
Abstract
Purpose:
To adapt the Rotator Cuff Quality of Life (RC-QOL) questionnaire into traditional Chinese (Chi-RC-QOL) and to evaluate the validity and reliability in patients suffering from rotator cuff pathologies in Hong Kong.
Methods:
The Chi-RC-QOL will be constructed using the forward-translation followed by the backward-translation method. Thirty consecutive patients with clinically and radiologically confirmed rotator cuff pathology were recruited. Descriptive statistics will be followed by validity assessment using comparison with the Constant Shoulder (CS) score, University of California Los Angeles (UCLA) Shoulder Rating Scale, and Western Ontario Rotator Cuff (WORC) score. Parametric data will be tested using Pearson’s correlation coefficient for the total scores. Reliability was assessed using a test–retest interval of 30 min. The Cronbach’s α and intraclass correlation coefficient were calculated.
Results:
Cronbach’s α and internal consistency scores were high for all parts of the Chi-RC-QOL, with Cronbach’s α ranging between 0.89 and 0.98. Internal consistency scores range from 0.82 to 0.92, which can be regarded as an excellent correlation. Test–retest reliability was excellent for all parts of the Chi-RC-QOL with good absolute reliability. Chi-RC-QOL correlates well with the CS score, UCLA Shoulder Rating Scale, and the WORC score, with all being statistically significant.
Conclusions:
The current study adapted the RC-QOL to traditional Chinese version. The analysis confirmed the validity and reliability of the Chi-RC-QOL questionnaire.
Level of Evidence:
III.
Introduction
Rotator cuff disease, a wide-spectrum from impingement syndrome without a tear to full-thickness tearing, is among the most common causes of shoulder pain. In the United States, shoulder pain leads to 4.5 million patient visits and 250,000 rotator cuff repairs are performed annually. 1 The diagnosis and treatment of all stages and types of rotator cuff disease could sometimes be challenging.
Further complicating decisions regarding treatment, clinical symptoms do not always correlate radiological findings. In an MRI study of 96 asymptomatic individuals, rotator cuff tear (RCT) was found in 35% of the subjects, the frequency increases with age with 54% of those over 60 years of age showing RCT. 2 Similarly, Gill et al. evaluated a population-based cohort, and the frequency of MRI findings of RCT was similar in people with shoulder pain, in people who have a history of shoulder pain, and in people who have never had shoulder pain. Therefore, the authors concluded that the “clinical symptoms do not necessarily match the radiological findings.” 3
The most extreme of the disease spectrum, massive RCT accounts for up to 40% of RCT. 4 It can be defined as tear of diameter >5 cm (by Cofield) or involvement of two or more tendons (by Gerber et al.). 5 However, the presentation of massive RCT can range from pain free with good function to pseudoparalysis with active forward flexion of less than 90° while passive motion is preserved.
In terms of management, Spennacchio et al. performed a systematic review of long-term outcome of arthroscopic rotator cuff repair (ARCR). Based on 16 studies (level II–IV evidence) with a follow-up of at least 5 years, the authors concluded that “ARCR appears to be effective and safe” although there is lack of high-level evidence. 6 However, from a systematic review carried out by Downie and Miller, there is insufficient evidence supporting operative or conservative management in those over 60 years of age with RCT. 7
The management of massive RCT is also evolving. In a recent review by Thes et al., he proposed an algorithm based on the chronicity of tear and also the presence of glenohumeral arthritis. 8 However, the recommendation was again based on a currently available level III or IV evidence. Greenspoon et al. reviewed different management options for massive RCT and noted that the re-tear rate following ARCR ranged from 25% to 57%, and the authors again highlighted the controversial association between anatomical integrity of the repair and functional status. 4 Re-tear rate was found to be related to size of tear and older age based on a systematic review. 9 Other commonly quoted factors associated with re-tear included fatty infiltration and atrophy. 10
Numerous outcome measures have been used in the literature, which has possibly led to varied reported efficacy of ARCR. 11 –13 Patient-reported outcomes include general outcome instruments, such as EuroQol (EQ-5D) or Short Form (SF) health surveys (SF-36 and SF-12), and disease-specific tools, such as Western Ontario Rotator Cuff (WORC) score, a 21-item self-report questionnaire with each item scored on a visual analogue scale (VAS). 13 On the other hand, joint specific outcome measures such as American Shoulder and Elbow Surgeons Shoulder Form and Constant Shoulder (CS) Score are based on both patient-reported and clinician-based assessments. 13
CS score was first published in 1987. It was one of the first outcome measures developed to assess shoulder function. It is the recommended scoring system of the European Society of Shoulder and Elbow Surgery. In this score, 35 points are allocated for subjective assessments of pain and activities of daily living by the patient and 65 points for objective measures of the patient’s range of motion and strength by the clinician. The strength of this instrument is that the method for administering the tool was easy with clear instruction. However, it may not be effective in evaluating shoulder instability and has not been validated for assessing improvements in shoulder function after treatments. 14
University of California Los Angeles (UCLA) Shoulder Rating Scale was published in 1981. 13 It consists of both objective measures of active forward flexion and strength by the clinician and subjective measures of pain, satisfaction, and function by the patient. It has a maximum score of 35, the higher the score, the better the outcomes. It was intended to be used in studies of patients undergoing total shoulder arthroplasty for arthritis of the shoulder. It was subsequently used also for patients with other shoulder conditions, for example, rotator cuff disease and shoulder instability. One of the drawbacks of this rating scale was that it did not justify the attribution of weighted scores to items, and patients’ opinions were not surveyed during the development stages. 15 Both CS score and UCLA Shoulder Rating Scale were developed before the introduction of modern outcome tool development methodology.
The WORC score was developed to analyze health-related quality of life in patients with rotator cuff disease. 13,16 Similar to the Rotator Cuff Quality of Life (RC-QOL), it consists of 21 items and is divided into five parts: part A (physical symptoms, six questions), part B (sports/recreation, four questions), part C (work, four questions), part D (lifestyle, four questions), and part E (emotions, three questions). Each question is answered on a 100 mm VAS, with a total score of “0” being the lowest score and “2100” being the highest score; the higher the score, the worse the quality of life. The WORC score was comprehensively tested during its development. Items were generated by reviewing relevant literatures and interviewing both clinicians and patients. Questions were selected based on the most important factors from patients’ perspective. It is a valid and reliable measurement tool in evaluating treatments in patients with rotator cuff disease.
The RC-QOL Index was introduced by Hollinshead et al. in 2000. 12 It consists of five parts: part A (symptoms and physical complaints, 16 questions), part B (work-related concerns, 4 questions), part C (sports and recreational activities, 4 questions), part D (lifestyle, 5 questions), and part E (social and emotional aspects, 5 questions). Each question is answered on a 100 mm VAS with “0” being the lowest score and “100” being the highest score. The total score represents a percentage. It is a 34-item self-administered questionnaire that has demonstrated excellent reliability, validity, and ability to discriminate between large and massive cuff tears. 12 Boorman et al. applied RC-QOL to nonoperative management of patients with chronic full-thickness RCT. Based on univariate logistic regression analysis, the baseline RC-QOL was found to be predictive of success or failure of conservative treatment. 17 RC-QOL has been adapted to Italian, German, and Turkish versions. At present, there is no Chinese version of RC-QOL. In our locality, only 4.3% of the population (2016) are English speakers according to Hong Kong Government website on Hong Kong facts that was last revised in February 2019. Therefore, traditional Chinese version will definitely aid the assessment of local patients. Our objective is to adapt the RC-QOL questionnaire into Chi-RC-QOL and to evaluate the validity and reliability in local patients suffering from rotator cuff pathologies. Our hypothesis is that Chi-RC-QOL is valid and reliable.
Methods
This study was approved by The Kowloon West Cluster Research Ethics Committee, and all patients who participated in this study gave verbal informed consent.
Translation
Our study aimed to first perform a cross-cultural adaptation of the RC-QOL based on Beaton’s guideline. 18 First of all, forward translation, that is, from English to Traditional Chinese, was carried out by an informed nurse and an uninformed linguistic teacher. Then, any discrepancies with translators’ reports were resolved. This is followed by a back translation by a native English speaker with no medical background. Further discrepancies were resolved, and consensus was reached after review with all translators, surgeons, and researchers.
Patients
Thirty consecutive local patients (median age 59, range 28–68 years) who are able to read and understand written Traditional Chinese and with clinically and radiologically confirmed rotator cuff pathology (6 impingement, 8 partial thickness RCT, and 16 full thickness RCT) were recruited. Clinical definition of impingement syndrome referred to having one or more of the following findings, including tenderness over subacromial space, positive painful arc, reproduction of pain with specialty testing, for example, Neer, Hawkins, and so on. Radiographical evaluation of rotator cuff pathology was by means of MRI. Of the eight partial thickness RCT, six of them were supraspinatus and two of them were involving two or more rotator cuff tendons. Of the 16 full thickness RCT, 3 of them were supraspinatus and 13 of them were involving 2 or more rotator cuff tendons. There were 11 females (median age 65, range 51–67 years) and 19 males (median age 58, range 28–68 years). Patients were excluded from the study if they had autoimmune or inflammatory joint disease as they often involve multiple joints and may have systemic involvement, which might affect the scoring in outcome measures. Patients who were unable to complete questionnaires due to language problem or cognitive disorders were also excluded. All 30 consecutive local patients who were screened fulfilled the inclusion criteria, and none of them was excluded.
Measurements
The Chi-RC-QOL questionnaire (see Online Appendix) was completed by all patients. In addition, CS score, UCLA Shoulder Rating Scale, and WORC score (aggregate score) were used to assess for validity and they were carried out consecutively. The Chi-RC-QOL was repeated after 30 min to evaluate the test–retest reliability of the questionnaire. The first set of Chi-RC-QOL for each patient was defined as Chi-RC-QOL 1, while the second set of Chi-RC-QOL that was carried out 30 min later was defined as Chi-RC-QOL 2. Neither the clinicians nor the therapists were blinded while carrying out the outcome measures.
Statistical analysis
Data were recorded using Microsoft Excel for Mac and analyzed using Stata 14. All tests were two-tailed and conducted at a 5% level of significance. The data are reported as the mean ± standard deviation. Parametric data were tested using Pearson’s correlation coefficient for the total scores. Internal consistency of the RC-QOL and relative reliability was evaluated by Cronbach’s α and intraclass correlation coefficient (ICC), respectively. A p value of <0.05 was set to be statistically significant. The ICC values were interpreted according to the general guidelines of Fleiss, 19 where ICCs > 0.75 were referred as “excellent,” >0.4 as “fair to good,” and <0.4 as “poor.” Higher standard error of measurement (SEM) scores suggest higher margin of error and poor absolute reliability. 20
Results
There were no major difficulties or problem encountered during forward–backward translation of Chi-RC-QOL. During the recruitment of patients, they all agreed to take part in the study after we explained about our study.
The mean scores of each of the questionnaires are shown in Table 1. Internal consistency and reliability of Chi-RC-QOL were shown in Table 2. Cronbach’s α and internal consistency scores were high for all parts of the Chi-RC-QOL with Cronbach’s α ranging between 0.89 and 0.98. Internal consistency scores range from 0.82 to 0.92, which can be regarded as excellent correlation. 19 Test–retest reliability was excellent for all parts of the Chi-RC-QOL, and they all carry a relatively low SEM score, which indicates good absolute reliability.
Descriptive values of all scores.
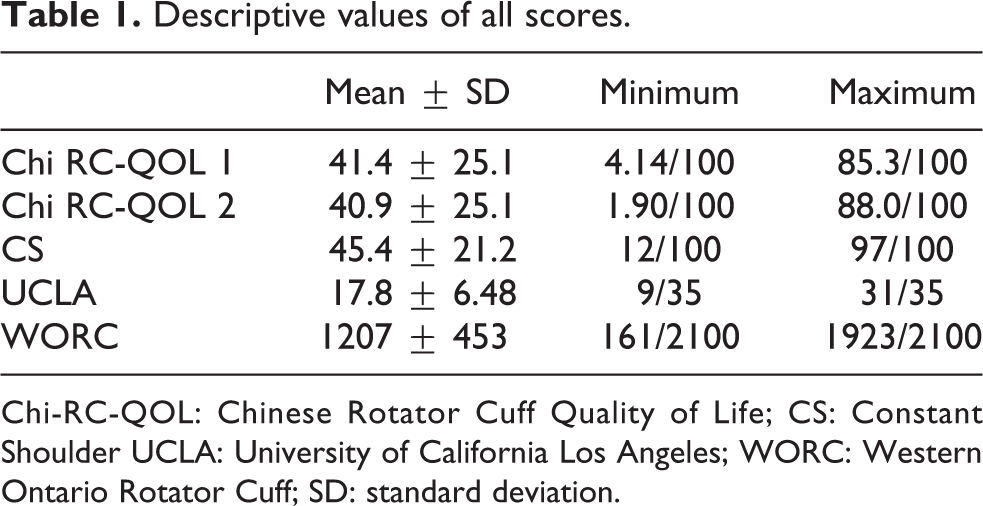
Chi-RC-QOL: Chinese Rotator Cuff Quality of Life; CS: Constant Shoulder UCLA: University of California Los Angeles; WORC: Western Ontario Rotator Cuff; SD: standard deviation.
Internal consistency and reliability of Chi-RC-QOL.
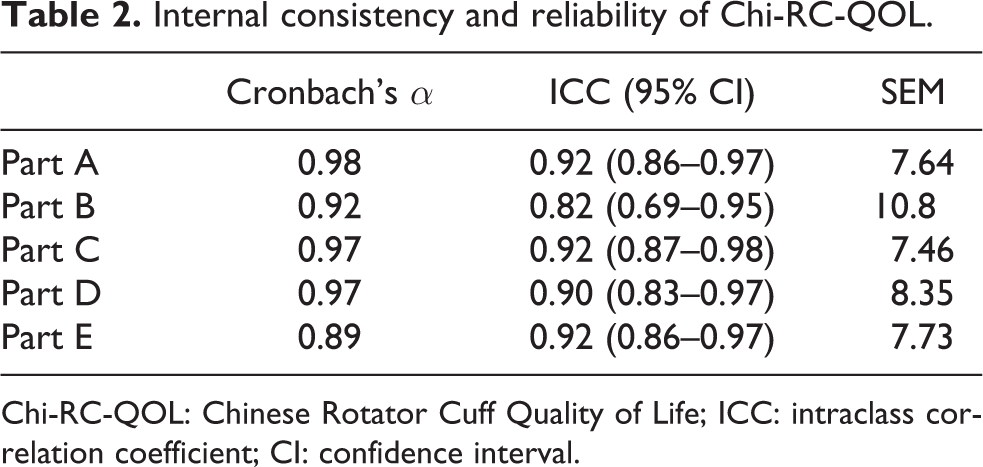
Chi-RC-QOL: Chinese Rotator Cuff Quality of Life; ICC: intraclass correlation coefficient; CI: confidence interval.
Table 3 shows the correlations between the Chi-RC-QOL and the CS score, UCLA Shoulder Rating Scale, and the WORC score. The result demonstrated good correlation between Chi-RC-QOL and the other measurement tools with all being statistically significant: Chi-RC-QOL 1 and the CS (r = 0.54, p < 0.05); Chi-RC-QOL 1 and the UCLA (r = 0.44, p < 0.05); Chi-RC-QOL 1 and the WORC (r = −0.76, p < 0.05); Chi-RC-QOL 2 and the CS (r = 0.52, p < 0.05); Chi-RC-QOL 2 and the UCLA (r = 0.43, p < 0.05); and Chi-RC-QOL 2 and the WORC (r = −0.80, p < 0.05).
Pearson’s correlation scores for the Chi-RC-QOL, CS score, UCLA Shoulder Rating Scale, and the WORC score.
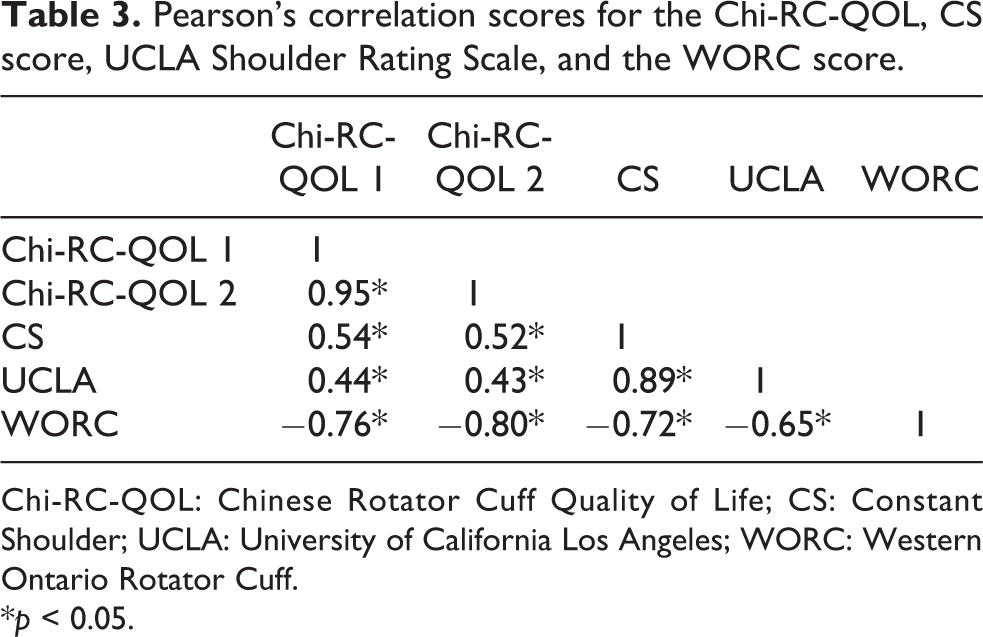
Chi-RC-QOL: Chinese Rotator Cuff Quality of Life; CS: Constant Shoulder; UCLA: University of California Los Angeles; WORC: Western Ontario Rotator Cuff.
*p < 0.05.
Table 4 shows the correlations for the similar subheadings of the Chi-RC-QOL and the WORC. High correlations were found for all subheadings: physical symptoms (r = −0.76, p < 0.05), work-related concerns (r = −0.51, p < 0.05), recreation and sports (r = −0.61, p < 0.05), lifestyle (r = −0.66, p < 0.05), and social emotional aspects (r = −0.66, p < 0.05).
Pearson’s correlation scores for each part of Chi-RC-QOL and WORC questionnaires.
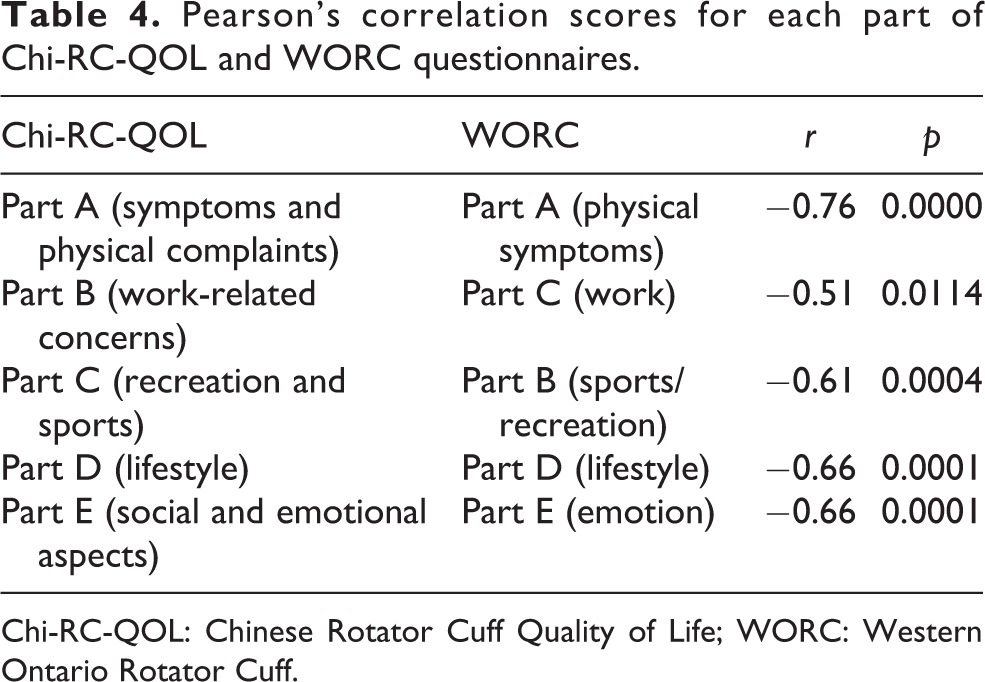
Chi-RC-QOL: Chinese Rotator Cuff Quality of Life; WORC: Western Ontario Rotator Cuff.
Discussion
The most important finding of this study was that it revealed satisfactory internal consistency, relative reliability, and validity of Chi-RC-QOL in assessing local patients with rotator cuff pathology in Hong Kong.
Further reliability testing within the subscales of the Chi-RC-QOL demonstrated excellent internal consistency and reliability with low margin of error.
The validity of Chi-RC-QOL was tested with CS score, UCLA Shoulder Rating Scale, and the WORC score. The Chi-RC-QOL showed good correlations with all three of the assessment tools. In addition, correlations for the similar subheadings of the Chi-RC-QOL and the WORC were evaluated. High correlations were found for all subheadings.
Although the relatively small sample size of 30 patients can be regarded as a limitation, the number of patients recruited in our study is comparable to other similar studies, 30 patients in Turkish version and 22 patients in Italian version. 21,22 After discussion among the authors, we decided to carry out our study with a sample size of 30. Our study results were comparable to the other adaptations and translated versions of the RC-QOL. 21,22,23 Also, Chi-RC-QOL was found to be a valid and reliable assessment tool in our study. Another potential limitation of the study is that test–retest was carried out on the same day with only 30 min of time lag. In theory, the test–retest intervals should be long enough so that patient is less likely to be able to recall their prior responses. Practically speaking, this will impose tremendous difficulties and workload to our frontline health-care staff and inconvenience to our patients if, for example, we asked our patients to come back in 2-day time for the retest. With the current logistic, patients who took part in our study reflected to us that they found it reasonable and the content of Chi-RC-QOL was easily comprehensible.
RC-QOL could also be used to assess patient’s quality of life postoperatively in patients undergoing rotator cuff repair. Therefore, in the future, we hope to carry out a prospective study using Chi-RC-QOL as an objective, valid, and reliable assessment tool to evaluate the operative outcome of local patients with rotator cuff pathology in Hong Kong.
Conclusion
Quality of life for patients with rotator cuff pathology is often used in research and in clinical practice to compare the effectiveness of different management modalities and monitor patient progress. Therefore, it is essential to use a validated questionnaire to do so. Our study adapted the RC-QOL to traditional Chinese version. The analysis confirmed that Chi-RC-QOL questionnaire is a valid and reliable tool to assess local patients with rotator cuff pathology in Hong Kong.
Supplemental material
Supplemental Material, Chi-RC-QOL_questionnaire_(JOTR)_1_-_Appendix - Chinese version of the Rotator Cuff Quality of Life questionnaire: Cross-cultural adaptation and validation in rotator cuff-impaired patients in Hong Kong
Supplemental Material, Chi-RC-QOL_questionnaire_(JOTR)_1_-_Appendix for Chinese version of the Rotator Cuff Quality of Life questionnaire: Cross-cultural adaptation and validation in rotator cuff-impaired patients in Hong Kong by Ho-ming Li, Jackie YM Chau, SB Woo, J Lai and WL Chan in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Acknowledgements
The authors would like to acknowledge Ms Joanna Chan and Ms Cherya Cheung for their help in translation of the questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by the Tung Wah group Hospital Research Funds, and the second author received technical support during her AO Clinical Investigation and Documentation Research Fellowship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.