
Abstract
Background:
Hip arthroscopy with a perineal post (ie, post assisted) may contribute to postoperative nerve and soft tissue complications. Postless hip arthroscopy has been increasingly used as an alternative to limit these postoperative nerve-related complications.
Purpose:
To compare the complication rates, such as pudendal nerve injury and perineal numbness, as well as any potentially reported clinical outcomes in patients undergoing postless versus perineal post-assisted hip arthroscopy.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
PubMed, MEDLINE, and Embase databases were searched until November 2024 according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, which yielded 2171 studies. Methodological quality was assessed using the methodological index for non-randomized studies (MINORS) criteria, and postoperative complications (ie, visual analog scale [VAS], modified Harris Hip Score, the Hip Outcome Score–Sports Specific Subscale), and outcomes were compiled in a meta-analysis where appropriate. Continuous outcomes were obtained using the mean difference (MD) while dichotomous outcomes were reported as odds ratios (ORs) that were calculated using the Cochran-Mantel-Haenzel method.
Results:
Five studies, from 4 patient cohorts, were included that comprised a total of 707 patients (60% female) with a frequency-weighted mean age of 29.9 years (range, 26.1-34 years). The mean MINORS score was 19.4 ± 1.1 (range, 18-21) with studies ranging from low to moderate quality. The pooled incidence of nerve or soft tissue injury from 2 studies was 48.1% (74/154 patients) for post-assisted and 31.3% (40/128 patients) for postless groups. Meta-analysis indicated a significantly lower incidence of nerve or soft tissue injury associated with postless hip arthroscopy (OR, 0.50; 95% CI, 0.31 to 0.82; P = .006). The pooled incidence of perineal numbness from 2 studies was 22.7% (35/154 patients) and 0.8% (1/128 patients) in the post-assisted and postless group, respectively. Meta-analysis demonstrated a significantly lower incidence of perineal numbness associated with postless hip arthroscopy (OR, 0.04; 95% CI, 0.01 to 0.21; P = .0002). Postless hip arthroscopy required lower traction time (MD, −6.15 minutes; 95% CI, −8.23 to −4.07 minutes; P = .00001) and holding traction force (MD, −12.12 kg; 95% CI, −15.32 to −8.93 kg; P = .00001) compared with post-assisted hip arthroscopy. Two studies reported VAS, with both studies indicating no significant difference between groups at either the postanesthesia care unit period or at 2 years’ follow-up.
Conclusion:
Our review showed that postless hip arthroscopy was associated with a significantly lower incidence of nerve or soft tissue injuries and perineal numbness, as well as reduced traction time and force, compared with the conventional post-assisted technique. However, the current paucity of comparative data in assessing complication rates and hip-related patient-reported outcome measures between post-assisted and postless hip arthroscopy techniques warrants further investigation.
The use of hip arthroscopy procedures has risen significantly over the past 2 decades,6,41 supported by growing evidence of improved patient-reported outcome (PRO) and lower rates of postoperative complications.8,26 A critical component of hip arthroscopy involves distraction of the hip joint, which is necessary to prevent intra-articular injuries and to provide sufficient working space for surgical instrumentation.23,30 Traditionally, this has been achieved with the use of a perineal post to apply countertraction during the procedure. 3
Despite the overall favorable safety profile of hip arthroscopy procedures, the use of a perineal post has been associated with complications. These include pudendal nerve injuries, which can result from compressive forces exerted on the pudendal nerve, and perineal soft tissue trauma, such as vaginal tears, skin necrosis, and vulvar hematoma. 24 The resultant pudendal nerve injury, which is one of the more serious complications, can manifest as external genital numbness and sexual dysfunction in men and women. 13 While pudendal nerve injuries typically resolve within a few weeks postoperatively, there is a risk of permanent nerve damage in certain cases that can result in urologic or sexual dysfunction. 24 A systematic review of hip arthroscopy complications from the past 26 years by Arriaza et al 1 reported that injuries caused by perineal compression accounted for 23% of all complications. Notably, perineal numbness have been reported to be as high as 42% in some studies.22,32 To mitigate these post-assisted risks, several postless hip arthroscopic techniques have been developed that leverage alternative patient positioning and support strategies. Some of these include placing the patient in the Trendelenburg using a specialized hip distraction table 24 or the Tutankhamun positions using a hip distractor (ArthroMX) or a hip fracture table (MAQUET Gmbh), 33 as well using support aids such as foam pads, yoga mats, and beanbags that can be performed with a standard fracture table.16,25,34 Kollmorgen et al 16 noted that existing hip distraction tables, including the Hana table (Smith & Nephew) distractor, ProFx table, and Arthrex distractor, can all be adapted to accommodate the Pink Pad technique. Results from initial studies have supported the benefits of postless techniques, including lower traction force required, minimal nerve damage, and fewer intraoperative changes in venous blood flow and tissue damage.17,24,31,39 However, postless techniques present unique challenges, including an increased risk of patient slippage at the foot or pelvis. 5 As awareness of these complications associated with post-assisted hip arthroscopy grows, the use of postless hip arthroscopic procedures has been increasing among surgeons seeking alternatives with fewer complications. 18
Until recently, data comparing post-assisted and postless hip arthroscopic procedures remained limited. Recent studies have sought to comparatively evaluate PROs, complication rates, and operative metrics among post-assisted and postless procedures.17,19 Findings from these studies suggest that postless procedures are associated with fewer complications and improved PROs compared with traditional post-assisted techniques. Despite the growing body of evidence, no systematic review or meta-analysis has been conducted to comprehensively compare these 2 approaches. Therefore, the purpose of this review is to synthesize the available evidence to evaluate the complications (eg, pudendal nerve injury and perineal numbness) as well as any potentially reported operative metrics and PROs associated with post-assisted and postless hip arthroscopy. We hypothesized that postless hip arthroscopy would be associated with fewer postoperative nerve complications when compared with post-assisted hip arthroscopy.
Methods
Search Strategy and Study Eligibility
This systematic review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. MEDLINE, Embase, and PubMed databases were electronically searched by 2 reviewers (P.A. and M.N.) from inception until November 2024. This search was conducted using the following keyword combinations and their synonyms as search terms: “post OR post-less OR post-less distraction” AND “hip arthroscopy.” The lead author cross-referenced relevant studies and previous review article reference lists, as well as searched Google Scholar to ensure a comprehensive search.
The inclusion criteria were (1) randomized controlled trials or comparative cohort studies assessing post-assisted versus postless hip arthroscopy; (2) studies that reported PROs, traction-related complications (ie, compression and distraction), or intraoperative outcome; and (3) studies published in English. The exclusion criteria were (1) case studies; (2) noncomparative clinical studies; (3) review articles or editorials; and (4) a lack of follow-up and/or comparative data in studies that reported complications or PROs.
Study Selection and Screening
After duplicate removal, the studies generated by the search were screened by 2 authors (P.A. and M.N.) in an independent manner during the title, abstract, and full-text stages. Any discrepancies at the title or abstract screening stage were carried forward to the full-text review to avoid premature exclusion. If no consensus was reached, a third senior author (J.C.) resolved any full-text disagreement. The kappa (κ) score was calculated to determine the level agreement between the 2 reviewers. Scores were categorized as perfect (1.00 > to κ≥ 0.81), substantial (0.80 > κ≥ 0.61), moderate (0.60 > κ≥ 0.41), fair (0.40 > κ≥ 0.21), slight (0.20 > κ≥ 0.01), or no agreement (κ = 0.00) between reviewers. 20
Methodological Assessment of Study Quality
Two authors (P.A. and M.N.) evaluated the methodological quality of the studies using the methodological index for non-randomized studies (MINORS) criteria. 36 This 12-item scale was designed to assess the risk of bias in nonrandomized comparative studies. An ideal global score of 24 signified high quality and a low risk of bias. Scores between >20 and <24 indicated moderate quality with a low risk of bias, while scores ≤20 denoted poor quality with a high risk of bias.
Data Abstraction
Data abstraction was carried out by 2 authors (P.A. and M.N.). Each author extracted data from half of the included studies and then crosschecked and verified the extracted data of their partner for accuracy. Data were abstracted into a standardized collection form using Microsoft Excel 2013 (Microsoft). Where possible, the following data were extracted from each included study: study information (author, design, level of evidence, publication year), patient demographic data (sample size, number of female patients, age, body mass index [BMI]), operative details (number of surgeons, operative and traction time, traction force, post-assisted and postless protocol), radiographic details (Tönnis grade, alpha angle, lateral center-edge angle [LCEA]), follow-up rate and duration, PROMs, and complication data. In our study, groin numbness reported as a complication in the included studies was categorized as perineal numbness.
Statistical Analysis
Descriptive statistics were used to analyze study characteristics and patient demographic data from all included studies. A meta-analysis was conducted on pooled data, and when pooling was not feasible, a qualitative synthesis was performed. For the continuous outcomes, the mean difference (MD) was obtained and calculated from the inverse variance method. For dichotomous outcomes, the odds ratio (OR) was calculated using the Cochran-Mantel-Haenzel method. Heterogeneity was assessed for all outcome variables using a standard χ2 test, and the calculation of an I2 statistic was used to quantify heterogeneity. 12 In the absence of significant heterogeneity (I2 < 50%), a fixed-effects model was performed. If significant heterogeneity was present (I2 > 50%), then the random-effects model was used to pool results. Confidence intervals (95% CI) were calculated and a P value of <.05 was deemed statistically significant for all outcome measures.
Results
Literature Search and Methodological Quality
Collectively, the systematic search yielded 2171 studies from all databases with 1361 studies remaining after duplicate removal (Figure 1). After title and abstract screening, 26 studies remained for full-text review, from which 21 studies were excluded mostly due to a lack of comparative data. The remaining 5 nonrandomized prospective or retrospective comparative cohort studies (1 level 2 evidence and 4 level 3 evidence) met the inclusion criteria and were incorporated into the study.17,19,28,31,35 It should be noted that although Kraeutler et al17,19 reported on patients from the same cohort and institution, each study offered distinct and nonoverlapping data. For instance, Kraeutler et al 17 detailed early postoperative complications in the full cohort, whereas Kraeutler 19 reported long-term PROs in a follow-up study from a subset of 69 out of the original 87 patients. The inclusion of both studies allows for a more holistic understanding of short- and long-term outcomes without duplicating data in our analysis. The interrater level of agreement between reviewers was considered near perfect (κ = 0.84) for the title and abstract screening as well as for the full-text screening (κ = 0.89).

Systematic search results using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Based on the MINORS criteria, the mean methodological quality score of included studies was 19.4 ± 1.1 (range, 18-21) (Table 1). Two studies17,19 were deemed to be moderate quality (low risk of bias), while 3 studies28,31,35 were poor quality (high risk of bias). Most studies did not specify a prospective study size calculation or an unbiased assessment (ie, blinding of assessors) of the study endpoints, which may have been difficult with the potential surgical intervention.
Quality Assessment of Nonrandomized Studies Using MINORS Criteria a

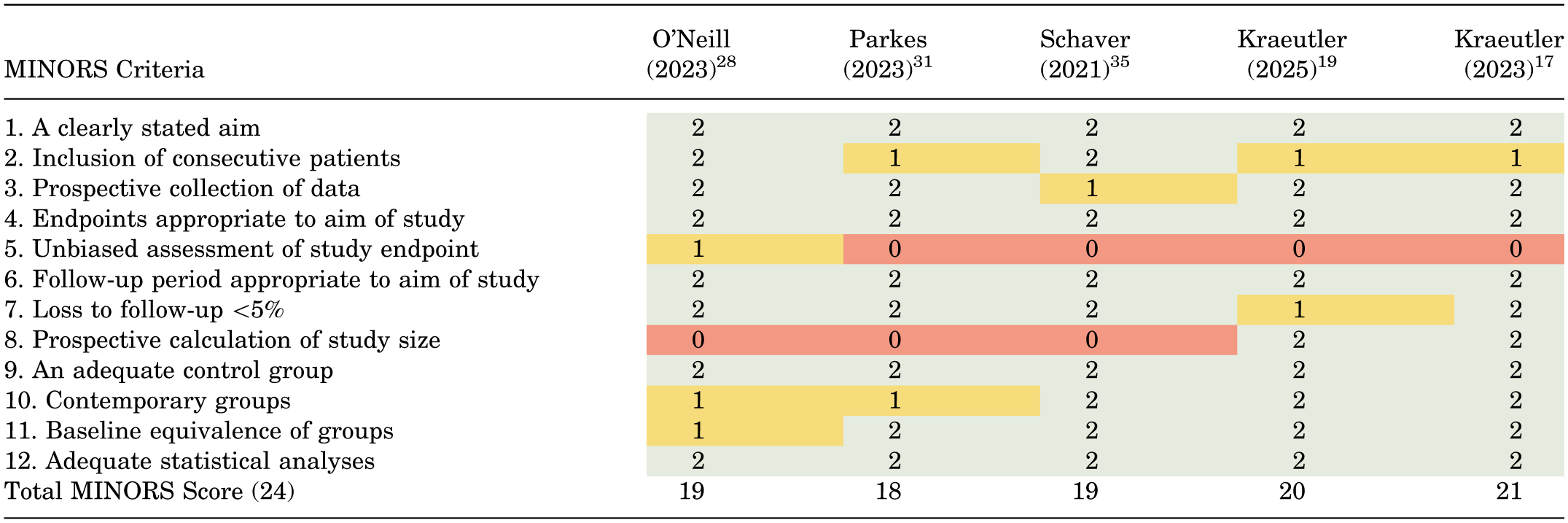
MINORS, methodological index for non-randomized studies. Scoring: 0 (not reported; red), 1 (reported but inadequate; yellow), or 2 (adequate; green).
Study Characteristics
From the 5 studies, a total of 707 patients (frequency-weighted mean age, 29.9 years [range, 26.1-34.0 years]; 60% female) were included (Table 2). Of these patients, 307 (frequency-weighted mean age, 28.6 years [range, 26.9-30.29 years]; 63% female) were in the postless group and 400 (frequency-weighted mean age, 30.8 years [range, 26.1-34.0 years]; 57% female) were in the post-assisted group. The frequency-weighted mean BMI was 25.1 kg/m2 and 25.3 kg/m2 for the postless and post-assisted groups, respectively. Three studies reported the preoperative alpha angle (postless, 65.9° [range, 65.1°-67.1°]; post-assisted, 64° [range, 61°-67.1°]) and LCEA (postless, 29° [range, 27.9°-30.9°]; post-assisted, 28.9° [range, 27.6°-31.1°]).19,28,31 One study 19 provided the Tönnis angle (postless, 6 ± 1.9; post-assisted, 6.5 ± 2.4). One study 31 reported a preoperative Tönnis grade (postless, 0.13 ± 0.34; post-assisted, 0.07 ± 0.26). Four studies18,19,31,35 (545/569 patients; 96%) reported follow-up rates of 21 days to 24.4 months.
Baseline Characteristics of Included Studies a

Data are presented as mean ± SD. Dashes in table cells indicate data not reported. BMI, body mass index; HOS-SSS, Hip Outcome Score–Sports Specific Subscale; LCEA, lateral center-edge angle; mo, month; mHHS, modified Harris Hip Score; PA, post-assisted; PL, postless; SANE, Single Assessment Numeric Evaluation; UCLA, University of California, Los Angeles; VAS, visual analog scale; wk, week.
Postless Technique and Operative Details
All studies specified that surgical procedures were performed by a single surgeon. Two studies17,19 reported labral repair (postless, 64.5% [40/62 procedures]; post-assisted, 77.7% [73/94 procedures]) and reconstruction (postless, 29% [18/62 procedures]; post-assisted, 22.3% [21/94 procedures]) procedures. Two studies17,35 reported the bed Trendelenburg angle, which ranged from 5° to 10° (Table 3). In all studies, the post-assisted procedures were performed using the Hip Distractor system (Smith & Nephew), also known as the Hip Positioning system. Three studies briefly provided further details on the post-assisted procedures. Two studies used a large, padded perineal post and a well-padded boot and positioned the operative extremity in 30° of abduction.17,19 The third study placed the perineal post in the pelvic rest opening, used well-padded boots, and positioned the contralateral limb in approximately 40° of abduction. 35 With regard to postless technique, 3 studies28,31,35 used the Pink Hip Kit (Smith & Nephew) while 2 studies17,19 used the Pivot Guardian (Stryker). Three studies17,31,35 reported traction time, from which the mean traction time was 46.6 minutes (range, 40.9-55.0 minutes) and 53.3 minutes (range, 45.8-63.0 minutes) for the postless and post-assisted groups, respectively. Traction force was reported by 2 studies28,31 as maximal and holding traction force. The mean maximal and holding traction force was 70.4 kg (range, 69.9-70.8 kg) and 55.8 kg (range, 55.8-55.9 kg) for the postless group and 96.1 kg (range, 96.0-96.3 kg) and 67.9 kg (range, 67.5-68.3 kg) for the post-assisted group, respectively. Meta-analysis indicated that postless hip arthroscopy required lower traction time (MD, −6.15 minutes; 95% CI, −8.23 to −4.07 minutes; P = .00001; I2 = 0%; Figure 2A), holding traction force (MD, −12.12 kg; 95% CI, −15.32 to −8.93 kg; P = .00001; I2 = 0%; Figure 2B), and maximal traction force (MD, −25.75 kg; 95% CI, −29.06 to −22.44 kg; P = .00001; I2 = 0%; Figure 2C) in comparison with post-assisted hip arthroscopy.
Post and Postless Operative Technique Used by Included Studies a

Data are presented as mean ± SD unless otherwise indicated. Dashes in table cells indicate data not reported.

Forest plots illustrating results of the pooled analysis for post (ie, post-assisted) versus postless hip arthroscopy for (A) traction time, (B) holding traction force, and (C) maximal traction force. IV, inverse variance.
Pain Outcomes
Pain levels were reported by 2 studies19,35 using either the visual analog scale (VAS) or self-reporting. One study recorded VAS scores during the postanesthesia care unit period, 35 while the other study collected VAS scores at approximately 2 years (21.3-24.4 months). 19 Kraeutler et al 19 also showed a trend toward significance with a higher proportion of patients in the postless group achieving a substantial clinical benefit (SCB) for the VAS score at roughly the 2-year follow-up (postless, 55.6%; post-assisted, 34.1%; P = .08). At the same follow-up period, no significant differences were observed in the proportion of patients between the 2 groups who achieved the VAS minimal clinically important difference (MCID) (postless, 82.6%; post-assisted, 66.7%; P = .18) or Patient Acceptable Symptom State (PASS) thresholds (postless, 74.1%; post-assisted, 56.1%; P = .13) for the VAS score. Schaver et al 35 further assessed the number of patients who reported postoperative pain using the VAS at the first follow-up visit (range, 21.0-23.2 days) and showed that a significantly higher proportion of patients in the postless group experienced pain compared with the post-assisted group (postless, 66.7%; post-assisted, 49%; P = .01). However, after adjusting for age, sex, BMI, and smoking status, no significant differences were found in the VAS pain scores between groups in the postanesthesia care unit (P = .35). Additionally, there was no statistically significant difference in the total mean morphine milligram equivalents consumed between the 2 groups (postless, 60.6 ± 15.5; post-assisted, 63.9 ± 18.3; P = .16).
Function- and Activity-Related Outcomes
One study 19 reported function and activity outcomes, including the University of California, Los Angeles (UCLA), Activity Scale, modified Harris Hip Score (mHHS), the Hip Outcome Score–Sports Specific Subscale (HOS-SSS), and the Single Assessment Numeric Evaluation. Among all the measures, the postless group had significantly higher scores at the 2-year follow-up for both the mHHS (postless, 82.2 ± 12.2; post-assisted, 73.7 ± 16.7; P = .03) and the UCLA Activity Scale (postless, 8.4 ± 2.1; post-assisted, 7.0 ± 2.5; P = .02). No other significant differences in PROMs existed between groups. When comparing the 2 groups in terms of SCB, PASS, or MCID, a significantly higher proportion of patients in the postless group achieved an SCB on the HOS-SSS score (postless, 72%; post-assisted, 41.5%; P = .02) and a PASS for the UCLA Activity Scale (postless, 89.3%; post-assisted, 68.3%; P = .04), mHHS (postless, 84.6%; post-assisted, 61%; P = .04), and HOS-SSS scores (postless, 84%; post-assisted, 61%; P = .048).
Nerve or Soft Tissue Injury and Complications
Three of the 5 studies17,31,35 reported on the incidence of any nerve or soft tissue injury. Of these, 1 study 35 subjectively documented any complications from surgery and stated that neither group experienced any nerve or soft tissue injuries. From the remaining 2 studies, 1 study 17 administered a 16-question survey inquiring about postsurgical regional numbness while the other study 31 embedded clinical questions into the electronic medical record regarding postsurgical nerve symptoms and location. From these 2 studies, the pooled incidence of nerve or soft tissue injuries was 48% (74/154) and 31% (40/128) for the post-assisted and postless groups, respectively. The meta-analysis indicated a significantly lower incidence of nerve or soft tissue injury associated with postless hip arthroscopy at follow-ups ranging from 3 to 6 months (2 studies [282 patients]; OR, 0.50; 95% CI, 0.31-0.82; P = .006; I2 = 0%; Figure 3A). One study 17 reported a higher incidence of sexual dysfunction (post-assisted, 5.6% [3/53]; postless, 0% [0/34]) and urinary dysfunction (post-assisted, 3.8% [2/53]; postless, 2.9% [1/34]) after post-assisted hip arthroscopy. However, these differences were not statistically significant when compared with postless hip arthroscopy. In the post-assisted group, the mean duration of sexual and urinary dysfunction was 7 ± 3 days and 6 ± 6 days, respectively, while in the postless group, urinary dysfunction in the single affected patient lasted 7 days.
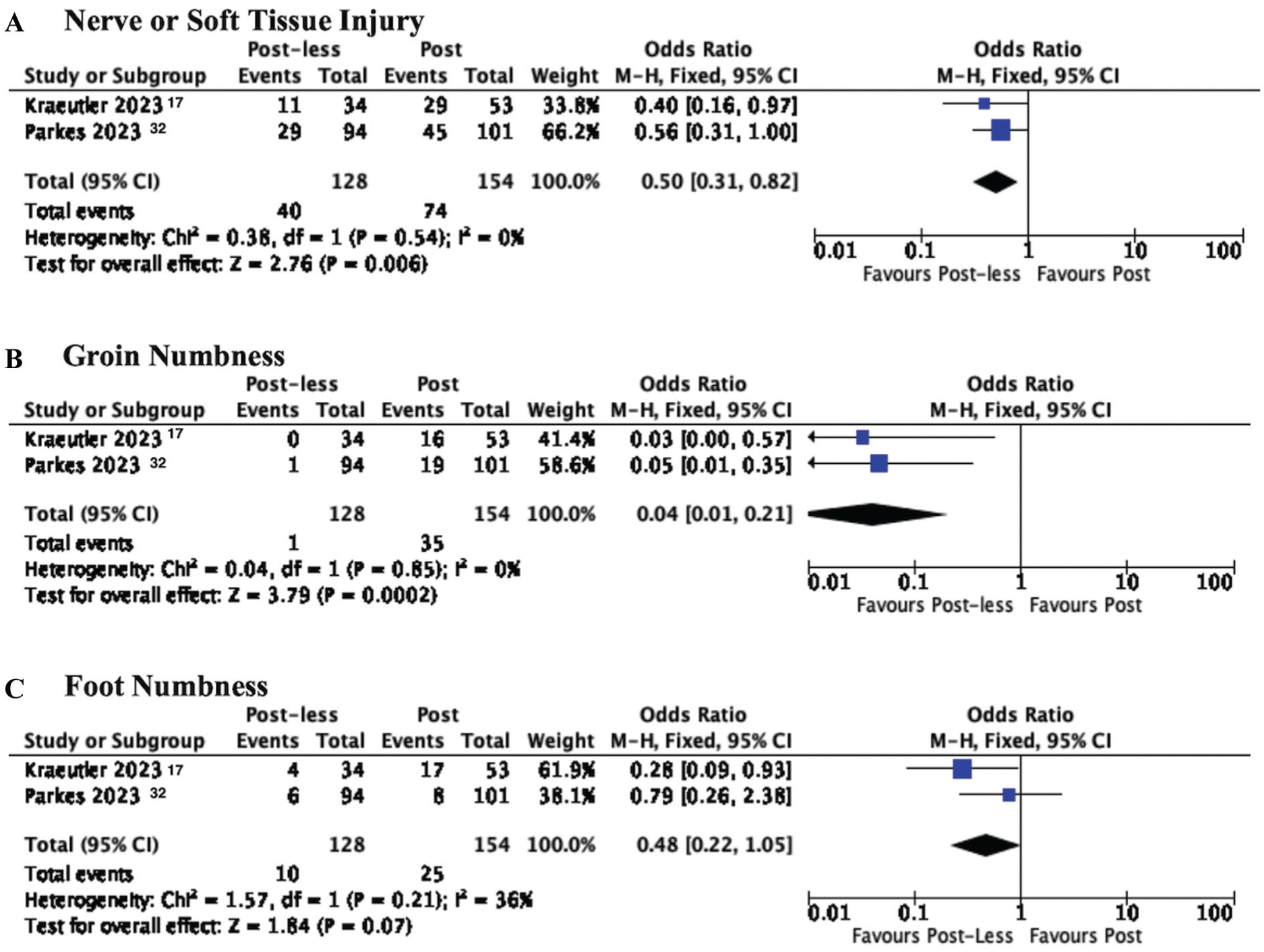
Forest plots illustrating results of the pooled analysis for post (ie, post-assisted) versus postless hip arthroscopy for (A) nerve injury/complications, (B) perineal numbness, and (C) foot numbness. M-H, Mantel-Haenszel.
Perineal and foot numbness were explicitly reported by 2 studies17,31 The pooled incidence of perineal numbness in these 2 studies was 0.8% (1/128) in the postless group and 22.7% (35/154) for the post-assisted group. The meta-analysis demonstrated a significant lower incidence of perineal numbness associated with postless hip arthroscopy at the 3- to 6-month follow-up period (2 studies [282 patients]; OR, 0.04; 95% CI, 0.01-0.21; P = .0002; I2 = 0%; Figure 3B). Perineal numbness lasted for a mean duration of 5 ± 3 days in the post-assisted group in 1 study 17 while another study 31 reported a mean duration of 75 ± 40 days until complete resolution in both groups.
At the same follow-up periods, the pooled incidence of foot numbness was 7.8% (10/128) for the postless group and 16.2% (25/154) for the post-assisted group. The meta-analysis indicated a trend toward significance favoring a lower incidence of foot numbness in the postless group (2 studies [282 patients]; OR, 0.48; 95% CI, 0.22-1.05; P = .07; I2 = 36%; Figure 3C). The mean duration of foot numbness was significantly longer in the post-assisted group compared with the postless group (postless, 2 ± 1 days; post-assisted, 15 ± 37 days; P = .04). Parkes et al 31 also noted no significant difference in the occurrence of regional numbness of the lateral thigh (postless, 21.2% [20/94]; post-assisted, 18.8% [19/101]; P = .83) or medial thigh (postless, 0% [0/94]; post-assisted, 4% [4/101]; P = .15) between the 2 groups.
Discussion
When comparing postless and conventional post-assisted hip arthroscopy, the major findings from this study demonstrated a significantly lower incidence of nerve and soft tissue injuries (P = .006) and perineal numbness (P = .0002), as well as less traction time and force (P = .00001) among patients undergoing postless hip arthroscopy. With regard to foot numbness, there was a lower incidence among postless hip arthroscopy procedures (7.8% vs 16.2%), however, this was not statistically significant (P = .07). There were no significant differences in postoperative pain levels between postless and post-assisted hip arthroscopy.
Although hip arthroscopy is a relatively safe procedure, the complication rates of post-assisted hip arthroscopies range from 1.8% to 46%, which encompass genitourinary/sexual dysfunction, perineal pain and numbness, perineal skin tears, and soft tissue injuries.7,11,15 However, due to study designs’ administering unvalidated measures coupled with the delicate and sensitive nature of these injuries, the incidence and severity of post-assisted injuries are likely underestimated. One review found post-related complications were reported at a rate 5 times higher in prospective versus retrospective studies. 40 From a study using online anonymous patient responses after post-assisted hip arthroscopy, 22% (5/23) of patients experienced permanent sexual dysfunction and only roughly 9% (2/23) were informed preoperatively of potential perineal-related complications. 13 While these complications often resolve over time, proactive measures to prevent such injuries and preoperative patient education about these complications are crucial for improving the overall patient experience. Postless hip arthroscopy may be associated with an increased risk of foot or pelvic slippage, a complication typically mitigated by the countertraction provided by a perineal post. In a survey of surgeons, 12% reported reverting back to using a perineal post, primarily because of insufficient distraction achieved with postless techniques. 37
Our study showed that perineal numbness occurred in 0.8% and 22.7% of patients in the postless and post-assisted groups, respectively. A previous case series of 1000 patients presented no perineal-related nerve or soft tissue injuries with postless hip arthroscopy. 24 In 100 patients, Frandsen et al 9 found 32% of patients reported traction-induced nerve injury after post-assisted hip arthroscopy. Bailey et al 2 demonstrated that postoperative nerve palsy may be associated with increased traction force and duration, even when traction time is <1 hour. Other studies have shown that traction times >60 minutes were associated with increased complications in post-assisted hip arthroscopy.4,21
Several patient factors may contribute to increased traction time and force applied intra-operatively. For instance, male sex, high BMI, decreased hamstring flexibility, increased LCEA, and low Beighton scores have been shown to be predictor variables for increased applied traction force.10,24,28 In our analysis, although mean traction variables were similar between the 2 groups, the postless group required significantly less traction time and force. One study 28 found that postless hip arthroscopy was associated with lower stiffness coefficients, which reduced the maximal and holding traction forces needed for adequate hip distraction, thereby lowering the risk of traction-related complications. The use of a perineal post may also contribute to postoperative numbness. O’Neill et al 28 suggested that the counterforce from the perineal post increases overall system stiffness, which can amplify patient-specific factors affecting the required traction force and distance. Further prospective studies are needed to evaluate the effect of traction variables on the incidence of nerve injuries in both postless and post-assisted hip arthroscopy.
Despite the higher incidence of nerve injuries with post-assisted hip arthroscopy, there were no significant differences in pain scores between the 2 groups. However, given the variation in follow-up periods, the findings should be interpreted carefully. In the long term, Kraeutler et al 19 found no significant difference in the proportion of patients achieving SCB, MCID, and PASS for the VAS score. Similar pain scores between groups from our analysis may be explained by the fact that the nerve injury experienced by a compressive force generally manifests as negative nerve symptoms (ie, absence of sensation or function) rather than positive nerve symptoms (ie, neuropathic pain). Patients with pudendal nerve injury typically present with perineal numbness and/or sexual dysfunction, 13 such as erectile dysfunction in men, reduced sexual lubrication in women, and anorgasmia in both, rather than perineal pain. Furthermore, neuropathic pain occurs transiently during nerve reactivation and usually resolves over time, which may not be captured by pain scores measured at fixed intervals. The long-term PROM data for postless hip arthroscopy are promising, showing higher mHHS and UCLA Activity Scale scores. Researchers from this study suggest that this could be due to technical advantages of the postless approach, including enhanced hip joint mobility during femoroplasty and improved access for cam resection. 19 In the short term, postless hip arthroscopy has also been linked to a faster recovery with shorter time to discharge and similar pain levels when compared with post-assisted hip arthroscopy. 35
In our study, the Pink Pad was the most reported and utilized postless distraction technique. This technique can be modified and utilized in various hip distraction tables, such as the Hana table, Smith & Nephew distractor, ProFx table, and Arthrex distractor. 16 The Pink Pad, which costs roughly $100 USD, allows for a cost-effective way to perform postless distraction, as it can be utilized with standard hip arthroscopy tables. 16 Moreover, the Tutankhamun technique is also a cost-effective method, which puts heavy-duty tape over the patient's upper body on a normal operating room table while entering the central compartment. 33 The Hip Arthroscopy Post-less Procedure Impingement (HAPPI) technique using the Hip Positioning System (Smith & Nephew) is another cost-effective way to obtain postless traction using standard hip distraction tables and does not require the patient to be in the Trendelenburg position to maintain traction. 14 Several variations of postless distraction techniques exist, such as the use of the Trendelenburg position, as well as low-cost approaches such as use of a yoga mat and beanbag.7,16 More recently, a postless distraction technique was performed with no additional equipment using only a fracture table, distractor, surgical sheets, and safety straps. 38 When comparing the Pink Pad (Xodus Medical Inc) and CarePad (Ab Medica S.P.A.), Daghero et al 5 found that in both pads the pelvic displacement was <60 mm at 50-kg traction load. However, further research is needed to elucidate the optimal postless distraction technique. A concern among surgeons with adopting the postless distraction technique is the associated learning curve. However, a survey of hip preservation surgeons that frequently use a perineal post revealed that more than half of the surgeons felt confident in performing a postless hip arthroscopy after <5 cases. 18 The low learning curve and minimal associated equipment along with the significant reduction in nerve-related injuries are strong arguments for surgeons to consider transitioning toward routinely performing postless hip arthroscopy procedures.
Despite these benefits, postless hip arthroscopy may not be appropriate for all patients. Utilizing a post-assisted approach may be suitable for patients with stiffer hips or in cases where adequate distraction is of particular concern.10,27 Nevertheless, when using a post-assisted approach, surgeons should aim to avoid unnecessary complications by limiting traction time as well as traction force by utilizing the Trendelenburg position 27 and venting the hip capsule. 29 Future research should focus on identifying which patient characteristics are more suitable for either postless or post-assisted hip arthroscopy.
Limitations
This is, to the best of our knowledge, the first systematic review to directly compare the postoperative outcomes and complications between patients undergoing postless and post-assisted hip arthroscopy procedures. Despite this, there are limitations with the current study. The inclusion of only 5 nonrandomized and relatively small studies may limit the generalizability of our findings and restrict the statistical power of the meta-analysis. However, this is a testament to the paucity of available comparative data. While including noncomparative studies would have increased the sample size, such an approach would introduce significant variability in patient selection, surgical techniques, complication definitions, and follow-up protocols, thus compromising the reliability of direct cohort comparisons. Limiting the inclusion of only comparative studies aimed to enhance the internal validity of our study by limiting heterogeneity. The findings from this study are compiled from the best available evidence and offer early insight into the feasibility of the postless technique, which may assist surgeons in making informed decisions about its use in practice. Future large, randomized studies comparing both techniques should be conducted with the aim of comparing complication rates and hip-related PROMs. Further, 2 studies were retrospective and 1 conducted a retrospective analysis on prospectively collected data, which were subject to recall and reporting bias, potentially leading to outcomes being underreported. 40 Additionally, the lack of intraoperative details (ie, surgical time, traction force/time, Trendelenburg angle) reported coupled with the heterogeneity in the postless technique, variations in follow-up periods, and the lack of standardization in assessing nerve injuries could have influenced outcomes. Last, some studies provided minimal data regarding concomitant procedures being performed, which could affect the postoperative outcomes.
Conclusion
Our review showed that postless hip arthroscopy is associated with a significantly lower incidence of nerve or soft tissue injury and perineal numbness, as well as reduced traction time and force, compared with the conventional post-assisted technique. These findings from 5 comparative studies suggest that postless hip arthroscopy is a safer and viable alternative to the conventional post-assisted approach. However, the current paucity of comparative data in assessing complication rates and hip-related PROs between post-assisted and postless hip arthroscopy techniques warrants further investigation.
Footnotes
Final revision submitted September 8, 2025; accepted September 24, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.