
Abstract
Background:
Rotator cuff repair is one of the most common surgical procedures performed on the shoulder. Previous studies have indicated that pain and disability can vary significantly between patients with similarly appearing rotator cuff tears on diagnostic imaging. Prior literature has compared functional outcomes between operative and nonoperative treatments as well as variability in surgical techniques. However, few studies have examined postoperative outcomes based on patient factors such as sex.
Purpose:
To compare patient-reported outcomes after rotator cuff repair between men and women.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 283 patients (153 male, 130 female) who underwent primary arthroscopic rotator cuff repair were included in this study; of those, 275 patients (97.2%) completed 1-year follow-up. Patient-reported pain visual analog scale (VAS), Veterans RAND 12-item Health Survey (VR-12 mental and physical components), American Shoulder and Elbow Surgeons (ASES), and Single Assessment Numeric Evaluation (SANE) scores were collected preoperatively and at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year postoperatively using an electronic outcomes system.
Results:
Women reported higher VAS pain scores when compared with men preoperatively (P < .01) and at 2 weeks (P < .01), 6 weeks (P < .01), and 3 months (P = .02) postoperatively. Additionally, women experienced a greater overall change in the mean VAS score preoperatively when compared with 1 year postoperatively (P < .01). The use of narcotic pain medication 2 weeks after surgery was greater in women (P = .032). Women had significantly lower preoperative VR-12 mental scores (P = .03) and experienced a greater increase in the mean VR-12 mental score preoperatively when compared with 1 year postoperatively (P < .01). Men had higher ASES scores preoperatively (P < .01) and at 3 months postoperatively (P < .01). Women experienced a greater overall change in the ASES score preoperatively when compared with 1 year postoperatively (P < .01).
Conclusion:
Women reported greater pain and decreased shoulder function compared with men during the initial 3 months after arthroscopic rotator cuff repair. There were no sex-based differences in patient-reported outcomes at 1-year follow-up. The results of this study indicate that there are sex-related differences in the early postoperative recovery of patients undergoing rotator cuff repair, contributing to postoperative expectations for both clinicians and patients alike.
Rotator cuff tears are common but complex injuries that can cause significant individual disability and socioeconomic burden. 16,35 Several previous studies have examined the outcomes of nonoperative versus operative interventions in the treatment of rotator cuff injuries. 11,19,22,29,30 While nonoperative treatment is initially recommended, an operative intervention is often required for patients who experience persistent pain and decreased function. 19,30 Previous literature has examined outcomes based on rotator cuff surgical techniques in addition to evaluating prognostic factors for retears and prolonged recovery. ∥
A 2001 Institute of Medicine report highlighted the need for sex-specific research in all types of medical studies, from the cellular to societal levels. 15 Few studies to date have primarily focused on the relationship between sex and patient-reported outcomes after rotator cuff repair. Of these studies, they have generally demonstrated worse pain, function, and greater disability in female patients both preoperatively and postoperatively. 6,26 Expanding research on sex differences in outcomes after rotator cuff repair is warranted and is an important component to providing comprehensive care, particularly as sex and gender topics have become part of mainstream media. In addition, few studies have examined the influence of sex on postoperative narcotic use after rotator cuff repair, and given the rise of prescription opioid use and abuse, such information is pertinent to determine the best course of early postoperative pain management. 9
Given the limited data examining the influence of factors such as sex on outcomes after arthroscopic rotator cuff repair, the goals of this study were to (1) examine the influence of sex on patient-reported outcomes, including pain and shoulder function, before and after primary arthroscopic rotator cuff repair and (2) identify any sex-based differences in the use of narcotic or nonnarcotic pain medication in the early postoperative period. Based on the findings suggested by prior studies, and on clinical observations by the principal investigator (E.G.M.), the null hypothesis was there would be no differences in outcomes between female and male patients within the first postoperative year after arthroscopic rotator cuff repair.
Methods
Study Population
Data were prospectively collected on consecutive surgical procedures performed by 3 surgeons at 2 large academic institutions and retrospectively reviewed for the present study. Permission was obtained from our institutional review board, and all patients signed an informed consent document. We utilized an electronic surgical outcomes registry for data collection. Patients who underwent rotator cuff repair and participated in the outcomes registry from July 2012 to June 2015 were screened based on inclusion and exclusion criteria. Inclusion criteria were the following: primary arthroscopic rotator cuff repair during the study period, at least 1 year from the date of surgery, and age older than 18 years. Exclusion criteria were the following: revision rotator cuff repair, open rotator cuff repair, advanced glenohumeral arthritis, and postoperative complications.
All patients followed the standard postoperative rehabilitation protocol for rotator cuff repair. All patients also followed a standard postoperative pain management protocol. A multimodal approach to pain control was utilized. All patients received a perioperative peripheral nerve block. For postoperative pain control, patients were instructed to take 5 to 10 mg oxycodone every 4 hours for moderate pain and 1000 mg acetaminophen every 6 hours. Additionally, all patients were given a Cryo/Cuff (DJO Global) shoulder wrap for cryotherapy.
At each designated data collection point, participants were distributed an electronic survey specific to that time point. If a patient did not initially fill out the designated questionnaire, 1 email reminder and 1 telephone call reminder were made by a study author (K.D.G.) to increase compliance. No paper questionnaires were used.
Data Collection Elements
Patients who consented and were enrolled in the electronic outcomes data capture system were distributed electronic surveys preoperatively and at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year postoperatively. Multiple validated measures were included within each study time point to accurately capture pain levels and shoulder function. The primary outcome measure was the visual analog scale (VAS) for pain. Secondary outcome measures were the American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE), Veterans RAND 12-item Health Survey (VR-12) mental component summary (MCS), and VR-12 physical component summary (PCS).
The VAS pain score was collected at all study time points. Pain was recorded on a sliding scale and scored from 0 to 10 (0 = no pain, 10 = worst possible pain). 31 The ASES and SANE were assessed at the preoperative, 3-month, 6-month, and 1-year time points. The ASES was scored on a 100-point scale, with 2 subsets of points: pain (50 points) and shoulder function for daily living (50 points). 21 The SANE was scored on a 100-point scale (0 = severely abnormal function, 100 = normal function). 36
The VR-12 MCS and PCS were assessed at the preoperative, 6-month, and 1-year time points. The VR-12 is a well-known health-related quality of life measure assessing 8 health domains that include physical ability/pain, social components, and mental health status. Accordingly, the VR-12 can be subdivided into mental and physical components, providing a more specific assessment of how a pathological process affects the patient’s perception of his or her physical and mental health. Each component is scored out of 50, with higher scores indicating better outcomes. The VR-12 is an abbreviated survey of the VR-36, a modified version of the SF-36, which has been demonstrated as a validated measure of patient-perceived health-related quality of life. The greatest utility of the VR-12 is its use for measuring the effectiveness of a particular intervention when working at the population level; it is therefore most applicable when comparing groups of patients before and after an intervention rather than assessing individual change. VR-12 MCS and PCS scores are referenced to a metric centered at 50.0. 32
The secondary outcome in this study was patient-reported use of pain medication, including narcotic pain medication, nonnarcotic pain medication, and sleeping medication collected 2 weeks after the date of surgery. Participants were prompted to self-report the current use of each aforementioned medication at the time of the survey.
Patient characteristics included sex, age at the time of surgery, body mass index, smoking status, history of diabetes, and history of workers’ compensation injuries. In addition, operative details such as primary or revision, open or arthroscopic, repair technique, acute or chronic nature of the injury, and degree (partial/full) of the tear were recorded. The size of the tear was confirmed on magnetic resonance imaging by the principal investigator.
Statistical Analysis
A descriptive analysis of demographic variables was performed. Means and standard deviations were calculated for continuous variables, and frequencies and percentages were calculated for categorical variables. Because of potential confounding effects from tear size and tear thickness, we additionally investigated their associations with primary outcome measures at each time point.
We used linear mixed-effects models to assess the associations between primary outcomes and sex, controlling for time point. We included the interaction between sex and time point in the models to examine whether the effect of sex on primary outcomes varied by time point. If no significant interaction was found between sex and time point, we then excluded it from the models. If a significant interaction was found, we further investigated sex differences in the mean changes in patient-reported outcomes from the preoperative to the designated postoperative time point.
To assess postoperative medication use, we first examined the frequencies and percentages of narcotic, nonnarcotic, and sleeping medication use overall and by sex. We then used the chi-square test to assess the associations between medication use and sex. All analyses were conducted using SAS version 9.4 (SAS Institute), and P < .05 was indicative of statistically significant results.
Results
A total of 314 patients underwent rotator cuff repair and participated in the outcomes registry from July 2012 to June 2015. There were 25 patients who underwent arthroscopic revision rotator cuff repair, 4 patients who underwent open rotator cuff repair, and 2 patients who underwent open revision rotator cuff repair who were excluded from analyses. Thus, 283 patients were included in the cohort for subsequent analyses, and 275 (97.2%) patients completed a survey at 1-year follow-up.
Of the 283 patients, 153 (54.1%) were male and 130 (45.9%) were female. There were 10 patients (3.5%) who indicated a current smoking status, 8 patients (2.8%) who had a history of diabetes, and 29 patients (10.2%) who reported their injury as a workers’ compensation case (Table 1). There was a single female patient missing “type of repair” data in Table 1. There was no statistical difference between the 2 groups with respect to these variables.
Demographic Characteristics and Surgical Details a
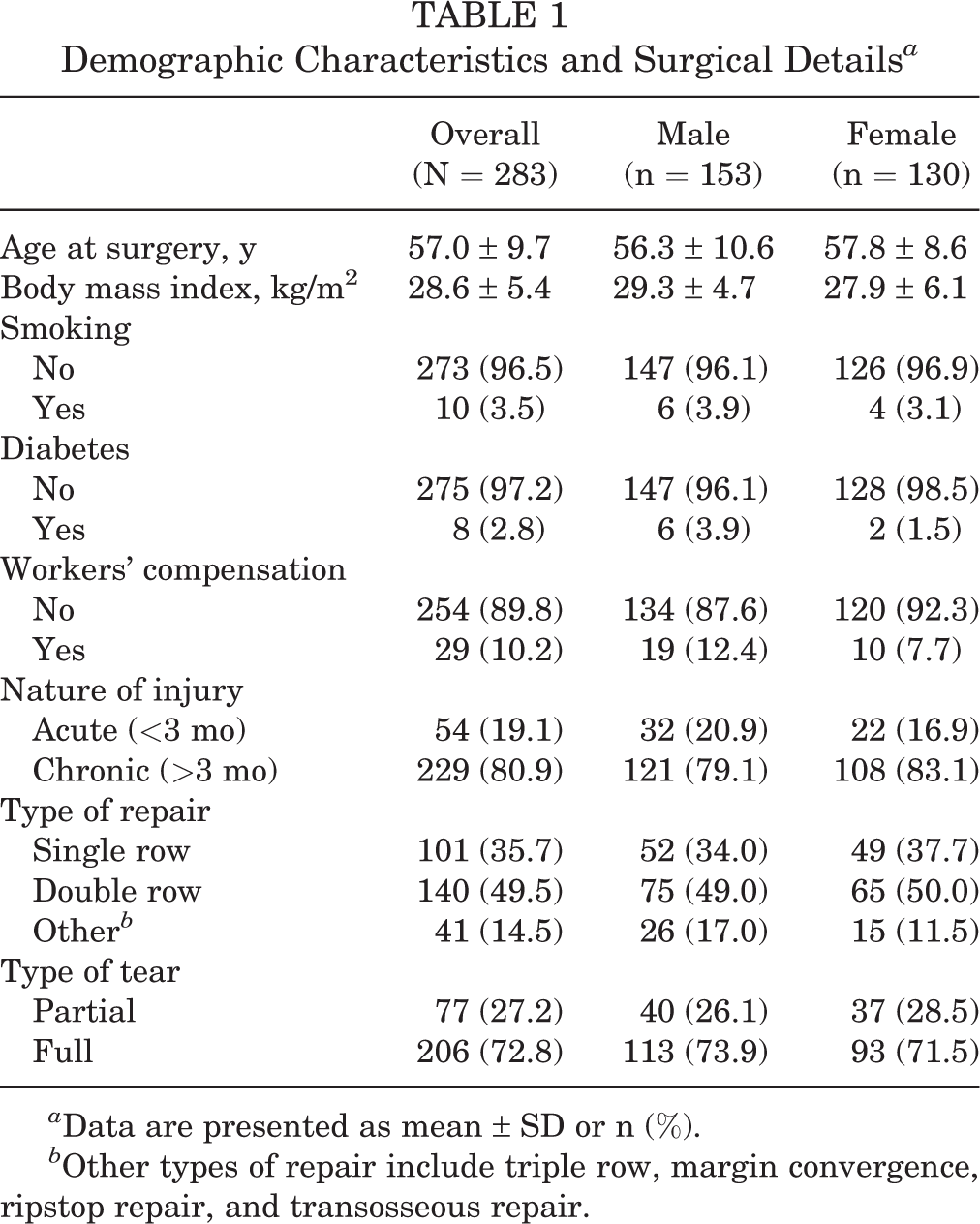
a Data are presented as mean ± SD or n (%).
b Other types of repair include triple row, margin convergence, ripstop repair, and transosseous repair.
There was a significant interaction between sex and time point for the pain VAS score, indicating an association between pain and time dependent on sex. Women reported significantly higher VAS pain scores at the preoperative (P = .0015), 2-week (P = .0086), 6-week (P = .0001), and 3-month (P = .0169) time points. No significant sex differences were found at 6-month and 1-year postoperative follow-up (P = .47 and .75, respectively) (Figure 1). However, women had a greater overall change in the VAS pain score from the preoperative to 6-month time points (P = .0094) and from the preoperative to 1-year time points (P = .0029).
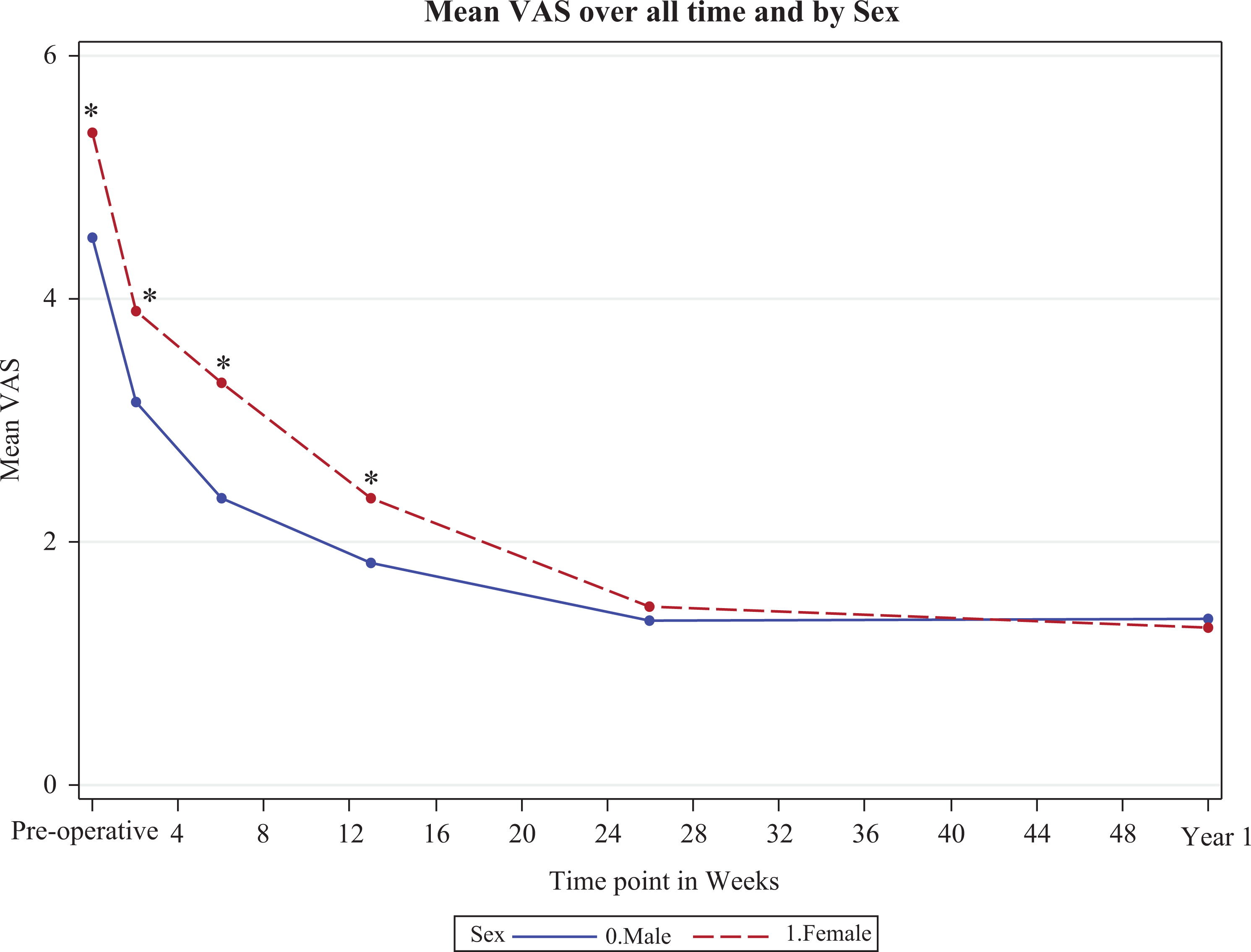
Mean visual analog scale (VAS) pain scores compared between sexes across all study time points (0 indicates preoperative time point). *Indicates significant differences between men and women.
Patient-reported shoulder function was measured with the ASES score, SANE, and VR-12 PCS. Significant sex differences, with women reporting decreased ASES scores, were noted at the preoperative (P < .0001) and 3-month (P = .0041) time points. No significant sex differences in the ASES score were found for the 6-month (P = .1403) or 1-year (P = .6819) postoperative time points (Figure 2). Women saw a greater change in the ASES score from the preoperative to 6-month (P = .0179) and 1-year (P = .0036) time points.

Mean American Shoulder and Elbow Surgeons (ASES) scores compared between sexes across all study time points (0 indicates preoperative time point). *Indicates significant differences between men and women.
The mean SANE score did not differ between men and women when controlling for time (P = .31). The mean SANE score did not significantly differ between the sexes at any time point (P > .05). SANE scores improved equally for both sexes from the preoperative to 1-year time points (P = .3517).
The VR-12 PCS showed significant sex differences when controlling for time point, with women reporting lower scores than men for all time points (P = .01). Women also reported lower VR-12 MCS scores preoperatively (P = .03); however, no sex difference was found at either the 6-month (P = .34) or 1-year (P = .36) postoperative follow-up. Women had a greater overall change in the VR-12 MCS score from preoperative to 1-year follow-up when compared with men (P < .0001).
In addition to significantly higher pain scores, women were also more likely to use narcotic pain medication 2 weeks postoperatively (P = .032). No significant differences were noted in nonnarcotic pain medication (P = .733) or sleeping medication (P = .062) use at 2 weeks (Table 2).
Medication Use at 2 Weeks After Surgery a

a Bolded P value indicates statistically significant sex-based difference (P < .05, chi-square test).
Intraoperative findings such as tear thickness or tear size did not significantly influence any outcomes at any time point. See the Appendix for additional figures showing all outcome measures stratified by sex and time.
Discussion
The primary focus of this study was to assess sex differences in patient-reported pain levels and self-reported functional outcomes after primary arthroscopic rotator cuff repair. We found that female patients reported higher VAS pain scores preoperatively and up to 3 months postoperatively. No significant sex differences were noted in patient-reported outcomes at the 6-month and 1-year time points. Women also experienced a greater absolute decrease in pain from the preoperative to 1-year time points, likely secondary to higher baseline scores.
Our results are similar to previously reported data from Cho et al, 6 who indicated that female patients reported higher VAS pain scores up to 2 weeks after surgery. The present study expands such findings, indicating that women may feel increased pain for up to 3 months after surgery when compared with men. While not examined in the present study, Cho et al 6 also indicated that female patients exhibited worse functional outcomes such as decreased forward flexion and external rotation up to the 6-week follow-up. In concordance with increased pain levels 2 weeks after surgery, we found that women were significantly more likely to be using narcotic pain medication at this time point. Recent emphasis has been placed on research that seeks to evaluate risk factors for prolonged postoperative narcotic use. 3,9 Our finding indicates that further research studies should evaluate sex as a possible risk factor for prolonged narcotic pain medication use in the acute postoperative period.
Increased interest has been placed on possible reasons for sex differences in pain levels. Bartley and Fillingim 2 examined differences in the perception and affective modulation of pain and hypothesized that psychosocial processes as well as gender roles may contribute to differences in pain expression, in addition to the possible modulatory role of sex hormones. Conversely, in a study that examined the affective modulation of spinal nociception and pain, Rhudy et al 27 found no differences between the sexes with regard to the affective modulation of nociceptive stimulation. Societal expectations and perceived gender stereotypes may also play a role, as one study found that pain in male and female patients is assessed and treated differently by independent observers. 34
Regarding self-reported functional outcomes, the results of the present study indicate that women reported decreased shoulder function as measured by the ASES score preoperatively and up to 3 months postoperatively. Our results are similar to previous data, with a study by Razmjou et al 26 indicating that female patients had decreased ASES, Western Ontario Rotator Cuff Index (WORC), and Disabilities of the Arm, Shoulder and Hand (QuickDASH) scores up to 6 months postoperatively. While our results indicated that male and female shoulder function converged at 6 months and 1 year, one previous study 28 with an average follow-up of 54 months indicated that there was a significant negative relationship between age and functional shoulder scores in women, which was not observed in a male cohort.
Among the health-related quality of life measures, the VR-12 MCS scores were significantly lower for women at the preoperative time point. However, no significant difference in the VR-12 MCS score was observed between the sexes at the 6-month and 1-year time points. While women experienced an overall greater improvement in the VR-12 MCS score, the lower preoperative score did not seem to predict any difference in functional recovery between men and women at final follow-up. Similarly, while we found the VR-12 PCS score to be significantly lower for women at all time points, this did not seem to influence a difference in functional or pain scores between the male and female groups at the 6-month or 1-year follow-up. Previous literature 4,5 has indicated that psychological factors such as patient expectations and other mental health indicators such as measures of self-efficacy may influence postoperative outcomes. A separate study by Cho et al 5 found that a history of diagnosed depression, anxiety, or insomnia was not predictive of VAS or ASES scores at 1 year after rotator cuff repair. In contrast, the same group found that self-reported depressive symptoms were independent predictors of postoperative functional disability and lower quality of life. 4
Although there is a paucity of literature that directly examines the effect of sex on outcomes after rotator cuff repair, other areas of orthopaedic surgery have closely evaluated differences in treatments and outcomes between men and women. Several studies have demonstrated that female patients have significantly worse preoperative functional outcome scores before total hip arthroplasty. 13,23 Mannion et al 20 evaluated pain and function 1 year after total hip arthroplasty and found that female patients had significantly lower baseline functional outcome scores. However, the authors noted no significant sex differences in outcome scores at 1-year follow-up. 20 Previous studies on elective orthopaedic surgery have hypothesized that preoperative scores in the female population are significantly lower because of gender roles or a higher pain tolerance. 17 Further research is necessary to assess sex differences in perceived pain and self-reported functional outcomes across all orthopaedic surgical procedures. Such research will add to the limited body of knowledge and aid in determining provider and patient expectations for postoperative recovery patterns.
Limitations
This study has several limitations. First, our length of follow-up was relatively limited, to 1 year from the date of surgery; however, we felt that it was long enough to assess preoperative and initial postoperative sex differences. Second, as a retrospective review of prospectively collected data, there exists the possibility of introducing confounding variables not accounted for in our subgroup analysis, which may have affected the overall outcome. All outcome scores were collected prospectively, so there should be minimal factors affecting the analysis. Third, despite our demonstrated difference between male and female patients, it is difficult from this study alone to determine if these differences are related to socioeconomic or physiological factors; therefore, further studies should be conducted in this area of research.
Conclusion
The present study indicated that women had increased pain and decreased self-reported function when compared with men for the first 3 months after primary arthroscopic rotator cuff repair. In concordance with increased pain, women were more likely to use narcotic pain medication 2 weeks after surgery. Such results contribute to the body of knowledge regarding sex differences in pain and functional outcomes after rotator cuff repair. In addition, the results inform provider expectations for postoperative recovery, and such information can be conveyed to patients when planning a rotator cuff repair procedure.
Footnotes
Notes
One or more of the authors declared the following potential conflict of interest or source of funding: L.D.H. is employed by Arthrex and has received educational support from Arthrex and hospitality payments from Arthrex and Ethicon. E.G.M. has received consulting fees from Smith & Nephew, educational support from Kairos Surgical, and hospitality payments from NuVasive. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethics approval for this study was obtained from the Partners Human Research Committee (protocol No. 2011P002663/PHS).