
Abstract
Background:
The postoperative influence of medial patellofemoral ligament reconstruction (MPFLR)—performed alone or in conjunction with tibial tubercle osteotomy (MPFLR+TTO)—on patellar height is not well-understood.
Purpose/Hypothesis:
The purpose was to compare longitudinal changes in patellar height after MPFLR and MPFLR+TTO. It was hypothesized that knees undergoing MPFLR will experience a decrease in patellar height that is greater than that of knees undergoing MPFLR +TTO and that both cohorts will return to Caton-Deschamps index (CDI) measures near that of preoperative levels.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This is a retrospective radiographic review of skeletally mature patients >15 years of age who underwent either an MPFLR or an MPFLR+TTO with lateral knee radiographs available from the preoperative period, 0 to 6 months (early) postoperatively, and >6 months (final) postoperatively. Exclusion criteria were (1) distalization TTO and (2) previous procedures, or procedures postoperatively near the extensor mechanism. CDI was used to quantify patellar height. Paired Student t tests and a repeated-measures analysis of variance was performed to evaluate the effect of CDI changes between MPFLR and MPFLR+TTO.
Results:
A total of 62 knees in 61 patients (55% female [34/62 knees]) were included, with n = 27 knees undergoing MPFLR and n = 35 knees with MPFLR+TTO. Mean age was 25.9 ± 9.8 years (range, 15-58 years). Mean time from surgery to early postoperative imaging was 1.9 ± 1.4 months with MPFLR and 2.4 ± 0.8 months with MPFLR+TTO (P = .08). Mean time from surgery to final follow-up imaging was 26.3 ± 24.6 months with MPFLR and 23.4 ± 17.8 months with MPFLR+TTO (P = .59). Preoperative mean CDI values were comparable between the MPFLR and MPFLR+TTO (1.15 ± 0.20 vs 1.18 ± 0.13; P = .13). At early follow-up (0-6 months postoperatively), mean CDI values with MPFLR decreased to 1.01 ± 0.18, compared with MPFLR+TTO at 1.11 ± 0.15 (P = .003). At final follow-up (>1 year postoperatively), the CDI values were similar between MPFLR (1.13 ± 0.21) and MPFLR+TTO (1.13 ± 0.14) (P = .79).
Conclusion:
Our study showed that MPFLR both with and without TTO demonstrated an eventual return toward preoperative patellar height, yet they followed different early postoperative trajectories. MPFLR demonstrated an early decrease in patellar height that progressively relengthened over time, whereas MPFLR+TTO exhibited almost no changes in patellar height.
Keywords
Patellar instability is a common musculoskeletal condition characterized by recurrent lateral patellar dislocations resulting from soft tissue abnormalities, limb malalignment, or bony deformities. 17 The etiology of patellar instability is multifactorial, often involving medial patellofemoral ligament (MPFL) dysfunction, trochlear dysplasia, patella alta, and an increased tibial tubercle–trochlear groove (TT-TG) distance, among others.4,13,17 Left untreated, patellar instability has been associated with substantial long-term sequelae including significant functional impairment, compromised patellofemoral biomechanics, and an increased risk of patellofemoral osteoarthritis. 3
One of the primary contributors to patellar instability is patella alta, defined as a superiorly positioned patella relative to the tibiofemoral joint, which significantly alters the anisometry of the medial patellofemoral complex attachment points and patellar tracking.1,15 First-line treatment for patellar instability is typically nonoperative management (physical therapy and bracing).14,16,17 Commonly, patients require surgical management because of recurrent instability and dislocation. MPFL reconstruction (MPFLR) is commonly employed in cases of recurrent patellar instability, however, in cases with significant bony abnormalities affecting patellar station, additional surgical procedures such as TT osteotomy (TTO) can be indicated to optimize patellar tracking.1,3,7,11,12
Previous research has demonstrated reductions in patellar height and tendon length after TTO procedures with and without MPFLR, and likewise with isolated MPFLR.8,10,18 Recently, a study by Yang et al. demonstrated that patients with patella alta and recurrent dislocations demonstrate decreased patellar height at 6-month follow-up. 18 However, the temporal evolution of patellar height in the immediate, early (0-6 months), and long-term (>1 year) postoperative periods remains poorly understood when comparing isolated MPFLR versus MPFLR plus TTO (MPFLR+TTO). Therefore, using the Caton-Deschamps index (CDI) as the primary metric, the purpose of the study is to characterize the dynamic trajectory of patellar height over these distinct postoperative intervals. We hypothesize that knees undergoing MPFLR will experience a decrease in patellar height that is greater than that of knees undergoing MPFLR +TTO and that both cohorts will return to CDI measures near that of preoperative levels.
Methods
Cohort Selection
Following institutional review board approval, all skeletally mature patients >15 years of age who underwent MPFLR between May 27, 2014, and June 15, 2023, were pulled from an institutional electronic data warehouse and reviewed in the electronic medical record software (Epic Systems). Note was made if a TTO was performed. Patient charts were then reviewed to ensure the availability of lateral knee radiographs from 0 to 6 months (early) and >1 year (final) postoperatively. Exclusion criteria were (1) patients with no imaging at the preoperative, early postoperative, or final time points, (2) skeletally immature patients as identified on imaging, (3) those that underwent distalizing TTO, and (4) individuals undergoing a revision procedure. The CDI was calculated by 2 independent measurers (A.S. and M.G.) for preoperative, early postoperative, and final postoperative radiographs by the methodology commonly utilized in the literature. 2 Patella alta knees were defined as a CDI of >1.30 (Figure 1). 2 A TTO procedure was performed in conjunction with MPFLR when excessive lateralization of the TT or clinically significant patellofemoral maltracking was present.
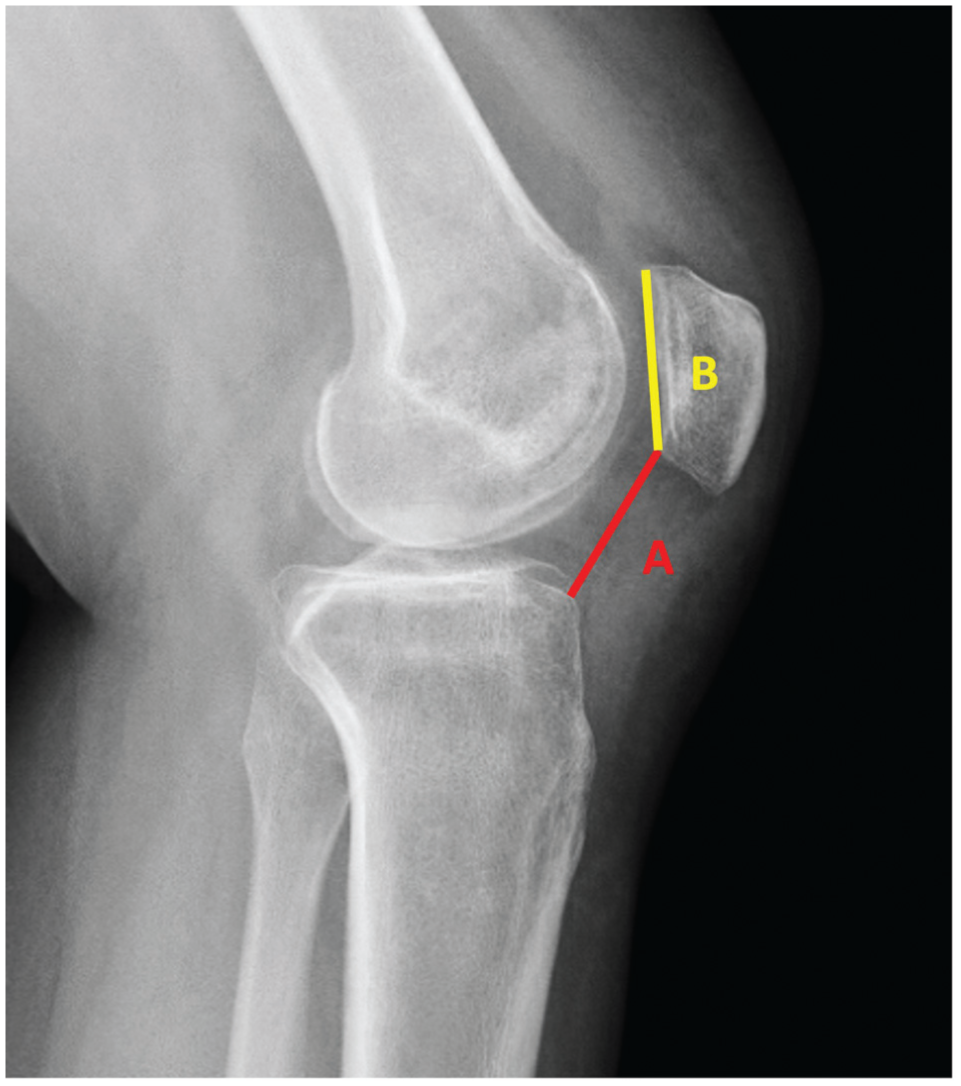
The Caton-Deschamps index (A/B) is defined as the ratio of (A) the length of the articular surface, and (B) the distance from the inferior edge of the patellar articular surface to the anterior superior edge of the tibial plateau. 2
Statistical Analysis
Intraclass correlation coefficient (ICC) was used to determine interrater reliability for all CDI measurements for preoperative and postoperative radiographs. Based on the 95% CI of the ICC estimate, values <0.50, between 0.5 and 0.75, between 0.76 and 0.9, and >0.90 were considered to have poor, moderate, good, and excellent reliability, respectively.
All analyses were performed using SPSS Version 27 (IBM Corp). For between-group comparisons, independent Student t tests were used to compare CDI between MPFLR and MPFLR+TTO groups at each time point (preoperative, early postoperative, and final postoperative). Within-group comparisons of CDI across time points were assessed using paired t tests, with the Bonferroni-Holm method applied to adjust for multiple comparisons.
To evaluate the overall effect of procedure type and time on CDI, a repeated-measures analysis of variance (ANOVA) was conducted. Procedure type (MPFLR vs MPFLR+TTO) was treated as the between-patient factor, and time (preoperative, early postoperative, final postoperative) as the within-patient factor. Mauchly test for sphericity was performed to assess the assumption of sphericity, and when this assumption was violated, Greenhouse-Geisser corrections were applied to adjust degrees of freedom.
To further investigate the nature of CDI changes over time, trend analysis was conducted to assess linear and quadratic patterns. A quadratic trend was analyzed to determine the nonlinear trajectory of CDI changes over time. Additionally, a time × surgery interaction was assessed to evaluate whether the CDI trajectory differed between the MPFLR and MPFLR+TTO groups. Post hoc analyses were conducted to interpret these differences, with adjustments for multiple comparisons where applicable. Statistical significance was set at P < .05.
Results
A total of 435 knees were identified. Of this total, 311 knees did not have radiographs available within the specified time frames, 22 knees were skeletally immature, 21 underwent a distalizing procedure, and 19 knees underwent a revision procedure. Ultimately, 62 knees, in 61 total patients, met the inclusion criteria.
Among those included, 27 underwent isolated MPFLR, and 35 underwent MPFLR+TTO. Preoperatively, patella alta (CDI >1.3) was present in 8 (30%) of MPFLR knees and 4 (11%) of MPFLR+TTO knees. The mean age was 24.65 ± 9.8 years in the MPFLR group and 27.2 ± 9.8 years in the MPFLR+TTO group (P = .11). Females accounted for 17 (63%) of the MPFLR group and 17 (49%) of the MPFLR+TTO group (P = .44). The mean body mass index (BMI) was 27.2 ± 9.8 in the MPFLR group and 27.6 ± 7.0 in the MPFLR+TTO group (P = .85). There were no significant between-group differences in age, sex distribution, or BMI (Table 1). Single-score ICC for the data was “excellent” at 0.91, indicating strong interrater agreement.
Demographics and Surgical Timing Data a

Data are presented as mean ± SD or n (%). Bolded P-values indicate statistical signifiance as defined by those <0.05. Independent Student t tests were used to compare means of continuous variables. Chi-square analysis was used to compare sex distribution. The MPFLR group was found to be significantly lower at the early postoperative period when compared with MPFLR+TTO, at a significance level of .05. BMI, body mass index; CDI, Caton-Deschamps index; MPFLR, medial patellofemoral ligament reconstruction; postop, postoperative; preop, preoperative; TTO, tibial tubercle osteotomy.
The interval between surgery and early postoperative imaging did not differ significantly between MPFLR (1.9 ± 1.4 months) and MPFLR+TTO (2.4 ± 0.8 months) (P = .08). Likewise, the interval between surgery and long-term follow-up imaging was comparable between the 2 groups (26.3 ± 24.6 vs 23.4 ± 17.8 months, respectively; P = .59). Preoperative CDI values were similar (1.15 ± 0.20 vs 1.18 ± 0.13; P = .13). At early follow-up, the MPFLR group had a significantly lower CDI (1.01 ± 0.18) than the MPFLR+TTO group (1.11 ± 0.15) (P = .003). However, by final follow-up at >1 year postoperatively, CDI values no longer differed significantly between the 2 groups (1.13 ± 0.21 vs 1.13 ± 0.14; P = .79).
Within-group paired t test analyses demonstrated that at early postoperative follow-up, the MPFLR group exhibited a significant decrease in CDI compared with preoperative values (1.15 ± 0.20 vs 1.01 ± 0.18; P < .001), whereas the MPFLR+TTO group demonstrated a smaller, nonsignificant decrease (1.18 ± 0.13 vs 1.11 ± 0.15; P = .07) (Table 2). By final follow-up, CDI values in both groups had returned toward their preoperative levels, with no significant difference between them (MPFLR: 1.13 ± 0.21, P = .53; MPFLR+TTO: 1.13 ± 0.14, P = .16, respectively). Within-group comparisons across time points revealed a significant increase in CDI from early to final follow-up in the MPFLR cohort (P < .001), suggesting that isolated MPFLR initially decreases patellar height, followed by a progressive relengthening over time. In contrast, MPFLR+TTO maintained a more stable CDI trajectory, with no statistically significant changes between time points.
Mean Patellar Height at Different Time Points of MPFLR and MPFLR+TTO Cohorts a

Data are presented as mean ± SD. Bold P values indicate statistical significance at P < .05. Paired t tests were used to compare Caton-Deschamps index values between consecutive time points (preoperative to early postoperative, early to final postoperative, and preoperative to final postoperative). MPFLR, medial patellofemoral ligament reconstruction; TTO, tibial tubercle osteotomy; Postop, postoperative; Preop, preoperative.
A repeated-measures ANOVA revealed a significant effect of time on CDI (F[1.71, 102.59] = 12.78; P < .001) and a significant time × surgery interaction (F[1.71, 102.59] = 3.43; P = .04), indicating different patterns of CDI change for MPFLR versus MPFLR+TTO. Because Mauchly test indicated violation of sphericity (P < .001), Greenhouse-Geisser corrections were applied. Trend analysis showed a significant quadratic pattern over time (F[1, 60] = 20.33; P < .001) and a significant quadratic time × surgery interaction (F[1, 60] = 5.58; P = .02), underscoring a nonlinear trajectory of CDI with distinct curves for each surgical group. These findings indicate that CDI changes followed a distinct pattern over time, with MPFLR+TTO patients demonstrating a different recovery profile compared with MPFLR-alone patients (Figure 2).

Caton-Deschamps index (CDI) values measured preoperatively, at early postoperative (0-6 months), and at final postoperative (>1 year) time points after isolated medial patellofemoral ligament reconstruction (MPFLR) compared with MPFLR combined with tibial tubercle osteotomy (MPFLR+TTO). The MPFLR cohort demonstrated a significant initial decrease in patellar height followed by a return toward preoperative levels, whereas the MPFLR+TTO group exhibited more stable CDI values across all measured intervals. Statistical significance was determined using paired t tests and repeated-measures analysis of variance (P < .05).
Discussion
The major findings of our study showed that both surgical approaches ultimately returned patellar height to near-baseline values by final follow-up, albeit via different trajectories. Specifically, the MPFLR group's patellar height decreased significantly from a preoperative CDI of 1.15 to 1.01 at the early assessment (P < .001), before significantly increasing again to 1.13 by the final follow-up (P < .001). In contrast, the MPFLR+TTO group showed no significant changes in patellar height between any time points, remaining stable from preoperative (1.18) to final follow-up (1.13) assessments. By final follow-up, CDI values were similar between the 2 groups, indicating that both interventions achieved restoration of patellar height in the long term.
The present study’s findings build upon existing work by McNamara et al, 10 who observed a decrease in patellar height at a mean of 18 months postoperatively among patients undergoing TTO (medialization or anteromedialization) with or without MPFLR. Because MPFLR was performed in the vast majority (91.9%) of their cases, it remained unclear whether this ligamentous procedure or the osteotomy component was the primary driver of the observed decrease in patellar height. In contrast, the present study’s direct comparison between isolated MPFLR and MPFLR+TTO offers clarity on that point: our data suggest that the MPFLR component itself may be a significant contributor to the early decrease in patellar height. While neither group’s patellar height changed substantially between the preoperative and final postoperative time points, the MPFLR group exhibited a marked reduction during the early postoperative period, highlighting a key divergence in recovery trajectories. This early decrease in CDI may reflect the initial soft tissue remodeling and tensioning that occur after MPFLR, whereas TTO appears to mitigate or stabilize any early fluctuation in patellar height. Ultimately, however, both surgical approaches were associated with patellar height returning to near-baseline values by final follow-up, underscoring the potential for dynamic rebalancing of the extensor mechanism over time.
Our study’s findings on the temporal evolution of patellar height both complement and refine the existing literature, particularly the work by Luceri et al, 9 which reported a significant and sustained decrease in patellar height at a mean of 18.4 months after isolated MPFLR. While our results were initially consistent, showing a similar decrease in patellar height in the early postoperative period, the key distinction of our study lies in its longitudinal design. By extending our analysis to nearly 2 years with multiple follow-up points, we discovered that this initial patella-lowering effect was not permanent; the patellar height in the isolated MPFLR group progressively relengthened to near-preoperative values. In contrast, the cohort that also underwent a TTO demonstrated stable patellar height throughout the entire follow-up period. This apparent discrepancy with the findings of Luceri et al 9 is likely explained by the differing follow-up methodologies, as their single, later time point captures a static outcome but does not account for the dynamic, time-dependent remodeling of the extensor mechanism that our study reveals. Therefore, our findings place theirs within a broader temporal context, highlighting that early postoperative changes in patellar height may not be reflective of the final, long-term outcome.
In a study of 103 knees in a pediatric population, Yang et al 18 reported a short-term decrease in patellar height at 6 months after MPFLR, measured by the CDI, Insall-Salvati ratio, and the Blackburne-Peel ratio. They excluded any patients who had undergone a TTO, thereby isolating the effect of the soft tissue procedure alone. Despite these differences in patient age range and surgical criteria, 26% of the Yang cohort had a CDI >1.3, which is comparable with the 30% in our sample. Although our findings similarly demonstrate an early postoperative decrease in the CDI, our extended follow-up data indicate that patellar height returns to near-preoperative values by 1 year. This return to length highlights the dynamic nature of the extensor mechanism during rehabilitation and remodeling.
Our data indicate that measurements of patellar height using the CDI on lateral knee radiographs within 6 months of MPFLR may not reflect the eventual values seen after 1 year, underscoring the dynamic nature of the extensor mechanism in the early postoperative period. Second, although the early postoperative CDI was significantly lower in the isolated MPFLR group (1.01 ± 0.18) than in the combined MPFLR+TTO group (1.11 ± 0.15) (P = .003), the absolute difference was modest. Finally, the clinical implications of these dynamic changes remain unclear, and future studies should prioritize outcome measures to clarify how these evolving patellar height parameters influence knee function and long-term stability.
Limitations
A significant limitation of this study is its retrospective design, which leads to typical biases traditionally seen with these studies. These include selection bias, variable postoperative rehabilitation protocols, and the inability to control for surgeon-specific factors. Furthermore, not all patients undergoing MPFLR or MPFLR+TTO queried over this study’s time period were available for early postoperative and final postoperative radiographic follow-up, which could introduce potential confounding factors. Repeating imaging of the knee at 6 months is not standard of care, and therefore these patients may not be representative of all patients undergoing MPFLR or MPFLR+TTO. Additionally, measuring patellar height is variable in nature and can have multiple factors affecting measurements. 6 However, given that this study’s ICCs were >0.9 across measurers, this is not likely to be a significant limitation. Additionally, radiographs taken at the early and final postoperative period exhibit variability, especially in the final time period. Larger studies with standardized imaging time points would potentially enhance generalizability and enable subgroup analyses (eg, by age, sex, or baseline patellar height). A limitation is that intrarater reliability was not formally assessed; however, this decision was based on the measurement's well-documented high reproducibility in previous literature.
Moreover, patellofemoral biomechanics are multifactorial. We did not account for other baseline factors such as differences in surgical techniques, rehabilitation protocols, other individual patient factors, or other anatomic variables such as tibial slope, Q-angle, or TT-TG distance, each of which could alter the risk of postoperative patellar height changes. Nor were we able to document the exact distance by which the TT was moved during osteotomy. Future investigations might include these measurements to identify specific risk factors for iatrogenic changes in patellar height or patellar tendon length. Another limitation is that this study relies on CDI as the only metric to evaluate patellar height and it is known that the evaluation of determining patella alta across various indices has been shown to be unreliable. 5
Last, prospective studies with larger patient populations and extended follow-up are essential to clarify the clinical effect of patellar height changes after these bony procedures in skeletally mature individuals. Additionally, prospective studies should include subgroup analyses based on factors such as patella alta and other baseline demographic variables. Evaluating both radiographic, patient-reported, and functional outcomes over time would help determine whether the observed patellar height alterations meaningfully affect knee function or stability in the long term.
Conclusion
Our study showed that MPFLR both with and without TTO demonstrated an eventual return toward preoperative patellar height, yet they followed different early postoperative trajectories. MPFLR demonstrated an early decrease in patellar height that progressively relengthened over time, whereas MPFLR + TTO exhibited almost no changes in patellar height.
Footnotes
Final revision submitted July 31, 2025; accepted September 12, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.K.A. has received consulting fees from Stryker. J.J.E. has received consulting fees from Depuy Synthes Products and Medical Device Business Services, support for education from Arthrex and Smith & Nephew, and a grant from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Utah (No. 00071733).