after.
Results:
A total of 1798 fractures were identified: 342 among MLB players and 1456 among MiLB players. Mean time missed per fracture was 56.6 ± 48.4 days, with significantly less time missed in MLB (46.8 ± 47.7 days) compared with MiLB (59.0 ± 48.3 days) (P < .0001). A 1-way analysis of variance with post hoc Bonferroni correction demonstrated that starting pitchers missed significantly more time due to fractures per injury than all other position groups (P < .0001). Acute fractures due to contact with the ground or with another athlete were significantly decreased after rule implementation at home plate in 2014 (22 [3.0%] vs 14 [1.3%]; P = .015) and at second base in 2016 (90 [7.0%] vs 23 [4.5%]; P = .045).
Conclusion:
The recently instituted rule changes to reduce collisions between players at home plate and at second base are associated with reductions in the proportion of acute fractures in those areas on the field.
Keywords
Although baseball is not a contact sport with the same magnitude of impacts as those associated with football or hockey, fractures comprise a small but significant portion of the injuries experienced by baseball players. Data presented at the 2018 Major League Baseball (MLB) Winter Meetings indicated that 7% of the overall injury events and 4% of the overall days missed across MLB and Minor League Baseball (MiLB) were due to fractures (MLB staff, personal communication, 2018), and a recently published study reported that fractures represented 3% of MLB and MiLB injuries from 2011 to 2016. 7 Baseball players are especially at risk for traumatic fractures of the foot, hand, and face due to contact with a ball or bat. 13,16,24,26 Using the National Electronic Injury Surveillance System (NEISS), Carniol et al 8 reported that 27% of baseball-related face injuries involved fractures.
In addition to being at risk for these higher energy, traumatic fractures, baseball players are at increased risk for stress fractures. Olecranon stress fractures are well described in throwing athletes. 12 Although less common, there are reports of baseball players sustaining humeral stress fractures and ulnar shaft stress fractures from throwing, as well as rib stress fractures from batting. 15,19,27 Baseball players with prior surgery for biceps tendon abnormalities undergoing biceps tenodesis may also be at increased risk for humeral fractures, likely related to an increased stress riser from the associated tenodesis site or drill hole, especially with the torsional stresses that players apply when throwing. 10,18,21 A recent epidemiologic study of stress fractures in college athletes of all sports found that they were more prevalent in the preseason, 22% were recurrent injuries, and 21% were season ending. 23 Studies specific to fractures in baseball players have mostly focused on the upper extremity, including elbow stress fractures, shoulder fractures, and hook of hamate fractures. 3,4,13,25 Although these studies are available, to date there has not been a broad epidemiologic overview of all fractures across professional baseball.
In recent years, MLB and the MLB Players Association (MLBPA) have instituted rule changes to help make the game safer for players. A rule was instituted before the 2014 season prohibiting the catcher from blocking the pathway of the runner and the runner from purposely initiating contact with the catcher. 20 In 2016, a similar rule was instituted preventing runners sliding into second base from deliberately attempting to make contact with the fielder. It is unclear how these rule changes have affected acute fracture risk in professional baseball players. By understanding where and how fractures occur in baseball, researchers can identify evidence-informed high-risk areas and activities, and specific interventions may be developed to protect the health and safety of players.
The primary purpose of this study was to evaluate the epidemiologic patterns of fractures across MLB and MiLB. We aimed to investigate the impact of the instituted rule changes on acute fracture incidence. We hypothesized that the incidence of acute fractures due to traumatic collisions at home plate and second base would be lower in the years after the respective rule changes.
Methods
Database
We used the MLB Health and Injury Tracking System (HITS) database to access injury information regarding professional baseball players and fractures. Detailed information on HITS has been previously published. 22 HITS is a centralized MLB database that includes de-identified individual-level injury data entered by athletic trainers and, less frequently, team physicians into MLB’s league-wide electronic medical record, thus standardizing the tracking of player injuries across all of MLB. All players provide consent for inclusion in the medical record, and all injuries and treatments are included. The injury data are linked to physician notes, and diagnoses and injuries are tracked via codes from the International Classification of Diseases, Ninth Revision. 22 The database includes data from all 30 MLB clubs as well as the more than 200 MiLB teams across the United States. The HITS database has proven to be an excellent source for epidemiologic studies involving injuries in baseball, such as recent studies on abdominal oblique injuries, sliding injuries, elbow injuries, and hamstring strains. 1,5,6,9
Data Collection
Injuries were included if the primary diagnosis was classified as a fracture—both acute and overuse—and if the injury occurred between 2011 and 2017. Injuries were excluded if they were not work related, if they occurred in the offseason, or if the designated position was “umpire” or “base coach.” Avulsion fractures were included, and acute and chronic fractures were distinguished by a selection option in the database. For analysis of days missed, we excluded events with a final medical clearance date more than 1 baseball year: for example, an injury that occurred in spring training of one year that was not cleared until the regular season of the following year. In accordance with MLB policy, for days-missed analysis we excluded injuries whose medical clearance dates were in February, because these dates are sometimes not entered until spring training, and thus accurate time out of play cannot be verified in some cases.
We included all players at all positions across all leagues, regardless of whether the player incurred any days missed due to the injury. We included data from all portions of the season, including spring training, the regular season, and the postseason. We then queried for additional data including basic demographic data, body part injured, activity, mechanism of injury, player position, and days missed because of the injury.
Data Analysis
The data were aggregated, and frequencies for each individual occurrence of a fracture were stratified by body part, activity, injury mechanism, player position, acute versus overuse injuries, and whether surgery was required. Subgroup analyses were performed on wrist and hand injuries owing to the high frequency of these injuries in the population. Days missed, defined as the difference between the date of injury and the medical clearance date, were reported for each fracture type.
We then investigated the influence of the 2 rule changes of interest that were implemented. The prohibition on collisions at home plate was instituted for the 2014 season, whereas the rule against sliding into the fielder at second base was instituted for the 2016 season. We compared the overall proportion of acute or traumatic fractures occurring because of contact with the ground or another person in the relevant area of the field—home plate and second base, respectively—in the years before versus after institution of the rule (2011-2013 vs 2014-2017 for home plate; 2011-2015 vs 2016-2017 for second base).
All statistical analyses were performed with Stata 14.2 (StataCorp). Chi-square tests were used to compare differences in the proportion of fractures requiring surgery between leagues, differences in the proportion of fractures that were acute or traumatic between leagues, and differences in the proportion of fractures occurring before versus after the 2 rule changes. Wilcoxon signed-rank tests were used to compare days missed between the 2 leagues, owing to nonnormal distribution of this variable. One-way analysis of variance (ANOVA) tests were performed to compare days missed between multiple groups, with post hoc Bonferroni analysis conducted when indicated. Significance was defined as P < .05.
Results
General Fracture Epidemiology
A total of 1798 fractures were recorded between 2011 and 2017, with 342 in MLB players and 1456 in MiLB players (Table 1). Of these, 1552 fractures had a validated number of days missed and a medical clearance date within 1 baseball year of injury. The mean age of MLB players at the time of injury was 28.7 ± 4.1 years, compared with 22.7 ± 3.3 years in MiLB players (P < .0001). Mean time missed per fracture was significantly less in MLB players (46.8 ± 47.7 days) compared with MiLB players (59.0 ± 48.3 days) (P < .0001). Acute fractures comprised 90% of the total, and 30% of total observed fractures required surgical treatment. The overall number of fractures by year is demonstrated in Figure 1.
Major and Minor League Fracture Data Overview a

a MiLB, Minor League Baseball; MLB, Major League Baseball.
b Statistically significant difference between leagues (P < .05).

Total fractures in Major League Baseball and Minor League Baseball players by year. In each year, the majority of fractures occurred during regular season, followed by spring training and then postseason.
Fractures of the hand, finger, or thumb accounted for 32.5% of the overall fractures, followed by fractures of the wrist (17.5%) and fractures of the head or face (10.5%). Fractures to the neck, upper arm, and elbow accounted for the greatest numbers of days missed (Table 2). Figure 2 details the location on the field where the fractures occurred, with 46% occurring around home plate. The most common activity during which fractures were sustained was batting, comprising 44.0% of the overall fractures, with the most common mechanism of injury being contact with the ball, comprising 46.1% of the overall fractures (Tables 3 and 4).
Fractures by Body Part a
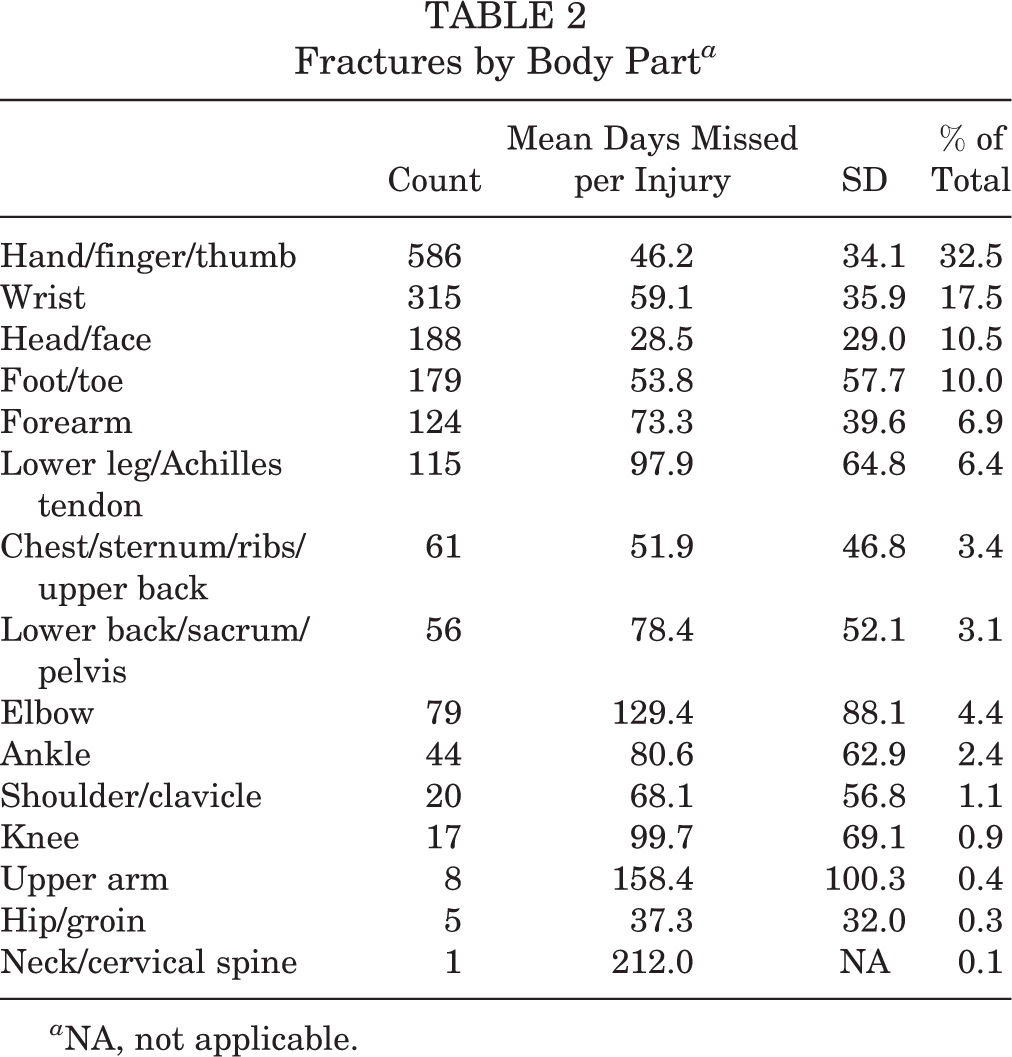
a NA, not applicable.
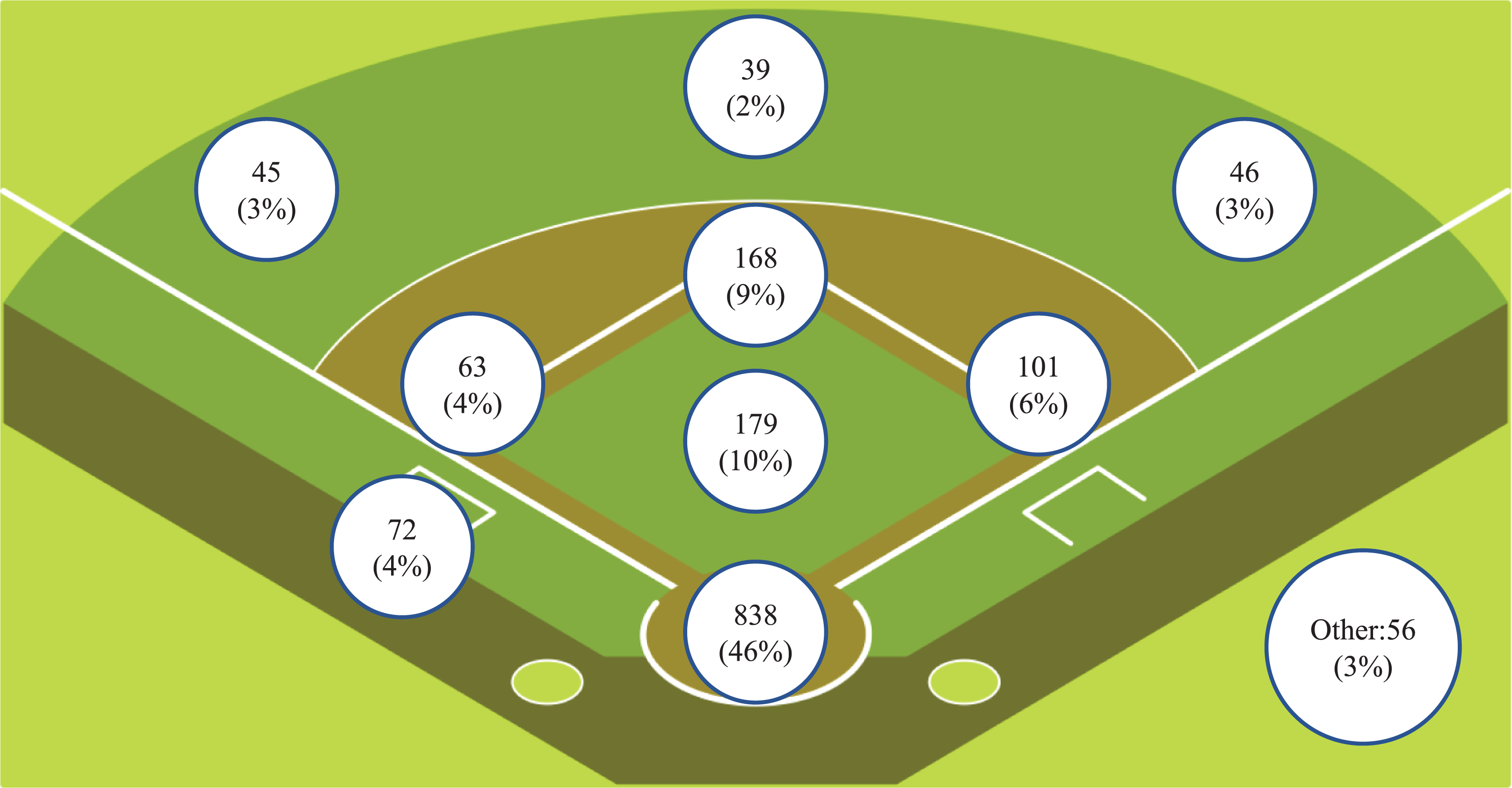
Fracture count based on location on the baseball field. The middle infield positions (second base and shortstop) are grouped together and represent 9% of fractures based on location.
Fractures by Activity

Fractures by Mechanism

Of the 791 fractures that occurred while batting, 516 (65%) occurred due to being hit by a pitch. The most common region injured while batting was the wrist with 268 fractures (34%), followed by the hand, finger, or thumb with 239 fractures (31%). Most of the wrist injuries sustained while batting were noncontact injuries (143 fractures, 53%), whereas the vast majority of hand/finger/thumb injuries were due to being hit by a pitch (224 fractures; 94%). Mean time missed for these wrist injuries was 58.2 ± 34.6 days, with surgery required in 70% of cases; for the hand/finger/thumb fractures, players missed a mean of 50.7 ± 31.2 days, with surgery required in 13% of cases.
Table 5 details fracture frequency and days missed by position per injury. Pitchers had the highest mean number of days missed, followed by outfielders. A 1-way ANOVA with post hoc Bonferroni correction showed differences among the position groups (F < .0001), with starting pitchers having significantly more missed time per injury than all other position groups (P < .0001).
Fractures by Position

Acute/Traumatic Fractures Related to Rule Changes
The overall proportion of acute fractures at home plate due to contact with the ground or another person was significantly decreased after the institution of the 2014 rule change regarding home plate collisions (3.0% vs 1.3%; P = .015) (Table 6). Similarly, the proportion of fractures at second base due to contact with the ground or another person was significantly decreased after implementation of the 2016 rule preventing sliding into fielders at second base (7.0% vs 4.5%; P = .045).
Impact of Rule Changes on Fractures Due to Contact With the Ground or Another Person

a A runner approaching home plate may not deviate from his path in order to initiate contact with the catcher, and the catcher may not block home plate.
b Statistically significant difference (P < .05).
c A runner approaching second base must make a bona fide attempt to slide into the base and not change his path to attempt to slide into the fielder.
Discussion
The present study examined the epidemiologic patterns of fractures in professional baseball players from 2011 to 2017. Fractures are a significant cause of time missed across professional baseball. Even in an ostensibly noncontact sport such as baseball, fractures to a variety of body regions occur each season. Fractures are injuries that result in a significant amount of missed time, with a mean of 56.6 ± 48.4 days, representing 2 months—nearly one-third of the season—due to these injuries.
There were 342 fractures in MLB compared with 1456 fractures in MiLB. Compared with MiLB players, MLB players were significantly older, returned to play faster, (46.8 vs 59.0 days; P < .0001), and required surgery less often (25% vs 32%; P = .0006). This discrepancy may suggest that treatment and return to play protocols differ between the major and minor leagues. However, the current analysis did not control for injury severity, which may drive some of these differences. Further investigation is required to thoroughly understand why these differences exist between the leagues.
Overall, players with fractures to the elbow, upper arm, and neck/cervical spine missed the most time before return to play. With respect to player position, starting pitchers missed significantly more time compared with other positions. Starting pitchers carry the burden of performing a repetitive throwing motion sometimes more than 100 times in a game and may repeat this stress on average every 5 days. Any fracture to a pitcher’s throwing arm will require additional caution to ensure that it is not reinjured once the player returns to pitching. The increased time missed among pitchers is also driven by elbow avulsion–type injuries and upper extremity stress fractures, which are not seen in other position players. 12,19 Although we did not have detailed prior surgical history from the database on the athletes included in the study, players who have undergone prior biceps tenodesis are known to be at higher risk for spiral humeral fractures from the increased stress riser postoperatively, which is compounded by the torsional stresses experienced by throwers. 10,18,21 Additionally, these throwing extremity fractures often require surgery and result in a protracted rehabilitation. 9
The most prevalent fractures seen in professional baseball were hand, finger, and thumb fractures (32.6%) and wrist fractures (17.5%), which together comprised almost half of all fractures evaluated. Wrist fractures (n = 268) and hand/finger/thumb fractures (n = 239) represented 65% of the overall fractures while batting. Whereas approximately 15% of these batting wrist injuries were due to being hit by a pitch, the majority were noncontact hook of hamate fractures, which are well-described in baseball and often require surgery. 3,13 In contrast, almost all of the fractures to the hand/finger/thumb that occurred while batting were due to being hit by a pitch. These specific injuries to the hand/finger/thumb may be decreased by future rule changes or equipment modifications, whereas noncontact injuries such as hook of the hamate fractures may be an innate risk with batting. Additional guards or padding on the dorsal hand or fingers may allow for a reduction in these hand/finger/thumb fractures. Although we were unable to assess the impact of protective gear on fracture incidence given the current data, this could be an interesting area for future research. For example, the effect of batting helmets modified with extensions to protect the face and jaw could be examined, as fractures to the head and face represented the third most common fracture area and were often the result of being hit by a pitch.
Encouragingly, the 2014 and 2016 rule changes designed to decrease injury risk for players involved in collisions at home plate and second base may have reduced acute fracture incidence in these areas. Carefully targeted rule changes may allow for mitigation of injury risk, as observed through our findings and others on the topics of injury prevention in various sports. Hanson et al 14 evaluated the effects of efforts to decrease concussions in professional football through a new rule in the National Football League that prevents players from leading with the crown of their helmet when making tackles. Those investigators found a reduction in concussions of more than 30% in defensive players, although they also found an increase in lower extremity injuries in offensive players. The institution of a 7-day injured list (formerly the disabled list) in professional baseball for players with concussions was designed in part to prevent concussion recurrence caused by returning to play too soon. 2 Restrictions on pitch counts have been instituted in a number of youth baseball leagues in order to prevent shoulder and elbow injuries. 11,17
In this study, we reviewed the effect of rule changes enacted by the MLB and MLBPA to decrease the likelihood of collisions between fielders and baserunners. We found that after the institution of these rules, there was a significant reduction in the number of acute fractures around home plate and second base occurring from contact with the ground or with a person. The overall proportion of acute/traumatic fractures at home plate areas decreased from 3.0% to 1.3% and the proportion of acute/traumatic fractures at second plate decreased from 7.0% to 4.5% after implementation of the associated rule. These results demonstrate the importance of injury surveillance after a rule change designed to reduce injuries to ensure that the rule has the desired effect on injury prevention.
Limitations
This study has several limitations. Although the HITS database is robust and is audited centrally, the data are entered by athletic trainers and, less frequently, physicians at the team level; therefore, differences with respect to documentation, rehabilitation protocols, and return-to-play policies among clubs may affect the consistency of the data across organizations. This study was a retrospective data analysis, and there may be flaws with in the actual data. The data only note diagnosis codes and may not accurately reflect injury severity. Furthermore, avulsion fractures were included, and these may be treated differently, with different associated time missed, compared with nonavulsion injuries of the same bone. Off-season injuries and non–work related injuries were also excluded, so the rates of fractures may be underestimated.
In addition, not all injuries were included in the days-missed analysis, such as those with medical clearance dates inconsistently entered or those with clearance date more than 1 baseball year. Coding inaccuracies could also exist in such a database. The data and diagnoses input by athletic trainers may differ from those that would be entered by sports medicine physicians and orthopaedic surgeons, although the diagnosis of fracture tends to be clear and there may be less change for miscoding. However, because the data are entered on an individual-level basis, coding inaccuracies may be less likely compared with aggregate data. In addition, because these data are collected for professional athletes, the results may not be generalizable to the broader population, who may not have access to the same elite orthopaedic surgeons, athletic trainers, and therapists. With respect to the analysis of the rule changes, only 2 years of data were available after the rule change at second base, which may affect the results. Finally, this study did not include an in-depth analysis of performance after return to play. Further research should focus on whether players are able to return to their preinjury level of performance after these fractures.
Conclusion
Fractures are a significant cause of time loss in professional baseball players. Detailed epidemiologic study may help guide areas of intervention and research to reduce fracture occurrence in these athletes. Interventions by MLB and the MLBPA to reduce collisions between players at home plate and at second base appear to be associated with reductions in the proportions of acute fractures in those areas due to traumatic collisions. Further interventions targeted at reducing fractures sustained to the hand area during batting may be effective given the high prevalence of fractures to the hand due to being hit by a pitch.
Footnotes
Final revision submitted March 8, 2020; accepted March 19, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study used data collected from the Major League Baseball (MLB) Injury Analytics Database, which is supported by the MLB. F.C. has a contract with MLB to provide MLB-related epidemiologic and biostatistical research support. B.T.F. has received consulting fees from Kaliber and hospitality payments from Zimmer Biomet. D.A.L. has received research support from Arthrex, educational support from Medwest and Smith & Nephew, and hospitality payments from Wright Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was waived for the present study.