
Abstract
Background:
Previous studies have demonstrated the risks of pudendal nerve and/or soft tissue complications due to the use of a perineal post during hip arthroscopy. Recently, various postless hip arthroscopy techniques have been described in the literature.
Purpose:
To assess the current international trends in the use of postless hip arthroscopy among hip preservation specialists.
Study Design:
Cross-sectional study.
Methods:
An anonymous 11-item survey was sent by email to all members of the International Society for Hip Arthroscopy (ISHA) in January 2022. Surgeons were asked various questions regarding their current use of post-assisted or postless hip arthroscopy, if they had changed their setup technique during their career and the reason for that change, and their perceived rate of pudendal nerve and/or perineal soft tissue injuries using their current technique. Descriptive statistics were used to report the results of each question. The Student t test was used to compare the number of years in practice between post-assisted and postless users. Fisher exact tests were performed to compare categorical rates of pudendal nerve and soft tissue complications between post-assisted and postless users.
Results:
A total of 126 surveys were completed from 431 ISHA members (29.2%). Sixty-one percent of the surgeons currently use a perineal post, while 33% use a postless technique. Seventy-five percent of the perineal post users and 98% of the postless users self-reported a rate of pudendal nerve and/or soft tissue injury of <1% (P = .015). Among 41 respondents who indicated changing their technique at some point, 59% reported doing so because of pudendal nerve and/or soft tissue complications. Among surgeons who switched from a perineal post to a postless setup, 71% indicated they have noticed a decrease in the rate of pudendal nerve and/or soft tissue complications.
Conclusion:
Although use of a perineal post is still a more common setup technique among hip arthroscopists, approximately one-third of surgeons use a postless technique. Surgeons who have switched to a postless technique often did so because of perineal complications, with the majority noticing a subjective decrease in these complications with the use of postless hip arthroscopy.
As the incidence of hip arthroscopy has rapidly increased in recent years, 23 so too have the techniques involved with hip arthroscopy, including patient positioning and setup. 4 Traditionally, hip arthroscopy has been performed with a perineal post since described by Byrd in 1994. 2 This allows the surgeon to maintain hip distraction while a traction force is pulled on the operative lower extremity. However, multiple studies have demonstrated the risks of pudendal nerve and/or soft tissue complications due to the use of a perineal post. 3,5,7,22 In a recent systematic review, Wininger et al 22 found a 7.1% incidence of post-related complications reported in prospective studies, including perineal soft tissue injury and pudendal neurapraxia.
In recent years, surgeons have developed a variety of novel patient positioning and/or setup techniques to avoid the use of a perineal post during hip arthroscopy. 4 These include use of a specialized hip distraction table with the patient in the Trendelenburg position, 11,20 the yoga mat technique, 17 the Tutankhamun technique, 16 the Beanbag technique, 13 and the hip arthroscopy postless procedure impingement technique. 8 Although a multitude of postless techniques have recently been published, it is unclear what proportion of hip arthroscopy surgeons are currently performing postless hip arthroscopy, which specific postless techniques are being used most commonly, and the perceived rate of perineal complications based on the various setup techniques used today. The purpose of this study was to assess the current international trends in the use of postless hip arthroscopy among hip preservation specialists. The authors hypothesized that a large proportion of the International Society for Hip Arthroscopy (ISHA) membership currently uses postless hip arthroscopy because of previous issues with pudendal neurapraxia.
Methods
After institutional review board approval (PR#22-003), an anonymous 11-item survey (Table 1) was sent by email to all members of ISHA in January 2022. A reminder email was sent approximately 2 weeks later to facilitate response. Surgeons were asked various questions regarding their current use of post or postless hip arthroscopy, if they had changed their setup technique at some point during their career and the reason for a change, and their perceived rate of pudendal nerve and/or soft tissue injuries using their current technique.
A Survey on the Use of Post Versus Postless Hip Arthroscopy a
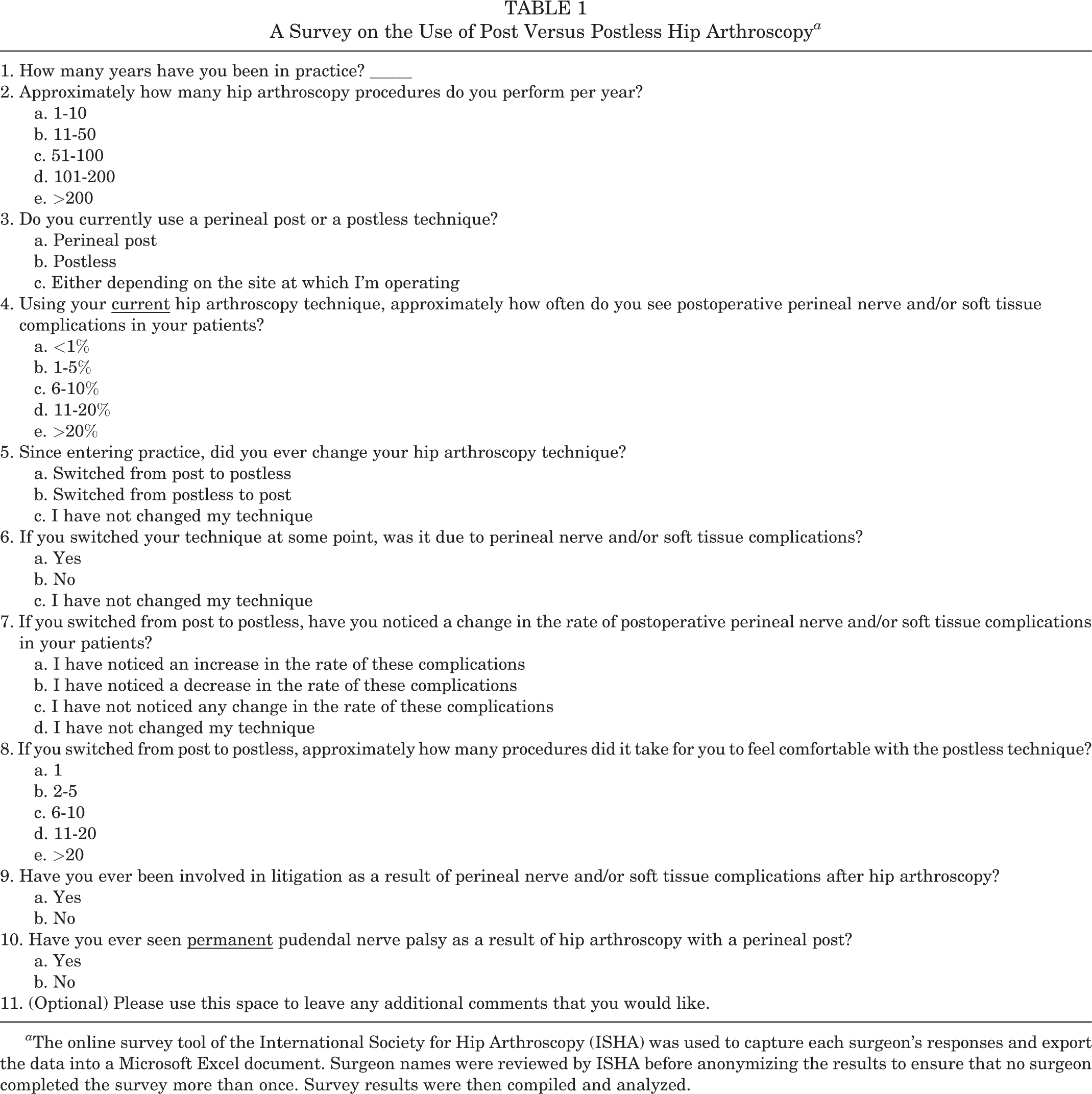
a The online survey tool of the International Society for Hip Arthroscopy (ISHA) was used to capture each surgeon’s responses and export the data into a Microsoft Excel document. Surgeon names were reviewed by ISHA before anonymizing the results to ensure that no surgeon completed the survey more than once. Survey results were then compiled and analyzed.
Statistical Analysis
Descriptive statistics were used to report the results of each question. The Student t test was used to compare the number of years in practice between post-assisted and postless users. Fisher exact tests were performed to compare categorical rates of pudendal nerve/soft tissue complications between post-assisted and postless users. Statistical analysis was performed using SPSS (Version 22; IBM). P <.05 was considered statistically significant.
Results
A total of 126 surveys were completed from 431 active ISHA members (29.2%). The gross results of the survey questions are shown in Table 2. Respondents reported being in practice for a mean of 14.2 years (range, 1-40 years), with no significant difference between post-assisted (mean, 15.1 years) and postless (mean, 12.9 years) users (P = .19). The majority of respondents (29%) reported a yearly hip arthroscopy caseload of 101-200 cases.
Gross Results of Survey Responses a

a N = 126 except where indicated.
b Data are given as mean (SD).
c N = 41, representing respondents who indicated they switched from post to postless.
Sixty-one percent of the surgeons currently use a perineal post, while 33% use a postless technique and 6% use either technique depending on the location at which they are operating. Seventy-five percent of the perineal post users and 98% of the postless users self-reported a rate of pudendal nerve and/or soft tissue injury of <1% (Table 3), with a statistically significant difference in the distribution between the 2 groups (P = .015). One post user reported a >20% incidence of perineal complications, and another post user reported an incidence between 11% and 20%.
Estimated Prevalence of Pudendal Nerve and/or Soft Tissue Complications in Perineal Post and Postless Users a

a Data are given as n (%). A statistically significant difference was found in the distribution of the 2 groups (P = .015).
Of the 41 respondents who indicated changing their technique at some point, 24 (59%) reported doing so as a result of perineal nerve and/or soft tissue complications (Table 2). For those surgeons who switched from a perineal post to a postless setup, the majority (46%) indicated that it took 2 to 5 procedures to feel comfortable with the postless system. Among surgeons who switched from a perineal post to a postless setup, 71% indicated they have noticed a decrease in the rate of perineal nerve and/or soft tissue complications. One surgeon noted initially changing from post-assisted to postless and then back to post-assisted, mentioning that postless is “most helpful for surgeons with long surgical times.” Overall, 9% of respondents have encountered permanent pudendal nerve palsy resulting from hip arthroscopy with the use of a perineal post, with 2% of surgeons previously being involved in litigation for such nerve and/or soft tissue complications.
Discussion
Based on the results of this study, a perineal post during hip arthroscopy remains the most common technique used by hip preservation specialists. However, many surgeons (33%) have switched to a postless setup, most often to avoid pudendal nerve and/or perineal soft tissue complications. Of those who have made the change to a postless technique, the majority (68%) have noticed a subjective decrease in perineal complications among their patients.
Interestingly, the vast majority (83%) of all respondents to our survey reported a perceived incidence of pudendal nerve and/or perineal soft tissue complications of <1% among their patients. Even among perineal post users, 75% reported a rate of perineal complications of <1%. Previous studies have reported rates of perineal and groin numbness as high as 41% to 59% while using a perineal post in hip arthroscopy. 5,10,15 In a systematic review of 24 studies, Habib et al 7 reported a 1.8% rate of pudendal nerve injury. However, this likely represents an underreporting, as Wininger et al 22 recently found that post-related complications are reported at a 5 times higher rate in prospective (7.1%) versus retrospective (1.4%) (P < .001) studies. The large discrepancy in self-reported groin-related complication rates is probably multifactorial, but some potential reasons are that patients are often hesitant to report symptoms of pudendal neurapraxia unless specifically asked, surgeons are often reluctant to probe patients on such issues, and many times the attending surgeon does not personally question/examine patients at the initial postoperative appointment when pudendal neurapraxia may still be present. Furthermore, the low rate of subjective reporting of complications by the surgeons in the current study may be partly due to the vague nature of the survey question, which did not clarify whether transient complications such as pudendal neurapraxia should be included.
We found that 33% of the ISHA surgeons currently use postless hip arthroscopy exclusively, with another 6% sometimes using a postless setup depending on the location at which they are operating. The concept of postless hip arthroscopy is relatively new. Although previous studies in 2007 13 and 2013 12 described postless techniques, commercially available postless distraction systems did not become available until 2018. Thus, there has been a rapid adoption of postless hip arthroscopy, as a result of not only the lack of groin-related complications mentioned above but also other benefits, such as shorter traction/operating room time (likely due to easier mobilization of the hip during cam resection) and shorter time to discharge from the postanesthesia care unit. 18 A recent study by Kraeutler et al 9 prospectively compared groin-related complications between patients undergoing hip arthroscopy by the same surgeon with versus without a perineal post. The authors found a significantly lower rate of postoperative groin numbness (0% vs 30%, P < .0001) and foot numbness (12% vs 32%, P = .04) in the postless group. In addition, 3 cases of temporary sexual dysfunction occurred in male patients undergoing hip arthroscopy with a perineal post versus none in the postless group. Despite the relative novelty of most postless techniques, 3 surgeon respondents to our survey mentioned that the use of a perineal post is outdated and that the “future is postless.”
The learning curve for surgeons performing hip arthroscopy has been previously studied, with a recent systematic review demonstrating a wide range of cutoff numbers proposed to achieve proficiency ranging from 20 to 519 cases. 6 As surgeons gain more experience, the average operative time and traction time decrease. 6 Other studies have shown a correlation between longer traction time and pudendal neurapraxia. 1,7 Thus, for new surgeons with potentially longer traction times, pudendal neurapraxia is of particular concern, and the use of postless hip arthroscopy can diminish this concern and allow surgeons to focus on the case at hand rather than minimizing traction time. In our study, 1 surgeon noted initially changing from post-assisted to postless and then back to post-assisted, mentioning that postless is “most helpful for surgeons with long surgical times.” However, even for experienced surgeons, longer traction times may be encountered with advanced central compartment procedures such as revision hip arthroscopy, labral augmentation/reconstruction, ligamentum teres surgery, and articular cartilage restoration, among others. For surgeons at teaching institutions, traction time with a postless technique may be less stressful while trainees (eg, residents, fellows, visiting board-eligible or board-certified surgeons) are learning hip arthroscopy. For established surgeons, our survey demonstrates that the learning curve when transitioning from a post to postless technique appears to be low, with most surgeons indicating it took only 2 to 5 procedures to feel comfortable with the new technique.
Two reasons cited by the survey respondents for not using a postless technique included lateral positioning and cost. Five surgeons reported that they use a perineal post with the patient in the lateral position because postless hip arthroscopy “is not an option” with lateral positioning. Although originally designed for supine positioning, the commercially available postless distraction system may also be used in the lateral position. The use of this device in the lateral position was originally validated in a cadaver laboratory setting and later adopted by numerous high-volume hip preservation surgeons worldwide. With regard to cost, 1 surgeon respondent to our survey noted that they are considering switching to a postless technique because of the ease of cam resection, although the cost of the specialized distraction table is potentially restrictive. However, a recent systematic review found that multiple low-cost, semireproducible techniques exist for postless patient positioning without using a specifically designed, researched, and tested surgical bed and setup. 4,8,13,16,17 There are potential disadvantages of postless hip arthroscopy techniques that place the patient in the Trendelenburg position, such as the potential for abdominal fluid extravasation. However, the use of commercially available products in conjunction with these techniques allows for increased friction between the patient and the operating table, such that Trendelenburg positioning can be minimized and in some cases eliminated.
The limitations of this study should be noted. First, the low response rate (29.2%) from ISHA members indicates that our findings may not reflect the current trends of all hip arthroscopists. However, this response rate is similar to other survey-type studies of society memberships. 14,19,21 Recall bias may have played a role in survey responses especially with regard to each surgeon’s perceived rate of perineal complications and the learning curve of the postless technique. In addition, the reported rates of groin-related complications may be underreported because of the wording of the survey questions, as transient complications (eg, pudendal neurapraxia) were not explicitly included in the question stem. The results are subject to response bias, particularly from surgeons who continue to use a perineal post. Surgeon responses were not validated for accuracy with regard to number of years of experience, annual case volume, and actual groin-related complication rate. We did not analyze or compare surgeon characteristics such as age, sex, or fellowship training. We also did not analyze geographic distribution of post versus postless use.
Conclusion
Although the use of a perineal post is still a more common setup technique among hip arthroscopists, approximately one-third of surgeons use a postless technique. Surgeons who have switched to a postless technique often did so because of perineal complications, with the majority noticing a subjective decrease in these complications with the use of postless hip arthroscopy.
Footnotes
Final revision submitted August 31, 2022; accepted September 26, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.H. has received research support from DePuy Synthes and Smith & Nephew; publishing royalties from SLACK Incorporated and Thieme Medical Publishers; consulting fees from Smith & Nephew; and speaking fees from Xodus Medical; he holds stock or stock options in PatientPop. O.M.D. has received royalties from Stryker and holds stock or stock options in HeapSi and MITA. A.J.S. has received research support from Isto Biologics; and consulting fees from Mitek, Medical Device Business Services, DePuy Synthes, and DePuy Orthopaedics; he holds stock or stock options in Biomet, CONMED Linvatec, Johnson & Johnson, Pfizer, Smith & Nephew, and Stryker.
AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from St. Joseph’s Health (PR#22-003).