
Abstract
Background:
Exercise therapy is recommended for the initial treatment of individuals with rotator cuff tears but fails in 25% to 50% of cases. Determining the baseline factors associated with patient-reported outcomes and tear propagation immediately following exercise therapy may improve treatment decision-making.
Purpose:
To prospectively identify factors associated with tear propagation and patient-reported outcomes immediately following a 12-week personalized exercise therapy program in individuals with symptomatic isolated supraspinatus tears.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
In total, 109 individuals were recruited for this prognostic prospective longitudinal cross-sectional study and underwent a 12-week personalized exercise therapy program for the treatment of rotator cuff tears. Individuals underwent assessments of passive glenohumeral range of motion (ROM), isometric muscle strength (internal and external rotation and abduction), and glenohumeral arthrokinematics during scapular plane abduction immediately before the initiation of exercise therapy. Immediately before and after the exercise therapy program, tear size was quantified using ultrasound (propagation defined as tear size change ≥4.6 mm), and individuals completed the Western Ontario Rotator Cuff (WORC) Index score. Logistic and multiple linear regression were used to determine if baseline glenohumeral contact path length, tear size, passive glenohumeral ROM, and isometric strength were predictors of tear propagation and patient-reported outcomes immediately following exercise therapy.
Results:
Overall, 7 individuals (8.5%) experienced tear propagation immediately following exercise therapy. Logistic regression analysis indicated that baseline tear size was the only predictor associated with tear propagation immediately following exercise therapy. There was a 29.0% decrease in the odds of tear propagation for each 1.0-mm increase in baseline tear size (odds ratio, 0.71; 95% CI, 0.51-0.99; P = .04). Higher baseline isometric internal rotation strength predicted higher WORC scores (P = .044).
Conclusion:
Immediately following a 12-week personalized exercise therapy program, the percentage of individuals who experienced tear propagation was low, and baseline tear size and higher internal rotation strength were associated with tear propagation and WORC scores, respectively. Thus, the current study identified factors immediately before exercise therapy that affect tear propagation and WORC scores following an exercise therapy program.
Well-informed prognosis of treatment outcomes following exercise therapy for individuals with rotator cuff tears may improve treatment success and reduce the economic burden associated with failed initial treatments. In individuals with symptomatic rotator cuff tears isolated to the supraspinatus tendon, important treatment outcomes include tear propagation and patient-reported outcomes. Progression of the tear to a second tendon (eg, the infraspinatus tendon) may complicate surgical intervention and affect joint function, leading to reductions in the magnitude of the joint reaction force at the glenohumeral joint and altered kinematics due to disruption of the transverse force couple.60,61 Operative treatment is believed to prevent tear propagation when compared with exercise therapy,19,78 but others hypothesize that tear propagation may occur due to muscle imbalances caused by the existing tear, resulting in overloading of neighboring rotator cuff tendons. 73 Thus, strengthening exercises may help restore balance to the intact rotator cuff musculature, preventing tear propagation. Despite the important implications, tear size and propagation have not been determined immediately before and after exercise therapy.
Additionally, because most therapies in orthopaedics are designed to improve quality of life, an individual's own perception of health status is an important indicator of the success of a treatment. 40 Therefore, predicting if an individual's perception of their pain and function will improve following treatment is crucial, as treatment is generally decided in a “patient-centered” manner. This notion is further supported by a large prospective cohort study that found expectations regarding the effectiveness of physical therapy were the strongest predictor of eventual surgery in individuals with symptomatic full-thickness rotator cuff tears. 18
Thus, identifying factors associated with tear propagation and patient-reported outcomes immediately following exercise therapy will provide information to identify individuals at risk of unfavorable clinical outcomes. Specifically, individuals more likely to experience tear propagation or unsatisfactory improvements in patient-reported outcomes may benefit from early surgery before the tear propagates, resulting in a more difficult surgery with worse outcomes.20,35 Conversely, individuals less likely to experience tear propagation could participate in exercise therapy given the beneficial effects on range of motion (ROM), muscle strength, and patient-reported outcomes commonly observed.4,21,45,57
Therefore, the objective of the current study was to prospectively identify factors associated with tear propagation and patient-reported outcomes immediately following a 12-week personalized exercise therapy program. It was hypothesized that baseline tear size, passive glenohumeral ROM, isometric muscle strength, and in vivo arthrokinematics are predictive of tear propagation and patient-reported outcomes immediately following personalized exercise therapy. Thus, the study was designed following peer-reviewed guidelines, where each variable was prospectively measured before the initiation of exercise therapy, with the treatment outcomes (ie, tear propagation and patient-reported outcomes) determined immediately following exercise therapy. 47
Methods
In total, 109 individuals (mean age 60.9 ± 9.9 years, mean body mass index [BMI] 28.7 ± 5.0 kg/m2) were recruited to participate in this prognostic prospective longitudinal cross-sectional study and provided institutional review board–approved written informed consent before performance of any research procedure (enrollment period April 7, 2017, to February 6, 2020). Individuals were included in the study if they had a symptomatic partial-thickness (>50% thickness of tendon) or full-thickness rotator cuff tear isolated to the supraspinatus tendon (confirmed via ultrasound). Additional inclusion criteria were age >40 years, BMI <40 kg/m2, and humerothoracic elevation range of 110° (ensuring the individual could participate in biplane radiography testing to prevent unnecessary radiation exposure). Individuals were excluded if they had a work-related injury, an asymptomatic rotator cuff tear, severely limited shoulder motion (<30° of internal or external rotation), diabetes mellitus, or previous participation in exercise therapy for the treatment of their rotator cuff tear.
Description of Personalized Exercise Therapy Program
Individuals underwent a 12-week personalized exercise therapy program (12 visits in total) for treatment of rotator cuff tears at the University of Pittsburgh Physical Therapy Clinical and Translational Research Center. 62 The program consisted of 2 visits per week for 4 weeks, then 1 visit per week for 2 weeks, and finally 1 visit biweekly until the conclusion of the 12 weeks. The program also included a home exercise program, and visit frequency was constructed to simulate current clinical practice and provide opportunities to progress while maximizing compliance with the prescribed home exercise program. The program used specific individualized criteria related to the participant's pain, ROM, and strength to tailor the interventions to each individual's unique clinical presentation. The overarching framework focused on restoring passive glenohumeral ROM and strengthening the rotator cuff and scapular muscles. However, depending on the initial staging of the individual based on tissue irritability, the impairments that needed to be addressed, and response to treatment, the selection and progression of interventions were individualized. 54
ROM, stretching exercises, and joint mobilization were performed as necessary to restore normal passive glenohumeral ROM. As ROM was restored, achievement of clinical criteria was determined when interventions focused on increasing the strength of the rotator cuff and scapular muscles and task-specific activities were initiated. Three levels of clinical decision-making led to the selection of individual-specific interventions during each visit. The first level dealt with determining the stage at which the individual presented. Information regarding the pain to restriction of motion sequence assisted the clinician in placing the individual in the high, intermediate, or low irritability stage (Table 1).
Criteria to Determine an Individual's Preexercise Therapy Irritability Status a

ADL, activity of daily living; ROM, range of motion.
Second-level decision-making related to determining if passive and/or active ROM was restricted. Restricted passive ROM led the clinician to determine the cause as either limited accessory motion or loss of tissue extensibility, and appropriate interventions were delivered (Figures 1 and 2). The final level of assessment made was the presence of weakness to determine the appropriate resisted and functional exercises. Exercise resistance and number of repetitions were determined based on a modification of the daily adjustable progressive resistance exercise program. 43
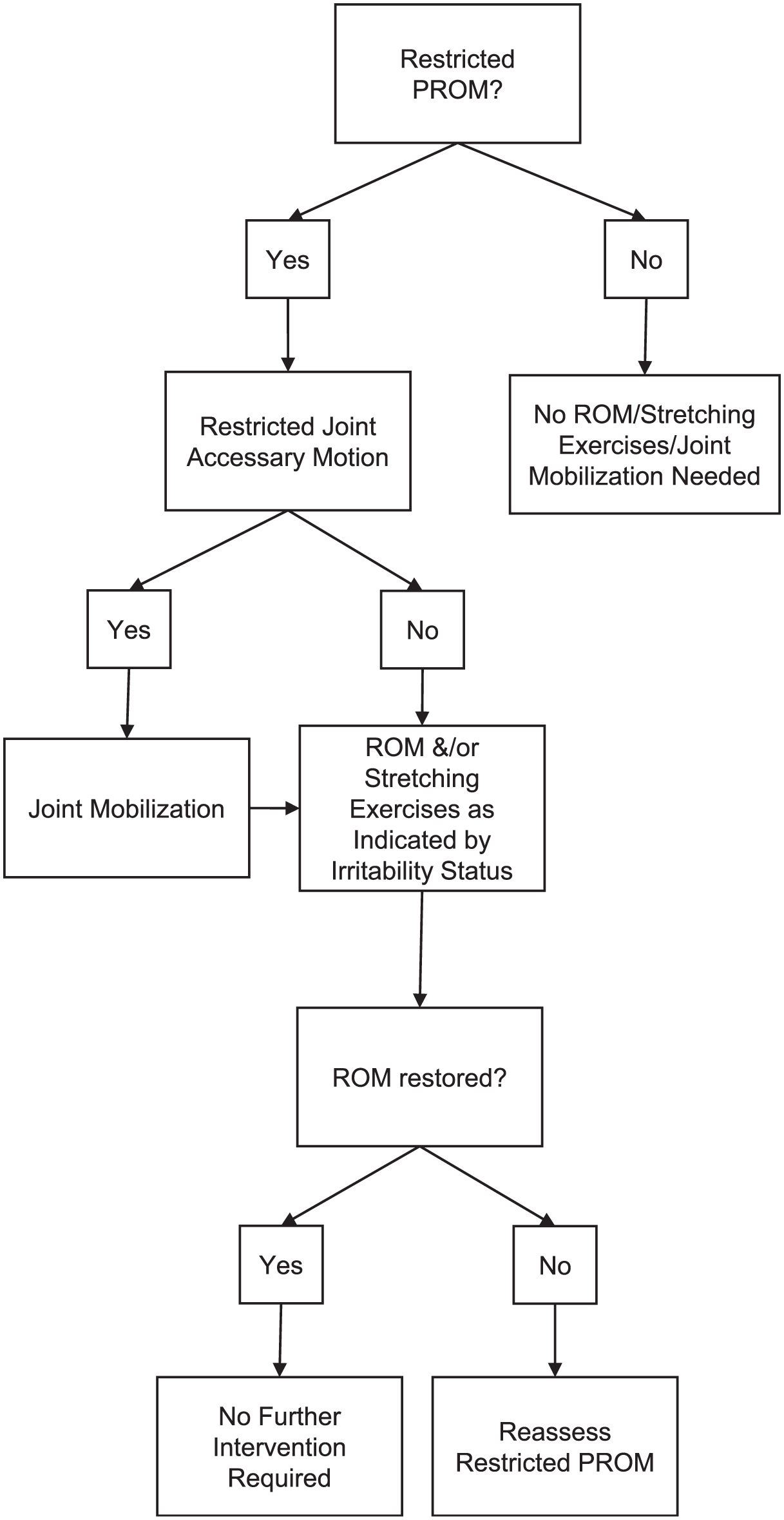
Flow diagram of the decision-making process for an exercise therapy program to progressively restore passive range of motion (PROM).
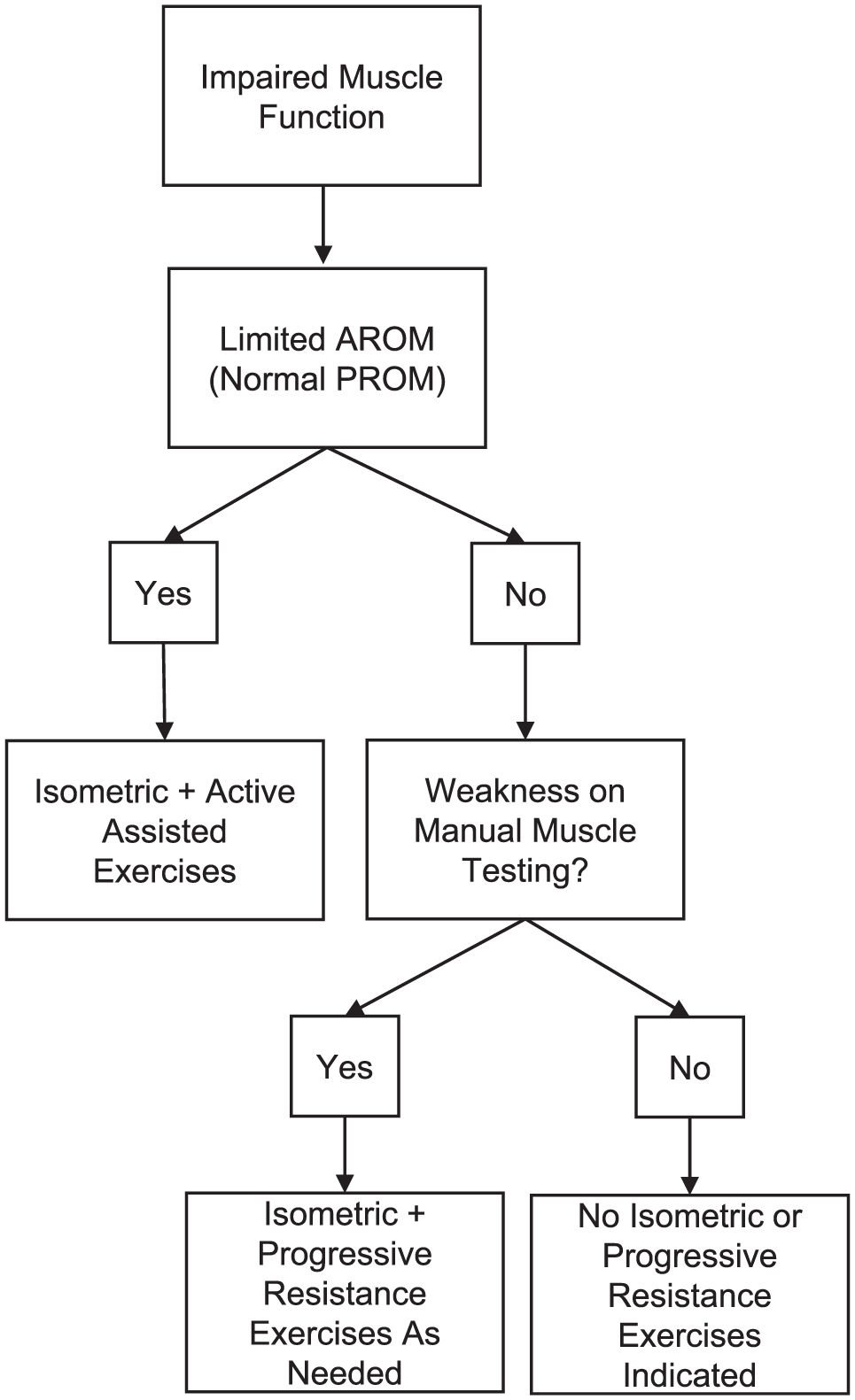
Flow diagram of the decision-making process for individuals with impaired active range of motion/muscle function to restore strength of the rotator cuff and scapular muscles throughout the 12-week individualized program.
Ultrasound Measurement of Rotator Cuff Tear Size
Ultrasound was used to quantify the anterior-posterior (AP) tear size within the supraspinatus tendon. Assessments were performed with a 6- to 15-MHz linear array transducer (LOGIQE9; General Electric) by a musculoskeletal radiologist. Individuals were seated with the glenohumeral joint in extension and internal rotation, with the involved side hand on the iliac wing to expose the supraspinatus tendon.63,71 Tear size was quantified as the AP distance of the widest portion of the defect of the tear measured perpendicular to a line tangent to the posterior edge of the long head of the biceps tendon in the acquired short-axis images. In the same short-axis image, the tear was defined as partial thickness if the defect did not span the entire thickness of the tendon. Conversely, the tear was defined as full thickness if the defect spanned the entire thickness of the tendon. Additionally, the subscapularis, infraspinatus, and teres minor tendons were also visualized and confirmed that the tear remained isolated to the supraspinatus tendon in all individuals. Diagnostic ultrasound has high sensitivity, specificity, and reliability for the detection and quantification of rotator cuff tears, with accuracy on the order of 1.0 mm or less.15,42,58,72,75,76
To determine if the change in tear size was greater than measurement error, we used the minimal detectable change of 4.6 mm that was established for 3 observers when measuring supraspinatus tear size on previously aquired ultrasound images. 30 To estimate the MDC, a subset of 15 randomly chosen ultrasound examinations from the current cohort and from varying time points (immediately before exercise therapy and at 6-week and 3-, 6-, and 12-month follow-ups) was provided by an independent laboratory member. Intraclass correlation coefficients ranged from 0.51 to 0.87 and increased with greater experience in the interpretation of ultrasound images. The standard error of measurement ranged from 1.3 to 1.8 mm and improved with experience. Using the standard error of measurement, the minimum detectable change was calculated to be 4.6 mm. Thus, any increase in tear size >4.6 mm was considered a true increase in supraspinatus tear size beyond measurement error. 30 Importantly, the currently defined threshold for tear progression is similar to previous studies evaluating the rate of tear size progression, which all used a 5.0-mm change in tear size to define progression.38,39,46,68
Patient-Reported Outcomes
Participants completed the Western Ontario Rotator Cuff (WORC) Index, which is a patient-reported outcome specifically used for individuals with rotator cuff tears. 40 The WORC has demonstrated evidence of reliability, validity, and responsiveness for individuals with rotator cuff tears.17,41 Possible scores for the WORC were from 0 to 100, where higher scores indicate greater function and less pain. The minimal clinically important difference for the WORC is 13.5 points. 23
Measurement of In Vivo Glenohumeral Arthrokinematics
Glenohumeral arthrokinematics during scapular plane abduction were measured using a synchronized biplane radiography system at 50 images/s.7,52,53,57 Individuals underwent a computed tomography (0.464 × 0.464 × 0.625 mm voxels) scan of the involved shoulder, and images were segmented using MIMICS 20 (Materialise) to create individual-specific humerus and scapula bone models. To assess glenohumeral function, individuals were seated with the involved glenohumeral joint centered in the system and performed scapular plane abduction. All individuals completed the movement with the elbow extended, and a metronome was used to help the participant maintain a steady abduction speed. Arm position in the desired plane was maintained using a laser pointer strapped to the ipsilateral hand, with individuals asked to keep the laser dot within a properly aligned strip of tape on a target surface. Three trials of scapular plane abduction were performed immediately before exercise therapy, and the trial in which maximum glenohumeral elevation was obtained was used for all analyses.
Biplane radiographs were distortion corrected, and the imaging system was calibrated following established procedures.7,21,57 Digitally reconstructed radiographs of the bone models were created from the computed tomography–based individual-specific bone models and the known geometry of the biplane radiography system. A semiautomated matching process was used to optimize the correlation between the digitally reconstructed radiographs and the distortion-corrected radiographs for each pair of synchronized images throughout the movement (accuracy of ±0.4 mm and ±0.5° for translations and rotations, respectively). 7
The local coordinate system for each humerus was constructed based on recommendations from the International Society of Biomechanics, with the origin located at the center of the humeral head. 77 The scapula coordinate system was modified to create a glenoid-based system to describe humeral motion with respect to the center of the glenoid. 57 Local coordinate system axes were aligned with the most AP and superior-inferior points on the glenoid rim, 6 with the superior and anterior directions considered positive. For each data frame, a 3-dimensional distance map was calculated between the humeral head and glenoid surfaces. The centroid of the 3-dimensional distance map was then quantified as the weighted average of the 200-mm2 region closest to the humeral head-glenoid contact, serving as an estimate of the contact center location.2,6
Glenohumeral contact center data were normalized to glenoid AP width and superior-inferior height. 6 The contact path length was calculated as the change in frame-by-frame position of the contact center, providing an estimate of the distance the humeral head articulated on the glenoid surface. Normalizing the contact center to AP width and superior-inferior height of the glenoid results in a contact path length normalized to glenoid size. The contact path length quantifies the amount of displacement of the humeral head on the articular surface of the glenoid, where a smaller contact path length may indicate the joint is functioning more like a ball-and-socket joint.
Measurement of Passive ROM and Isometric Muscle Strength
Passive glenohumeral ROM and isometric strength of the rotator cuff muscles were measured by 1 of 3 physical therapists who had been trained on the measurement procedures. Passive glenohumeral abduction was assessed using a goniometer on the involved side in the supine position. Passive glenohumeral abduction ROM was chosen because the movement is important for upper extremity function during daily tasks. Previous literature assessing isolated glenohumeral and overall shoulder ROM demonstrated intra- and interobserver repeatability ranging from 0.38 to 0.98 and 0.26 to 0.99, respectively, for various joint positions. *
Isometric strength measurements of the rotator cuff were taken as previously described,21,57 using a handheld dynamometer (Lafayette Manual Muscle Testing System; Lafayette Instrument Company) in 3 joint positions. Individuals were asked to perform a maximal isometric contraction strength according to their level of pain tolerance. However, the strength measurements were stopped and not collected if the individual expressed significant pain and discomfort. Isometric strength measurements included external and internal rotation with the arm at the side and abduction strength at 90° of humerothoracic abduction in the scapular plane. Measurements were taken 3 times in each position and averaged to determine isometric force production. All strength measurements were normalized as a percentage compared with the contralateral normal shoulder. The repeatability for assessing shoulder strength using a handheld dynamometer is acceptable, with an intraobserver repeatability of 0.57 to 0.99 for internal rotation and 0.87 to 0.98 for external rotation.5,12,36,55,65,70 Furthermore, interobserver repeatability has been shown to range from 0.72 to 0.97 for internal rotation and 0.64 to 0.98 for external rotation using a handheld dynamometer.5,12,36,65 All testers also underwent protocol training before initiation of the study.
Statistics
Continuous variables were reported as means and standard deviations, and categorical variables were reported as frequencies and percentages. Logistic and multiple linear regression were used, respectively, to determine if tear propagation and patient-reported outcomes immediately following a 12-week personalized exercise therapy program were predicted by glenohumeral contact path length, tear size, passive ROM during glenohumeral abduction, and isometric external, internal, and abduction rotation strength collected immediately before initiation of the exercise therapy program. The final set of predictors was arrived at via backward stepwise regression, starting with a model consisting of all variables that had a univariate association of P < .05. Tear propagation was coded as either 0 (no propagation) or 1 (propagation, defined as a change in tear size ≥4.6 mm) for the logistic regression analysis. Significance was set at P < .05.
Results
Overall, the cohort had varying symptoms and demographic characteristics in terms of tissue irritability, duration of shoulder pain, and type of occupational work. Specifically, 38 individuals began the program in the low-irritability stage, 55 in the intermediate-irritability stage, and 14 in the high-irritability stage (missing data for 2 individuals, categorized based on Table 1). Before entering the study, the duration of shoulder pain was ≤1 month for 14 individuals (12.8%), >1 to ≤3 months for 29 individuals (26.6%), >3 months to <6 months for 34 individuals (31.2%), and ≥6 months to ≤12 months for 32 individuals (29.4%). Eight individuals (7.3%) were current smokers, and 30 individuals (27.5%) were past smokers at the start of exercise therapy. The type of work varied where 43 individuals (39.5%) were mostly sedentary, 14 (12.8%) were sedentary (with substantial walking), 46 (42.2%) were moderately active (some lifting), and 6 (5.5%) were demanding (Table 2). Additional demographic and clinical characteristics for the entire cohort, as well as individuals who did or did not experience tear propagation, are shown in Table 2.
Demographic and Clinical Characteristics of the Entire Cohort and Those Who Did Not Versus Did Experience Tear Propagation a

Values are presented as mean ± SD or number (%). BMI, body mass index; HS, high school.
Overall, minimal restrictions in passive glenohumeral abduction were observed at baseline in the current cohort (Table 3). However, strength limitations relative to the contralateral side were observed for all isometric strength tests (Table 3). The greatest limitation in strength compared with the contralateral arm was isometric abduction strength in the scapular plane, where strength of the involved arm was on average 23.3% weaker than the noninvolved side. Regarding in vivo arthrokinematics, the displacement of the humeral head on the glenoid surface during scapular plane abduction was variable throughout the cohort with a standard deviation of 27.4% glenoid size (Table 3).
Descriptive Statistics for Baseline Factors for the Entire Cohort and for Each Regression Analysis a

Values are presented as mean ± SD (sample size). WORC, Western Ontario Rotator Cuff.
Tear size (both immediately before and after 12 weeks of exercise therapy) was collected in 82 participants (75.2%). However, complete data for all baseline predictors and tear size immediately following exercise therapy were collected in 68 individuals and used for the logistic regression analysis (Table 3). Importantly, all 7 individuals who experienced tear propagation had complete data and were included. Reasons for missing data included lost to follow-up, withdrawal from the study, inability to participate in follow-up research procedures due to COVID-19 restrictions, failure to attend a scheduled study visit, or poor image quality. For the full cohort, baseline tear size was 11.4 ± 5.7 mm and ranged from 0.5 to 28.3 mm. Seven individuals (8.5%) experienced tear propagation (change in tear size ≥4.6 mm) immediately following exercise therapy. The tear characteristics for individuals who did or did not experience tear propagation are shown in Table 4. Initial tear size for individuals who experienced tear propagation ranged from 4.6 to 10.7 mm. Tear propagation immediately after exercise therapy was predicted by only baseline tear size (odds ratio, 0.71; 95% CI, 0.51-0.99; P = .04), indicating a 29.0% decrease in odds of tear propagation for each 1.0-mm increase in initial rotator cuff tear size.
Tear Size and Thickness Before and After Exercise Therapy in Individuals Who Did and Did Not Experience Tear Propagation a

Values are presented as mean ± SD or number (%).
The WORC (both immediately before and after 12 weeks of exercise therapy) was collected from 98 participants (89.9%), of whom 66 participants (67.3%) achieved the minimal clinically important difference for the WORC (change >13.5). WORC scores immediately before and after exercise therapy were 61.2 ± 20.0 and 82.7 ± 18.2, respectively. However, complete data for all baseline predictors and the WORC score immediately following exercise therapy were collected in 78 individuals and were used for the regression analysis (Table 3). Reasons for missing data included lost to follow-up, withdrawal from the study, inability to participate in follow-up research procedures due to COVID-19 restrictions, failure to attend a scheduled study visit, or poor image quality. Higher internal rotation strength measured before exercise therapy was the only factor associated with the WORC scores following exercise therapy (β = 0.18; 95% CI, 0.0-0.4; P = .044). Based upon univariate analysis, external rotation strength was also included in the model as a predictor but did not significantly independently predict WORC scores following exercise therapy (β = 0.09; 95% CI, 0.0-0.2; P = .073). Given strength in the involved shoulder was normalized as a percentage compared with the noninvolved shoulder, the predicted WORC score immediately after exercise therapy would increase by 0.18 points for each 1% increase in strength when normalized to the noninvolved side.
Discussion
The findings of the current study have important clinical implications regarding the identification of factors that are associated with tear propagation and WORC scores immediately following exercise therapy in individuals with symptomatic supraspinatus tendon tears. Specifically, major findings immediately following a 12-week personalized exercise therapy program include (1) the risk of tear propagation (defined as an increase in tear size ≥4.6 mm) was low (8.5%), (2) a larger tear size immediately before exercise therapy was associated with decreased risk of tear propagation, and (3) greater internal rotation strength compared with the contralateral normal shoulder immediately before exercise therapy was associated with higher WORC scores.
Based on the current cohort, the risk of tear propagation immediately following exercise therapy is low. Individuals at risk of tear propagation may be identified before treatment based on their initial tear size, but a second independent analysis is needed to confirm. Only 7 individuals (8.5%) experienced tear propagation immediately following exercise therapy, where every 1.0-mm increase in baseline tear size reduced the risk of propagation by 29.0%. Interestingly, the total displacement of the humeral head on the glenoid surface (contact path length) during scapular plane abduction was not associated with increased risk for tear propagation. Theoretically, if the contact path length is longer, the intact rotator cuff in some individuals may not be controlling the humeral head on the glenoid surface as effectively leading to unfavorable joint function. However, tear propagation is multifactorial, and the variability in contact path length between individuals, as well as the low rate of tear propagation, may explain why no association was observed.
Intuitively, many individuals believe larger tears would be at greater risk for propagation. Studies indicate that larger tears, smoking, diabetes, more fatty infiltration, infraspinatus atrophy, supraspinatus atrophy, and subscapularis involvement are related to tear progression.22,38,44,50,51,79 However, the referenced studies include multiple tendon tears, which can lead to poorer tissue quality, scarring and adhesions to the retracted tendon, and more fatty infiltration compared with a tear isolated to the supraspinatus tendon.14,24,25,29-34,37,80 Thus, in cases of isolated symptomatic supraspinatus tear, the previous associations may not be generalizable. Factors such as tissue quality around the tear edges or the status of the rotator cable may play a larger role compared with the tear size alone. For example, smaller tears with an intact rotator cuff cable may be associated with degenerative tissue on the edges of the tear that would be more likely to tear, whereas larger tears may have already progressed to the rotator cable. Specifically, subject-specific and validated computational models of the rotator cuff demonstrated that propagation was strongly correlated with local material strength and stiffness near the tear tips. 74 Furthermore, propagation occurred at moderate strains, such as those associated with smaller loads or tears in sheep infraspinatus tendons (which is an established model for human supraspinatus tendon1,13,26-28). Additional research should focus on tear size and tissue quality at the edges of the tear, which may allow clinicians to identify individuals susceptible to tear propagation following exercise therapy. Given the low propagation rate, long-term follow-up is ongoing to determine if additional individuals experience tear propagation, which will provide more information regarding the current findings.
Higher baseline isometric internal rotation strength was associated with higher patient-reported outcomes immediately following exercise therapy. Specifically, individuals with greater subscapularis strength (and likely other force-generating muscles that contribute to internal rotation strength, ie, pectoralis major, teres major, latissimus dorsi) were predicted to achieve higher WORC scores immediately following exercise therapy, indicating an improved perception of one's pain, other symptoms, and function. Although isometric external rotation strength was not significantly associated with the WORC scores, posterior rotator cuff strength (ie, infraspinatus and teres minor) is likely still important given the dynamic balance with the subscapularis required to maintain the transverse force couple.10,11,61 Based on the results, external rotation strength (β = 0.09; 95% CI, 0.0-0.2; P = .073) may become significantly associated with WORC scores immediately following exercise therapy if a larger sample of individuals with isolated supraspinatus tears were investigated. Overall, individuals with better baseline strength may require fewer therapy sessions focused on muscle strength, allowing physical therapists to focus on pain management or other symptoms and functional deficits. Therefore, the current finding implies that individuals with higher baseline strength of the intact rotator cuff may be more likely to have better patient-reported outcome scores immediately following exercise therapy.
In combination, the major findings of the current work provide information to clinicians on factors that affect tear propagation and WORC scores following exercise therapy in individuals with symptomatic supraspinatus tendon tears. A limitation of the current study was that no imaging data, such as magnetic resonance imaging, were obtained to quantify fatty infiltration of the rotator cuff. 69 An additional limitation is missing data due to loss to follow-up, individuals missing a scheduled study visit, or poor ultrasound images, which may introduce selection bias, especially given the low rate of tear propagation observed. Furthermore, because ultrasound was used, additional pathology, such as a superior labrum AP lesion, labral tear, or proximal biceps pathology, was not investigated. Future studies investigating tear propagation should obtain imaging data to quantify tissue quality, which likely influences the risk of tear propagation.1,16,74 However, the current study provides important information on predictors of postexercise therapy outcomes (ie, tear propagation and patient-reported outcomes) in a prospective cohort of individuals with an isolated supraspinatus tear who underwent a highly controlled exercise therapy program. Future research is needed to validate the findings of the current study in a larger independent sample, to determine if the associations observed may provide actionable information to help clinicians identify individuals at risk of tear propagation and worse patient-reported outcomes following exercise therapy for the treatment of a symptomatic isolated supraspinatus tendon tear.
Conclusion
Using a prospective longitudinal cohort of individuals with symptomatic rotator cuff tears isolated to the supraspinatus tendon, we identified several baseline variables associated with tear propagation and patient-reported outcomes immediately following exercise therapy. Baseline tear size was associated with tear propagation, where individuals with larger baseline tears were at a decreased risk of propagation (risk of propagation decreased 29.0% with each 1.0-mm increase in baseline tear size). Furthermore, higher baseline isometric internal rotation strength, relative to the contralateral normal shoulder, was associated with higher WORC scores immediately following exercise therapy. Further research to validate these results in a larger independent sample is necessary to identify how these variables, as well as other variables, may help identify which individuals with an isolated supraspinatus tear may experience tear progression or worse clinical outcomes. Additionally, long-term assessment of predictors of tear propagation and patient-reported outcomes should be investigated to provide additional information for treatment decision-making.
Footnotes
Acknowledgements
The authors thank Camille C. Johnson, Tom H. Gale, Dennis E. Dever, Naomi E. Frankston, and Sabreen A. Megherhi for their contributions to kinematic data collection and processing. The authors also thank Christopher M. Gibbs, Satoshi Takeuchi, and Andrew C. Cordle for their contributions to ultrasound image acquisition and measurements.
Final revision submitted September 25, 2025; accepted November 9, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Departments of Orthopaedic Surgery, Bioengineering, and Physical Therapy at the University of Pittsburgh and National Institutes of Health grant 5R01AR069503. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pittsburgh (STUDY19020103).