
Abstract
Background:
Microfracture offers a joint-preserving treatment for glenohumeral osteochondral defects, although its application to bipolar defects remains understudied, especially among an active-duty servicemember (ADSM) population.
Purpose:
To evaluate outcomes after microfracture of bipolar glenoid and humeral head lesions in ADSM aged <55 years.
Study Design:
Case series; Level of evidence, 4.
Methods:
ADSM aged <55 years were eligible for inclusion if they underwent microfracture for Outerbridge grade IV bipolar glenohumeral cartilage lesions identified on diagnostic arthroscopy at various locations within the joint and had >5 years of postoperative follow-up. All patients underwent concomitant arthroscopic subacromial debridement and other procedures that did not necessitate extended postoperative immobilization, while those with concomitant rotator cuff or labral repair were excluded. Outcomes included patient-reported outcome measures—specifically, pain on visual analog scale, Single Assessment Numeric Evaluation, and American Shoulder and Elbow Surgeons standardized assessment—and range of motion, return to duty, and arthroplasty-free survivorship.
Results:
In total, 31 patients were eligible for inclusion (mean ± SD age, 45.7 ± 8.1 years; male, 90.3%; mean follow-up, 8.0 ± 1.9 years). On average, glenoid and humeral head lesions measured 247 ± 155 and 201 ± 137 mm2, respectively. All patient-reported outcome measures demonstrated significant improvements postoperatively independent of lesional size (visual analog scale, 8.2 ± 1.8 to 1.7 ± 1.8; Single Assessment Numeric Evaluation, 51.0 ± 18.8 to 80.5 ± 14.9; American Shoulder and Elbow Surgeons, 47.0 ± 11.7 to 85.2 ± 12.5; P < .0001 for all). Internal rotation improved slightly (T10.5 ± 2.4 to T9.1 ± 2.5; P = .0109); otherwise, range of motion remained stable. At final follow-up, 71% (n = 22) returned to full duty and 65% (n = 20) to preinjury level of sport. Two patients (6.5%) experienced symptom progression and underwent total shoulder arthroplasty at 6 and 8 years postoperatively at ages 52 and 62 years, respectively.
Conclusion:
Microfracture of bipolar glenohumeral osteochondral lesions among ADSM yields significant improvements in pain and shoulder function; however, rates of return to unrestricted duty and former level of sport were limited, and 6.5% of patients ultimately underwent total shoulder arthroplasty 6 to 8 years postoperatively. While microfracture begets symptomatic relief for many young, active patients with bipolar osteochondral lesions and appears to offer several years of improved symptom management, return to full occupational and athletic function remains limited and warrants appropriate patient education and counseling.
Keywords
The incidence of glenohumeral osteochondral defects (OCDs) of the shoulder is reported at 5% to 17%, representing a relatively common shoulder pathology that often reflects a precursor of osteoarthritis or sequelae of shoulder instability.1,5 Bipolar cartilage lesions, which represent a subset of OCDs involving injury to the glenoid and humeral head articular cartilage, are less commonly observed and studied. 17 While the exact progression of bipolar articular cartilage lesions remains variable and incompletely understood, these lesions risk progression to symptomatic glenohumeral arthritis with a corresponding increase in shoulder pain and decrease in physical function and quality of life. 3
Although bipolar osteochondral lesions are more commonly observed among an older population that sustains a higher, time-dependent risk for cartilage degeneration, the presence of bipolar lesions among younger populations poses a unique challenge in management, especially among active-duty servicemembers (ADSM) whose occupations elicit high shoulder demand and greater rates of shoulder dysfunction as compared with their civilian counterparts.2,12,16 While total shoulder arthroplasty (TSA) remains the gold standard for the treatment of OCDs that have progressed to end-stage degenerative glenohumeral arthritis in the elderly, there are substantial risks and function-limiting restrictions associated with shoulder arthroplasty in younger patients. 11 For OCDs that have not progressed to end-stage degenerative joint disease, microfracture remains a viable option for joint preservation in treating isolated glenoid or humeral head OCDs4,5,14,21,23; however there remains a paucity of literature regarding the application of microfracture in managing bipolar osteochondral lesions.
The purpose of this study is to evaluate outcomes after microfracture of concomitant glenoid and humeral head lesions in active-duty military patients <55 years of age. We hypothesize that microfracture of bipolar lesions would produce significant improvement in patient-reported outcome measures (PROMs).
Methods
Study Design and Inclusion Criteria
In this retrospective analysis of prospectively collected data, ADSM <55 years of age were eligible for inclusion if they underwent arthroscopic debridement and microfracture of Outerbridge grade IV bipolar glenohumeral cartilage lesions between January 2012 and December 2019 at a single institution. All patients had at least 5 years of follow-up. To reduce the confounding effects of substantially different postoperative rehabilitation protocols with longer immobilization times, patients were excluded if they were indicated either for concomitant rotator cuff repair for a full-thickness rotator cuff tear or for labral repair. Patients remained eligible for inclusion if they underwent concomitant arthroscopic subacromial debridement (aSAD), biceps tenodesis or tenotomy, acromioclavicular joint resection, arthroscopic rotator interval release, or debridement of partial-thickness articular-sided supraspinatus tendon avulsions. Informed consent and institutional review board approval were obtained before initiation of this study.
Surgical Indications
Before operative management, all patients who were indicated for surgery had at least 3 months of nonsurgical therapies that failed, including nonsteroidal anti-inflammatory use, home exercise programs, supervised physical therapy, and activity modification. All patients who were indicated for shoulder arthroscopy and had Outerbridge grade IV bipolar osteochondral defects intraoperatively were eligible for inclusion in the present study.
Surgical Technique
Before surgery, all patients received a preoperative interscalene block and underwent general anesthesia. After positioning in the beach chair and before securing the extremity in a Spider hydraulic arm holder (Smith & Nephew), an examination under anesthesia was conducted to assess range of motion (ROM) and glenohumeral stability. Diagnostic arthroscopy was performed to identify all intra-articular pathology, including bipolar glenohumeral cartilage defects. After the concomitant pathology was addressed, the bipolar cartilage lesions were inspected, and any nonviable cartilage flaps were debrided with an arthroscopic shaver, ring curette, and arthroscopic biter. For well-contained lesions on the glenoid and humeral head, a ring curette was used to create stable vertical walls around the defect to help shield the neighboring cartilage from further biomechanical stress. 24 After the underlying calcified cartilage layer was debrided, ensuring that subchondral bone was not inadvertently violated, a microfracture awl was used to penetrate the subchondral bone to a depth of 4 mm with multiple perforations spaced approximately 3 to 4 mm apart. After completion of the microfracture, the fluid inflow was stopped to visually confirm appropriate extrusion of marrow elements into the prepared defect site. Figure 1 demonstrates the debridement, measuring, and microfracture of bipolar glenohumeral cartilage defects. The senior surgeon's (N.P.) technique did not change significantly throughout the study duration from 2012 to 2019.
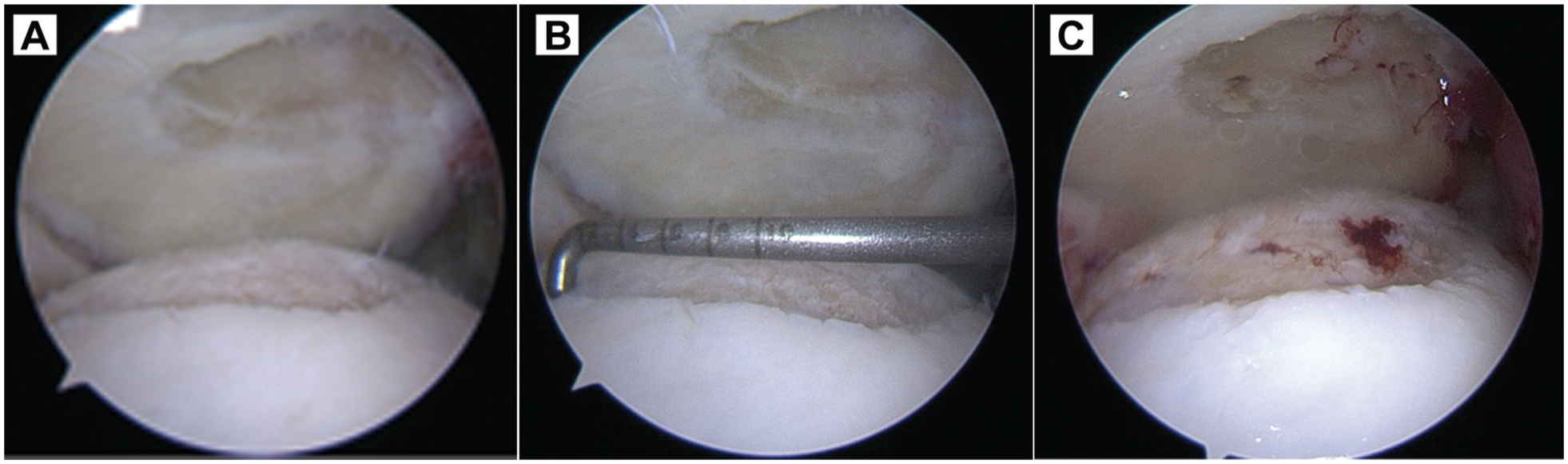
(A) Example of a debrided bipolar glenohumeral cartilage lesion. (B) Measurement of the bipolar glenohumeral cartilage lesion. (C) Microfracture of the bipolar glenohumeral cartilage lesion.
Postoperative Rehabilitation
All patients were discharged from same-day surgery with a multimodal pain regimen and a sling for comfort for the first 2 to 4 weeks postoperatively. Patients were instructed to begin gentle pendulum exercises once the interscalene nerve block had completely resolved. The physical therapy protocol was selected according to the most intensive concomitant procedure; however, all patients who underwent concomitant rotator cuff repair and labral repair were excluded, so no patients required prolonged sling immobilization. For patients who underwent isolated microfracture of bipolar glenohumeral osteochondral lesions, passive ROM was encouraged immediately after surgery with progression to active-assisted ROM and active ROM based on physical therapy performance and evaluation. Once patients demonstrated restored ROM, strengthening was initiated at a minimum 6 weeks postoperatively and progressed to full activity without restrictions at 12 weeks postoperatively. Patients received a profile limiting participation in military duty and excluding them from the Army Combat Fitness Test for the first 12 weeks postoperatively. At 16 weeks postoperatively, patients were permitted by the surgical team to return to full duty without restrictions once cleared by physical therapy.
Data Collection
Preoperatively, patient demographics and PROMs were collected for comparison with postoperative values. Intraoperatively, the sizes of the glenoid and humeral head components of bipolar lesions were measured by a standardized, graduated probe. Other intra-articular findings and concomitant relevant procedures were collected. Postoperatively, PROMs, ROM, rates of return to preinjury level of work and sport, and survivorship were collected and analyzed. Return to full, unrestricted active duty was defined as returning to the patients’ original military occupational specialty without duty restrictions or medical limitations. Similarly, return to preinjury level of sport was defined as the subjective self-assessment of return to former level of play by each patient.
PROMs included pain on visual analog pain (VAS), Single Assessment Numeric Evaluation (SANE), and American Shoulder and Elbow Surgeons (ASES) standardized assessment. ROM was measured by the senior surgeon for forward flexion and external rotation with a goniometer, while internal rotation was measured to the highest spinal level that the patient could reach with his or her hands. Failure of survivorship was defined as progression to TSA within the 5-year follow-up period.
Statistical Analysis
Statistical analysis was performed in SPSS Statistics Version 25.0 (IBM Corp) and RStudio Version 4.4.1 (R Foundation for Statistical Computing). Continuous data were described by a combination of mean, standard deviation, range, and 95% confidence intervals. Paired t tests were used to evaluate the differences between the pre- and postoperative PROMs and ROM. Chi-square and Fisher tests were used to evaluate differences between categorical variables. Multiple linear regression was used to identify the relationship between (1) lesion size and concomitant procedures and (2) PROM variables. A distribution-based minimal clinically important difference (MCID) was approximated for VAS, SANE, and ASES scores via the 0.5–standard deviation method: MCID = 0.5 × (SD of Δ score). Survivorship data were used to formulate a Kaplan-Meier curve and associated risk table. Statistical significance was set at P < .05.
Results
Between 2012 and 2019, 42 patients with Outerbridge grade IV bipolar cartilage lesions underwent simultaneous glenoid and humeral head microfracture. Of these, 8 patients underwent concomitant rotator cuff repair or labral repair and were subsequently excluded owing to prolonged immobilization in rehabilitative protocols; 2 patients were lost to follow-up; and 1 patient died 3 years postoperatively from causes unrelated to surgery. Ultimately, 31 patients were eligible for inclusion (Figure 2).

STROBE flow diagram.
Patient Demographics and Perioperative Findings
On average, patients were 45.7 ± 8.1 years of age and 90.3% were male (n = 28) (Table 1). Slightly more than half of injuries (n = 16; 51.6%) involved the dominant extremity, while slightly under half (n = 14; 45.2%) involved the right upper extremity. A majority (67.7%; n = 21) of patients had combat arms military occupational specialties. As measured intraoperatively, the mean size of the glenoid cartilage lesion was 247 ± 155 mm2 (range, 49-500) while that of the humeral head cartilage defect was 201 ± 137 mm2 (range, 35-450). Concomitant procedures are presented in Table 1. Mean follow-up was 8.0 ± 1.9 years (range, 5.2-12). All patients underwent aSAD (n = 31; 100%) while slightly over half underwent biceps tenodesis or tenotomy (n = 16; 51.6%). In total, 5 patients (16.1%) had only aSAD as a concomitant procedure. There were no postoperative complications to include infection or nerve injury.
Patient Demographics, Lesion Characteristics, and Concomitant Procedures (N = 31) a
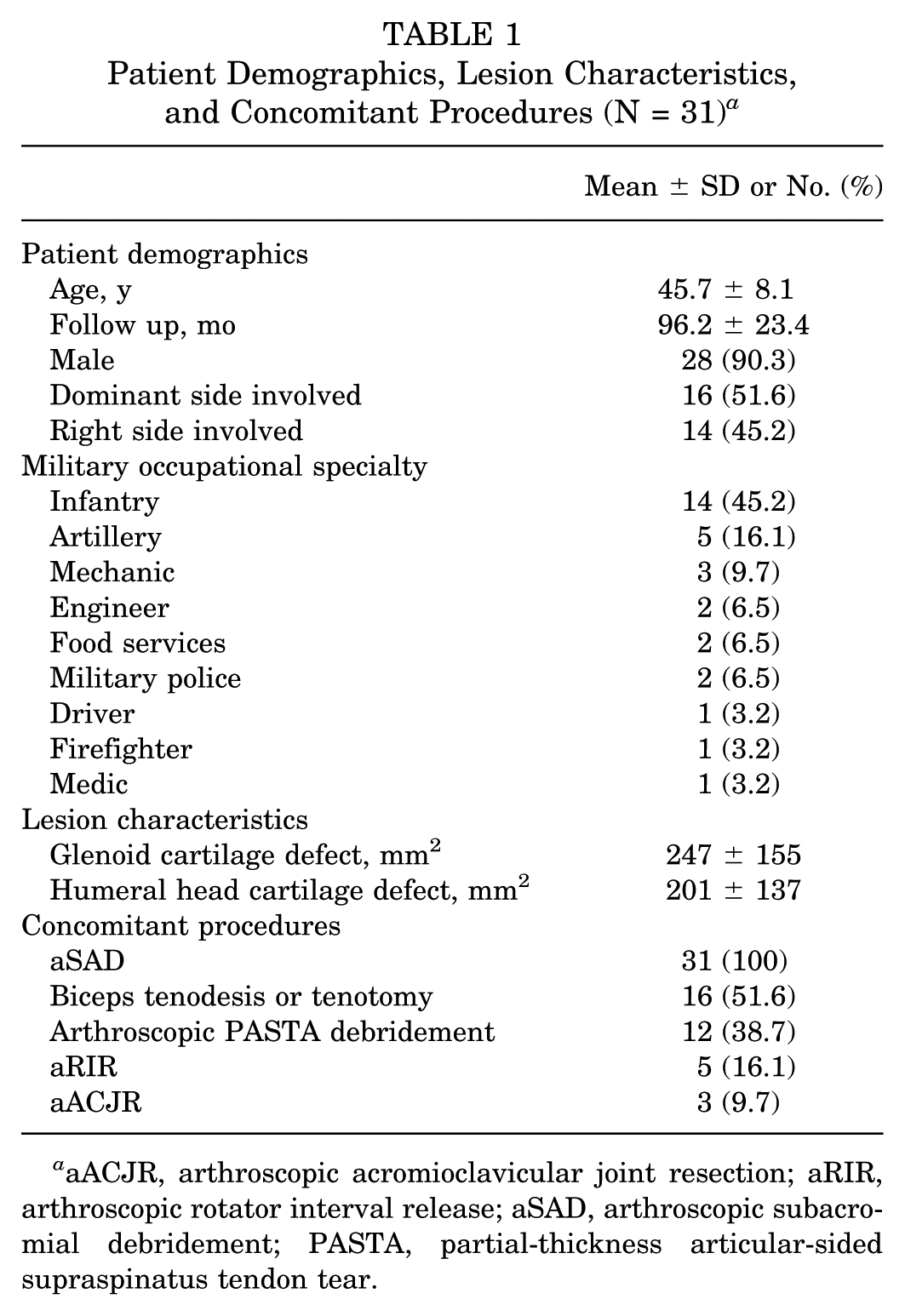
aACJR, arthroscopic acromioclavicular joint resection; aRIR, arthroscopic rotator interval release; aSAD, arthroscopic subacromial debridement; PASTA, partial-thickness articular-sided supraspinatus tendon tear.
Patient-Reported Outcome Measures
Statistically significant improvements were observed among all PROMs at final follow-up (Table 2). All patients (N = 31) demonstrated VAS improvements over the MCID threshold, while 77.4% (n = 24) and 96.8% (n = 30) demonstrated improvements over the SANE and ASES thresholds (Table 3). Three patients had 10-point decreases in SANE scores; however, all 3 showed improvements in VAS and ASES scores (+8 and +30; +3 and +12; +7 and +32). On multivariate regression, glenoid and humeral head lesion size were not associated with postoperative VAS (R2 = 0.084; F2,28 = 0.099; P = .906), SANE (R2 = 0.020; F2,28 = 0.290; P = .750), and ASES (R2 = 0.002; F2,28 = 0.027; P = .973). Similarly, the presence of individual concomitant procedures was not associated with final PROM outcomes: VAS (R2 = 0.05767; F4,26 = 0.3978; P = .8084), SANE (R2 = 0.02644; F4,26 = 0.1765; P = .9485), and ASES (R2 = 0.04682; F4,26 = 0.3193; P = .8625).
Patient-Reported Outcome Measure Scores (N = 31) a

Data presented as mean ± SD. Bold denotes statistical significance. Patients with survivorship include those who did not progress to total shoulder arthroplasty, while all patients include those who underwent total shoulder arthroplasty. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Distribution-Based MCID Thresholds (N = 31) a

The 0.5–standard deviation method was used to calculate the distribution-based MCID threshold: MCID = 0.5 × (SD of Δ score). ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Range of Motion
There was no statistically significant difference between pre- or postoperative forward flexion and external rotation, although there was a statistically significant improvement in internal rotation by about 1 vertebral level (Table 4).
Range of Motion (N = 31) a

Data presented as Mean ± SD. Bold denotes statistical significance. ER, external rotation; FF, forward flexion; IR, spinal level.
Return to Duty and Sport
At final follow-up, 71% (n = 22) of patients had returned to full, unrestricted active-duty military service, and 65% (n = 20) were able to return to preinjury level of sport activity. The patients who did not return to full, unrestricted active duty were medically discharged.
Survivorship
Two patients (6.5%) experienced symptom progression and were indicated for TSA. One patient underwent TSA 6 years postoperatively at the age of 52 years while another underwent TSA 8 years postoperatively at the age of 62 years (Figure 3). Of the patients who ultimately underwent TSA, 1 had improvement in VAS from 7 to 5, SANE from 20 to 50, and ASES from 46 to 62, while the other showed improvement in VAS from 7 to 2, SANE from 50 to 75, and ASES from 52 to 84.

Kaplan-Meier survivorship curve and risk table. Gray shading indicates 95% CI.
Discussion
In the present cohort of 31 ADSM with bipolar osteochondral defects of the glenoid and the humeral head, simultaneous microfracture of the glenoid and humeral head lesions was associated with significant reductions in pain and improvements in shoulder function at 5-year follow-up; however, 29% of patients were not able to return to full active duty and 35% were not able to return to preinjury level of sport activity. Ultimately, 2 patients (6.5%) experienced symptomatic progression and were indicated for shoulder arthroplasty at 6 and 8 years postoperatively. Based on these results, microfracture appears to offer a reasonable, joint-preserving option for symptomatic improvement among active, younger patients with bipolar osteochondral lesions of the glenohumeral joint where surgical options such as TSA, hemiarthroplasty, or ream-and-run arthroplasty may be limited by occupational requirements and duty status. Patients should be counseled on the risk of occupational and sport limitations associated with these lesions as well as the temporizing nature of microfracture on symptom control, with a 6- to 8-year duration of symptom control observed in the present study among patients who progressed to shoulder arthroplasty.
At the present time, there is a paucity of literature discussing bipolar glenohumeral osteochondral defects among active patients. Unlike in the knee, where articular cartilage defects are historically well researched, likely owing to the deleterious effects of shearing forces on a weightbearing joint and subsequent widespread prevalence, 18 the exact incidence of symptomatic bipolar glenohumeral OCDs is not precisely known. Considering our clinical experience, we suspect that risk factors identified for cartilage injury of the knee among ADSM—including older patient age, patients undergoing their first 6 months of training, and enlisted personnel—can similarly be extrapolated to risk factors for cartilage injuries of the shoulder. Unlike in the knee, where microfracture is associated with high rates of treatment failure beyond 5 years of follow-up, 6 the relative success of microfracture for cartilage lesions in the shoulder may be attributable to the lack of weightbearing demands on the shoulder joint. Additionally, the existing literature has discussed (1) the deleterious effects of glenoid cartilage lesions on return-to-duty rates among ADSM, often attributed to high-shoulder occupational demand and limited ability to modify activities in the occupational setting, and (2) the role of cartilage pathology as the rate-limiting step in achieving return to duty when performed concomitantly with other procedures; however, bipolar lesions were excluded from these assessments.7,20,21
Glenohumeral chondral defects among younger patient populations remain a challenging condition to manage. While arthroplasty may be a reasonable option for elderly or low-demand patients, only 41.7% of patients remain on active duty at 2 years, and only 20.8% were subsequently deployed after anatomic TSA, suggesting that postoperative restrictions are often incompatible with the occupational requirements of an ADSM population, especially those within combat arms specialties that require significant use of the shoulder for warfighting tasks. 11 Moreover, with younger age comes an increased risk for earlier revision surgery, as investigated by Kusnezov et al 11 who found that 46.2% of ADSM who underwent anatomic shoulder arthroplasty sustained complications within a 41-month period, with 23.1% requiring reoperation.
Given the postoperative limitations and high revision rates associated with shoulder arthroplasty in young patient populations whose nonsurgical management for isolated glenoid or humeral head osteochondral lesions fails, microfracture is increasingly recognized as an attractive, joint-preserving surgical option, especially when used to address smaller, isolated humeral head lesions.8,9,19,21-23 Despite the success of microfracture in treating unipolar lesions, however, there remains a discrepancy in achieving equally efficacious postoperative outcomes in the treatment of bipolar lesions.4,10,13 In a study of 16 patients with a mean age of 51 years, Frank et al 4 demonstrated an approximately 10-point discrepancy in postoperative Constant and Subjective Shoulder Value scores among patients with bipolar lesions as compared with their unipolar counterparts, although the differences did not reach statistical significance (P = .070 and .065, respectively). Among the 6 patients with bipolar lesions included in the study by Millett et al, 14 2 patients aged 45 and 50 years ultimately underwent shoulder arthroplasty (30%), while only 1 of the 25 patients with unipolar lesions aged 52 years went on to shoulder arthroplasty (4%). In a study of 13 patients with a mean age of 36 years who underwent microfracture for unipolar or bipolar glenohumeral lesions with a mean 10.2 years of follow-up, Wang et al 23 reported a 33%-42% rate of clinical failure and a 21% rate of conversion to shoulder arthroplasty. In the present study, with a mean age of 46 years and 8.0 years of follow-up, rates of progression to shoulder arthroplasty are much lower at 6.5%. The dissimilarity in rates of progression to shoulder arthroplasty despite an older cohort may reflect reticence for ADSM to progress to shoulder arthroplasty given their high occupational shoulder demands; yet, the present study and that by Wang et al demonstrate significant improvements in shoulder pain and function for patients who did not eventually undergo arthroplasty. Ultimately, though, the exact impact of these lesions on shoulder function remains largely unknown; in the present study, for example, all patients were indicated for diagnostic arthroscopy because of persistent shoulder pain unresolved with nonsurgical measures rather than glenohumeral osteochondral lesions specifically, and there was no comparative observation cohort that did not undergo microfracture. Similar to how comprehensive arthroscopic management of early glenohumeral osteoarthritis has the potential to improve PROMs among young and active patients, 15 the concomitant procedures present in this study may similarly explain the improvements in PROMs observed among these patient populations rather than direct improvement from microfracture. Regardless, much of the existing literature surrounding microfracture remains low-volume and not specific to microfracture of bipolar lesions.
Specific to ADSM, Scanaliato et al 21 demonstrated a return-to-duty rate of 65% and a survivorship rate of 75% at 5-year follow-up after using microfracture for glenoid lesions in isolation. Of the 5 patients who required secondary surgery in their study, 4 underwent comprehensive arthroscopic management and 1 underwent shoulder arthroplasty. Two other patients did not proceed to secondary surgery within the 5 years of follow-up but similarly did not return to active duty. While a slightly greater proportion of patients in the present study of bipolar lesional microfracture ultimately underwent shoulder arthroplasty (6.5% vs 5.0%), a slightly greater proportion of patients were eventually able to return to duty after microfracture of the bipolar lesions (71% vs 65%). The similarities between these findings suggest that glenohumeral cartilage lesions yield similar symptomatic incidences of shoulder pain and dysfunction irrelevant of whether the lesions involve the glenoid in isolation or the glenoid and the humeral head. For ADSM with either unipolar glenoid or bipolar glenohumeral cartilage lesions, microfracture appears to offer improved symptomatic control and shoulder function; however, patients should be thoroughly counseled on the risks of treatment failure and the potential occupational limitations that this pathology imbues.
Limitations
This study is not without limitations. The small sample size and study cohort of predominantely male ADSM limit overall generalizability to a broader population. While excluding patients undergoing concomitant rotator cuff and labral repair minimizes the confounding effects of extended postoperative immobilization, patients with cartilage lesions secondary to shoulder instability were subsequently excluded from this study. Other confounding variables in the present study include (1) indications for shoulder arthroscopy beyond the presence of bipolar glenohumeral cartilage lesions, prompting concomitant procedures such as aSAD, acromioclavicular joint resection, arthroscopic rotator interval release, and partial-thickness articular-sided supraspinatus tendon avulsion debridement, without stratification to isolate the effects of concomitant procedures on PROM results, and (2) variations in osteochondral lesion size, location within the glenohumeral joint, containment, and congruence. Furthermore, the absence of a control group reporting outcomes for untreated lesions renders drawing conclusions regarding microfracture vs observation and the impact of microfracture vs concomitant procedures unattainable from the present study's design. Additionally, PROM threshold values for MCID, substantial clinical benefit, and Patient Acceptable Symptom State after microfracture of glenohumeral osteochondral lesions are not identified, so PROM threshold analysis was limited to distribution-based MCID. Finally, this study did not evaluate radiographic progression to arthritis given that radiographs were not routinely obtained for patients postoperatively unless clinically indicated, limiting evaluation of progression of osteoarthritis over time and comparison of the progression of arthritis as early-onset vs traumatic.
Conclusion
Microfracture of bipolar glenohumeral osteochondral lesions among ADSM yields significant improvements in pain and shoulder function; however, rates of return to unrestricted duty and former level of sport were limited, and 6.5% of patients ultimately underwent TSA 6 to 8 years postoperatively. While microfracture begets symptomatic relief for many young, active patients with bipolar osteochondral lesions and appears to offer several years of improved symptom management among patients whose lesions progress beyond the threshold of joint preservation, return to full occupational and athletic function remains limited and warrants appropriate patient education and counseling.
Footnotes
Final revision submitted October 12, 2025; accepted October 14, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.H. has received travel and lodging fees from Pinnacle, Inc. I.R. has received travel and lodging fees from Smith and Nephew, Inc and Legacy Ortho, LLC. A.R. has received consulting and travel and lodging fees from Stryker Corporation. N.P. has received consulting fees from Mitek.
Ethical approval for this study was obtained from Carthage Area Hospital (IRB: 2024-0005).