
Abstract
Background:
Patellofemoral instability (PFI) is a condition that leads to recurrent dislocation events and is typically secondary to extensor mechanism malalignment and rotational deformities. To correct malalignment, a tibial tubercle osteotomy (TTO) can be performed; however, an understanding of the associated complications, recurrence rates, and potential for reoperation is necessary.
Purpose:
To systematically review the literature to determine the incidence of postoperative complications, rate of recurrent instability, and all-cause reoperation rate after TTO for PFI.
Study Design:
Systematic review; Level of evidence 4.
Methods:
The Cochrane Database of Systematic Reviews, PubMed, Embase, MEDLINE, and CINAHL were queried for studies that reported complications after TTO. No date limits were applied. A total of 1050 studies were identified. Complications were categorized into “minor” and “major” groups using a modified Clavien-Dindo Classification. A meta-analysis was conducted to examine complication rates, recurrent instability, and all-cause reoperation, utilizing a DerSimonian and Laird random-effects model. A meta-analysis for recurrent instability was subgrouped according to follow-up periods of ≤2 years and >2 years.
Results:
A total of 38 studies were included, comprising 1546 patients, representing 1733 knees. The study dates ranged from 1989 to 2024, and the level of evidence ranged from 2 to 4. The weighted mean age at surgery was 24.1 years (range, 20-54 years), and 67% of patients were women. The weighted mean follow-up of all studies was 4.2 years. Overall, 197 minor complications, 39 major complications, 90 recurrent instability events, and 275 reoperations were identified. The minor complication rate was 9% (range, 0%-65% [95% CI, 6%-13%]). The major complication rate was 3% (range, 0%-10% [95% CI, 3%-4%]). Seven studies had a ≤2-year follow-up, and the remaining 31 studies had a >2-year follow-up. The recurrent instability rate was 3% in studies with ≤2 years of follow-ups (range, 0%-26% [95% CI, 1%-13%]). In studies with >2 years of follow-up, the recurrent instability rate was 8% (range, 0%-31% [95% CI, 6%-12%]). The all-cause reoperation rate was 16% (range, 0%-54% [95% CI, 11%-21%]).
Conclusion:
This systematic review and meta-analysis identified the incidence of complications (17%), the rate of recurrent instability (3%-8%), and the all-cause reoperation rate (16%) after TTO. TTO, performed alone or in combination with medial patellofemoral ligament reconstruction for the treatment of PFI, reliably improved clinical outcome scores in the setting of variable complication rates. Interestingly, rates of recurrent instability increased over time, and most reoperations were undertaken for hardware removal rather than revision patellar stabilization surgery.
Keywords
Tibial tubercle osteotomy (TTO) is a generalized term for a set of procedures that attempt to address some of the major anatomic risk factors of patellofemoral instability (PFI) that may lead to recurrent dislocation. Biomechanically, the effect of TTO is the alteration of the quadriceps force vector on the patella, which ideally decreases the risk of patellar dislocation.12,42 TTO types include either an isolated or combined anteriorization, medialization, and/or distalization of the tibial tubercle. 16 TTO can be done in isolation or with concomitant procedures such as proximal patellofemoral soft tissue balancing, which is also intended to stabilize the patella during knee motion and prevent dislocation.
TTO is performed to address major anatomic risk factors for PFI; however, the procedure has multiple complications ranging from minor (eg, superficial wound infection, delayed union, or hardware irritation) to catastrophic (eg, neurovascular injury or osteotomy nonunion). 50 Complications after TTO have been reported in case series, case reports, and systematic reviews.8,35,39 Reoperation rates have been reported as high as 21%, with the majority of reoperations reported for the removal of painful hardware. 39
Multiple systematic reviews have reported on complications after TTO; however, these studies either focused on short-term outcomes or lacked abundant long-term outcome data. Recurrent instability rates were not stratified by postoperative time period. Further investigation is necessary to identify long-term complications and recurrence instability rates, which may help physicians counsel patients on the risks and benefits of TTO. This study aimed to systematically review the literature to determine the incidence of complications, the rate of recurrent instability, and all-cause reoperation after TTO for PFI. We hypothesized that the incidence of complications, the rate of recurrent instability, and all-cause reoperation would be low in this patient cohort.
Methods
Before completion of this study, registration was conducted in PROSPERO (CRD42024549102). All steps of this study were completed in strict accordance with systematic review guidelines from Cochrane Methods. 26 A comprehensive query of the Cochrane Database of Systematic Reviews, PubMed, EMBASE, MEDLINE, and CINAHL databases was conducted on February 10, 2024. In accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines, studies reporting complications after TTO were identified. A broad search criterion was implemented to ensure capture of all studies that may qualify for our inclusion criteria. The query was conducted with Boolean search terms: ((tibial tubercle osteotomy) OR (tibial osteotomy) OR (TTO)) AND ((outcomes) OR (complications)). No date limits were applied.
Selection Criteria
A total of 1050 studies were identified from 1979 to 2024 and screened independently by 2 authors (X.P. and A.M.H.) for inclusion sequentially based on title, abstract, and full manuscript (Figure 1). Any discrepancies were resolved with the senior author (A.J.T.). The inclusion criteria comprised the following: studies written in the English language; clinical studies (level of evidence 1-4); studies pertaining to outcomes after TTO, specifically for the indication of PFI; and studies explicitly examining postoperative complications. The exclusion criteria included the following: studies evaluating TTO outcomes for indications other than PFI (ie, patellofemoral pain syndrome); studies in which data from PFI cohorts could not be isolated; studies examining unconventional or experimental TTO procedures; biomechanical studies; narrative reviews; and other systematic reviews.

A PRISMA flow chart for screening studies in this systematic review. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
Risk of Bias
All studies included in this systematic review were reviewed for risk of bias utilizing the Risk of Bias in Non-randomized Studies of Interventions (ROBINS I) tool.45,46 The ROBINS I system implements a systematic criterion for risk of bias within 7 discrete domains, which include confounding factors, selection bias, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, and bias in selection of the reported results. Each domain receives a designation of “low,”“moderate,”“serious,” or “critical risk of bias.” These designations are aggregated to achieve an overall risk of bias assessment. Risk of bias was assessed independently by 2 authors (X.P. and A.M.H.), and results are tabulated in a stoplight representation of all domains and overall risk of bias (Figure 2).

ROBINS I assessment in stoplight representation and bar graph summary for all studies included in this systematic review. ROBINS I, Risk of Bias in Non-randomized Studies of Interventions.
Data Extraction
Two reviewers (X.P. and A.M.H.) conducted data extraction in a standardized Excel spreadsheet. Study characteristics, patient characteristics, indication for TTO, preoperative radiologic measurements, concomitant procedures, type of TTO, method of fixation for TTO, complications, reoperations, and recurrent instability were isolated. Complications were categorized into “minor” and “major” groups using a modified Clavien-Dindo Classification. 6 Grade 1 and 2 complications were considered “minor,” and grade ≥3 complications were considered “major.” Recurrent instability and all-cause reoperation were collected and analyzed separately from other complications to improve the interpretation of the data.
Minor complications identified were as follows: infection not requiring reoperation; arthrofibrosis; minor neurologic complications not requiring surgery; minor vascular complications not requiring surgery (eg, hematoma); venous thromboembolism; hardware irritation; delayed union; wound complications not requiring surgery; and range of motion pain. Minor neurologic complications included focal sensory deficit, peroneal neurapraxia, neuroma, complex regional pain syndrome, and myalgic encephalomyelitis/chronic fatigue syndrome. Major complications identified were as follows: infection requiring reoperation; nonunion; fracture; wound complication requiring surgery; and broken hardware. All-cause reoperations were as follows: hardware removal; irrigation and debridement; fracture treatment; cartilage procedures; revision TTO; meniscectomy; and revision medial patellofemoral ligament reconstruction (MPFLR). Notably, total knee arthroplasty (TKA) was not considered a reoperation nor a complication. There were 6 TKAs and 1 patellar hemiarthroplasty.
Statistical Analysis
A meta-analysis was conducted with respect to complication rates, recurrent instability, and all-cause reoperation utilizing a DerSimonian and Laird random effects model.
5
Studies in the meta-analysis for recurrent instability were subgrouped with respects to ≤2 years of follow-up and >2 years of follow-up. A meta-analysis of recurrent instability and all-cause reoperations was only conducted with studies that explicitly reported these events. Forest plots were constructed to visualize the results of the meta-analysis. Heterogeneity was reported
18
as the Higgins and Thompson I2, between-study variance τ2, and the Cochran Q (
Results
A total of 38 studies published between 1989 and 2024 were included in this systematic review. A total of 24 studies were level 4 evidence, 11 studies were level 3 evidence, and 1 study was level 2 evidence. A total of 1546 patients and 1733 TTOs were included in this analysis. The mean age at surgery was 24.1 years (range, 12-56 years), and 67% of patients were women. The mean follow-up of all studies was 4.2 years. Study types mainly included case series (66%), followed by cohort studies (26%) and case control studies (8%). Detailed study characteristics—including level of evidence, study type, study period, number of patients, sex, mean follow-up, mean age, and mean body mass index—are displayed in Table 1.
Study Characteristics, Baseline Patient Characteristics, and Clinical Data a

BMI, body mass index; NR, not reported.
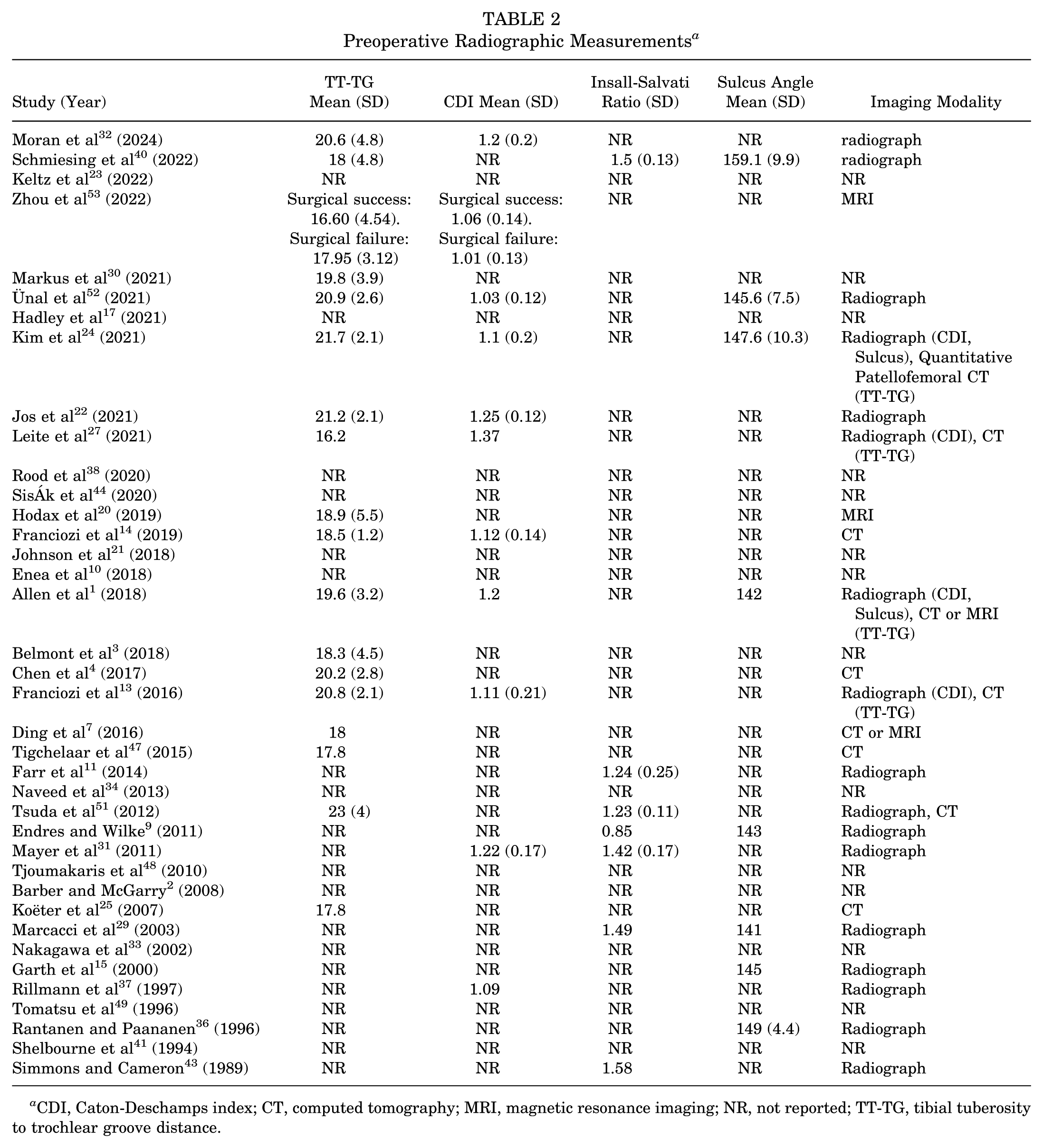
Preoperative Radiographic Measurements
Among the included studies, the tibial tuberosity to trochlear groove (TT-TG) distance was the most commonly reported preoperative radiographic measurement, documented in 17 (45%) studies. Caton-Deschamps index (CDI), Insall-Salvati ratio, and sulcus angle were also commonly reported, documented in 9 (24%), 7 (18%), and 7 (18%) studies, respectively. Of the studies that reported TT-TG distance, the mean (±SD) was 19.5 ± 3.2 mm; of the studies that reported the CDI, the mean (±SD) was 1.15 ± 0.15; of the studies that reported the Insall-Salvati ratio, the mean (±SD) was 1.33 ± 0.17; and of the studies that reported sulcus angle, the mean (±SD) was 146 ± 7.27. All reported preoperative radiographic measurements separated by study can be found in Table 2.
Preoperative Radiographic Measurements a
CDI, Caton-Deschamps index; CT, computed tomography; MRI, magnetic resonance imaging; NR, not reported; TT-TG, tibial tuberosity to trochlear groove distance.
Procedural Characteristics
Of the 1733 TTOs, the distribution of osteotomy types was 33% anteromedialization, 31% medialization only, 20% distalization only, and 16% medialization and distalization. Concomitant medial MPFLR was performed in 38% of TTOs. In accordance with the inclusion and exclusion criteria, all surgeries were indicated for recurrent patellar instability. Detailed information about the surgical technique, indication, concomitant procedures, and fixation characteristics, separated by individual study, can be found in Table 4.
Heterogeneity
The effect sizes of the included studies varied substantially, resulting in high heterogeneity (I2 = 78%) (Figure 3). When stratifying by follow-up duration, studies with ≤2 years of follow-up also had high heterogeneity (I2 = 84%). Studies with a follow-up period of >2 years displayed notably lower results, although moderate heterogeneity (I2 = 48%) was observed (Figure 4).

(A) Forest plot visualization for a meta-analysis of aggregate rates of minor complications. (B) Major complications (B). (C) All-cause reoperation.

Forest plot visualization for meta-analysis of aggregate rates of recurrent patellofemoral instability after tibial tubercle osteotomy. Studies have been subgrouped into (A) studies with ≤2 years of mean follow-up or (B) studies with >2 years of mean follow-up. (C) Additional meta-analysis of major complications, minor complications, and recurrent patellofemoral instability.
Patient-Reported Outcome Measures
Multiple studies included patient-reported outcome measures—including the International Knee Documentation Committee (IKDC), Tegner Activity Scale, Kujala, Lysholm, and Knee Injury and Osteoarthritis Outcome Score (KOOS) Quality of Life (QoL) (Table 3). Four studies included both pre- and postoperative IKDC scores and performed statistical analysis to determine significance. Four studies included both pre- and postoperative Tegner Activity Scale scores and performed statistical analysis to determine significance. Nine studies included both pre- and postoperative Kujala scores and performed statistical analysis to determine significance. Six studies included both pre- and postoperative Lysholm scores and performed statistical analysis to determine significance. Statistical analysis for significance was not found in the 2 studies that reported both pre- and postoperative KOOS QoL scores.
Patient-Reported Outcome Measures a

IKDC, International Knee Documentation Committee; KOOS, QoL, Knee injury and Osteoarthritis Outcome Score Quality of Life; NR, not reported.
Complication Rates
The overall complication rate varied from 0% to 74% within each study, while the all-cause reoperation rate varied from 0% to 54% (Table 4). There were 197 minor complications and 39 major complications. Meta-analysis demonstrated a minor complication rate of 9% (range, 0%-65% [95% CI, 6%-13%]) (Figure 3). The major complication rate was 3% (range, 0%-10% [95% CI, 3%-4%]). The 3 most common minor complications observed were hardware irritation (n = 63 [3.6%]), range of motion pain (n = 46 [2.6%]), and arthrofibrosis (n = 31[1.7%]). The 3 most common major complications observed were fracture (n = 20 [1.2%]), nonunion (n = 11 [0.6%]), and infection requiring surgery (n = 5 [0.3%]).
Individual Study Surgical Characteristics and Complications a

DVT, deep vein thrombosis; MPFLR, medial patellofemoral ligament reconstruction; NR, not reported; ROM, range of motion; TKA, total knee arthroplasty.
Rate of Recurrent Instability
There was a total of 90 recurrent instability events. Studies were further stratified by the final follow-up time, with patients categorized into groups based on ≤2 years or >2 years of follow-up. In the 7 studies with a follow-up period ≤2 years, meta-analysis demonstrated a recurrent instability rate of 3% (range, 0%-26% [95% CI, 1%-13%]). The mean follow-up in this cohort was 16 months (range, 4-24 months). In the 31 studies with >2 years of follow-up, meta-analysis demonstrated a recurrent instability rate of 8% (range, 0%-31% [95% CI, 6%-12%]) (Figure 4). The mean follow-up in this cohort was 5.90 years (range, 2.02-20.90 years). Recurrent instability rates, major complications, and minor complications were combined and reported to provide a comprehensive complication rate. Meta-analysis demonstrated an all-complication rate of 17% (range, 0%-74% [95% CI, 13%-22%]) (Figure 4C).
All-Cause Reoperation Rate
A total of 275 reoperations were identified. The all-cause reoperation rate was 16% (range, 0%-54% [95% CI, 11%-21%]). The leading causes of reoperation were hardware removal and revision TTO, accounting for 13% (n = 216) and 1.9% (n = 33) of knees, respectively. A total of 7 (0.4%) total knee arthroplasties and 1 (0.05%) unicompartmental knee arthroplasty were reported. A comprehensive tabulation of all complications reported in each respective study is presented in Table 4.
Discussion
The results of this review and meta-analysis supported the hypotheses that the overall complication rate, recurrent instability rate, and overall reoperation rate would be low. Findings in this study included a 17% complication rate, rates of recurrent instability from 3% for studies with ≤2 years of follow-up to 8% for those with >2 years of follow-up, and an overall all-cause reoperation rate of 16%. Postoperative patient-reported outcomes were overall significantly improved from preoperative status, and <1% of patients underwent conversion to definitive surgery such as arthroplasty. The interpretation of the data includes acknowledgement of the high percentage of case series included in the literature, as well as the reported overall risk of bias in the ROBINS I assessment. Nonetheless, the present review represents the comprehensive data currently available with respect to TTO, with or without concomitant MPFLR, for the treatment of PFI.
The complication rate in the reviewed studies varied from 0% to 74%. Previously reported complication rates in the literature21,28,35,39 have similarly varied, with overall rates ranging from 4% to 59%. The variation in complication rate is likely due to heterogeneity in the definition of what constitutes a complication. In this study, hardware irritation was the most common minor complication reported (3.6%). The hardware irritation rate is difficult to compare to the literature because not all studies defined it as a complication.28,35 Johnson et al 21 reported a 21% rate of painful hardware in their 240-patient retrospective cohort study. One quarter of complications identified in this review were considered major. In this study, tibial fracture was the most common major complication, occurring at a rate of 1.2%. Fracture rates in the literature ranged from 1% found by Payne et al 35 to 3.7% reported by Lundeen et al. 28 Nonunion was the second most common major complication in this review. Payne et al 35 reported that nonunion was one of the most devastating complications and typically occurred when the tibial tubercle was completely detached. Complete detachment of the tibial tubercle is typically done to address patella alta, which is often determined by an elevated CDI or Insall-Salvati ratio. The nonunion rate was 0.6% in this study compared with 0.8% in the study by Payne et al. 35 Although major complication rates were low, patients should be counseled on the risk of fracture and nonunion, as the consequences of these complications are significant.
The rate of recurrent instability after TTO, alone or in combination with MPFLR, for PFI varied based on follow-up duration in the included studies. The overall instability rate was 11%, with more than three-quarters of recurrent instability being reported in studies with >2 years of follow-up. To the author’s knowledge, other reviews have not reported on rates of recurrent instability, nor have they stratified rates based on follow-up duration. Some of the studies in this review that reported high levels of instability include Tsuda et al, 51 who reported an 11.3% rate of postoperative patellar instability and found a statistical correlation with the magnitude of patella alta. Tsuda et al 51 stated that patient selection for Fulkerson (anteromedialization) osteotomy should be based on predisposing anatomic factors for patellar instability, with a focus on patellar height. Similarly, Hodax et al 20 reported a 13.5% rate of recurrent dislocation at a mean follow-up of 3.8 years. Nakagawa et al 33 reported recurrent dislocation in 6 knees (13.3%), with 2 of those 6 knees sustaining >1 dislocation postoperatively, with a mean study follow-up of 13.4 years. Nakagawa et al 33 suggested that stabilization of the patella is difficult when habitual dislocation is associated with abnormalities in bone morphology or when there is generalized joint laxity. The difference in recurrent instability rates based on follow-up duration warrants further research to identify risk factors for late instability.
The all-cause reoperation rate was high (16%), with removal of hardware being the most common reason for reoperation (13%). Hardware removal rates vary considerably in the literature but are uniformly high. Lundeen et al, 28 in a retrospective cohort study, reported a 11.7% rate and 2 systematic reviews found rates from 39 21% to 35 36.7%. Not all studies in this review reported on the reason for hardware removal; therefore, it was not possible to extrapolate the most common complication leading to reoperation for hardware removal. Despite the high reoperation rate, revision TTO was performed in only 1.9% of the cohort. The revision TTO rate was comparable with data from a review by Saltzman et al, 39 which found a 1.5% revision rate. Conversion to an end-stage procedure, such as total or unicompartmental knee arthroplasty, was exceedingly rare, occurring in only 8 patients (0.52%). The low incidence of conversion to arthroplasty may be secondary to insufficient follow-up durations for this end-stage procedure. In this review, postoperative patient-reported outcomes were consistently and significantly improved in nearly all studies that included these metrics. The high rate of hardware removal previously reported in the literature and reinforced in this study indicates that physicians should carefully discuss this risk with patients and counsel them on the potential for additional hardware removal procedures.
Limitations
Limitations of the study include the retrospective nature, with the level of evidence for the majority of the reviewed literature being low, as 66% of the studies were case series. The literature with higher levels of evidence is sparse for TTO. Additional limitations include heterogeneity of the cohort in terms of type of TTO performed (eg, medialization, distalization) and concomitant procedures (eg, MPFLR). Another limitation is that it was often difficult to delineate the reason for hardware removal. While cases were likely due to irritation, patient preference, or other factors, this was often not explicitly indicated. Thus, there was a discrepancy between the percentage of patients experiencing hardware irritation and the percentage of patients undergoing hardware removal, with hardware irritation likely being underreported. The definition of postoperative recurrent instability varied across studies. While some studies explicitly reported recurrent patellar dislocation, others simply stated “recurrent instability.” Thus, it may be unclear whether this was a recurrent dislocation, subluxation, or positive apprehension. There was also heterogeneity in terms of the reporting of imaging type and measurements. The variation in types of procedure and reporting limits the ability to draw definitive conclusions with a greater level of evidence. The large sample size and stratification of data by follow-up duration provide a framework by which surgeons can estimate the type and rate of complications after TTO.
Conclusion
This systematic review and meta-analysis identified the incidence of complications (17%), the rate of recurrent instability (3%-8%), and all-cause reoperation (16%) after TTO. TTO, performed alone or in combination with MPFLR for the treatment of PFI, reliably improved clinical outcome scores in the setting of variable complication rates. Interestingly, recurrent instability rates increased over time, and most reoperations were performed for hardware removal rather than revision patellar stabilization surgery.
Footnotes
Final revision submitted June 4, 2025; accepted June 24, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.B.F.S. has received consulting fees from Smith & Nephew; has received nonconsulting fees from Smith & Nephew and Aesculap Biologics LLC; is a board or committee member of the American Academy of Orthopaedic Surgeons and International Cartilage Regeneration & Joint Preservation Society; is an editorial or governing board member of Cartilage; has received research support from JRF; and is a paid consultant for Phoenix Kinetic and Relive biotechnologies. A.J.K. has received research support from Aesculap/B.Braun, Arthrex, Arthritis Foundation, Ceterix, and Histogenics; has received intellectual property royalties from Arthrex; has received speaking fees from Arthrex; has received consulting fees from Arthrex, Responsive Arthroscopy LLC, and Joint Restoration Foundation; has received personal from Ceterix, Gemini Mountain Medical LLC, and Smith & Nephew; has received honoraria from Vericel, Joint Restoration Foundation, Responsive Arthroscopy, and Musculoskeletal Transplant Foundation; has received a grant from DJO, Foundation and Exatech; has received nonconsulting fees from Arthrex; has received consulting fees from Arthrex, Responsive Arthroscopy LLC, and Joint Restoration Foundation; has received royalties or a license from Arthrex and Responsive Arthroscopy LLC, and Joint Restoration; has served on the medical board of trustees for the Musculoskeletal Transplant Foundation; is a board or committee member of the International Cartilage Repair Society, the International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine, the Minnesota Orthopedic Society, and the Musculoskeletal Transplantation Foundation; is a paid consultant for JRF Ortho and Vericel; and is an editorial or governing board member of The American Journal of Sports Medicine. M.H. has received education payments from Arthrex, Foundation Medical, Medwest Associates, and Smith & Nephew; honoraria from Encore Medical; hospitality payments from Orthalign, Stryker, and Medical Device Business Services; consulting fees from Vericel, DJO-Enovis, Moximed, and Vericel; and support for education from Smith & Nephew and Medwest Associates; and is an editorial or governing board member of the Journal of Cartilage and Joint Preservation. K.O. has received consulting fees from Arthrex, Smith & Nephew, and Endo Pharmaceuticals; support for education from Gemini Medical, Smith & Nephew, Arthrex, Endo Pharmaceuticals, Pinnacle Inc, and Medwest Associates; nonconsulting fees from Smith & Nephew; hospitality payments from Arthrex, Stryker, Wright Medical Technology, Medical Device Business Services, and Zimmer Biomet; and a grant from Arthrex. A.J.T. has received hospitality payments from Stryker, Zimmer Biomet Holdings, Foundation Medical LLC, DePuy Synthes, Wardlow Enterprises, Vericel, Arthrex, and Medical Devices Business Services Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.