
Abstract
Background:
Scheduled follow-up (FU) appointments are a vital element of monitoring patient progress and outcomes. However, failure to attend FU appointments continues to be a regular problem in orthopaedics.
Purpose:
To investigate the relationship between FU appointment attendance and functional outcomes after hip arthroscopy.
Study Design:
Cohort Study; Level of evidence, 3.
Methods:
A retrospective analysis of prospectively collected data was conducted in patients who underwent primary hip arthroscopy for symptomatic labral tears between 2014 and 2023. FU attendance after suture removal was used to categorize patients into 2 cohorts based on whether they attended all standard FU appointments (AA) or missed at least 1 FU appointment (MAO) at 3-, 6-, or 12-month intervals. Patient-reported outcome measures (PROMs) included the modified Harris Hip Score, Nonarthritic Hip Score, Hip Outcome Score–Activities of Daily Living, HOS–Sports Specific Subscale, 33-item International Hip Outcome Tool, and patient satisfaction.
Results:
Overall, 178 hips (54.5% women) met the inclusion criteria, with 110 hips (mean age, 35.9 ± 10.6 years) in the AA cohort and 68 hips (mean age, 35.1 ± 11.8 years) in the MAO cohort. Both groups had similar radiographic and demographic characteristics, except for the distribution of Asian and White patients (18 vs 3 and 44 vs 100, respectively; P < .001). PROMs were statistically similar at all time points (P > .05). Multivariate linear regression model analyses showed no differences after adjusting for cohort, distance from clinic, sex, race, and age for all PROMs. Additionally, both cohorts achieved clinically meaningful outcomes (CMOs) at similar rates (P > .05).
Conclusion:
Patients who missed at least 1 FU appointment achieved similar improvements in functional outcomes compared with those who attended all. Both cohorts achieved minimal clinically important difference, patient acceptable symptom score, and significant clinical benefit at comparably high rates. These findings suggest that functional outcomes are not associated with FU appointment attendance. Additionally, those who do not attend all of their postoperative FU appointments can still achieve CMOs.
Keywords
Follow-up (FU) appointments are an important part of monitoring patient progress after orthopaedic surgery. They provide the opportunity for a surgeon to evaluate postoperative recovery and identify complications. However, the demand regular FU imposes on orthopaedic clinics continues to increase as the popularity of orthopaedic procedures grows. 25 From a financial perspective, nonattendance has been estimated to result in a mean of $129.48 in lost revenue per visit at a federally qualified health center, and the implementation of telemedicine visits as an alternative to in-person visits saved $16,444 of monthly revenue. 1 More importantly, nonattendance represents missed opportunities for other patients to be seen in the clinic.
Loss to FU continues to present as a common challenge in postoperative care.3,55 There has been extensive exploration into the prognostic factors associated with FU attendance in orthopaedics. Male sex, younger age, Black or African American race, insurance type, illicit drug abuse, increased distance from clinic, and worse baseline scores are among the factors that left patients at a higher risk of being lost to FU.3,15,17,18,23,28,36,44,45,54,55 This is a result of complex influences such as access to reliable transportation, cost, and socioeconomic status.3,55 By recognizing those at greater risk of nonattendance, more effective alternatives and preventative strategies for FU attendance can be strategically implemented to consider the needs of these specific demographics. Furthermore, research into the effect that patient outcomes have on FU attendance in an orthopaedic setting has not found any clear association between the 2 variables and warrants further investigations. 28
Previous studies have shown that patients who miss preoperative appointments before total joint arthroplasty have an increased risk for postoperative infection.34,35 However, there is minimal understanding for those who do not attend FU visits after surgery. One investigation has found no correlation between FU status and clinical outcomes after spine surgery. 28 Therefore, the purpose of this study was to (1) compare patient-reported outcome measures (PROMs) in patients who underwent hip arthroscopy who missed ≥1 FU appointments (MAO) versus those who attended all (AA) FU appointments after suture removal, (2) understand the effect of risk factors that contribute to missed FUs, and (3) compare rates of achieving clinically meaningful outcomes (CMO) for both cohorts. It was hypothesized that patients who miss at least 1 FU appointment would have worse functional outcomes.
Methods
Study Population and Design
Institutional review board (IRB) approval (IRB, 2019P002191 and 2013P001442) was obtained for this study. A retrospective analysis of prospectively collected data was conducted with patients who underwent primary hip arthroscopy for symptomatic labral tears. FU appointment attendance after suture removal was used to stratify patients into 2 groups at 1 year postoperatively. One cohort included patients who had attended all standard FU appointments (AA), while the other cohort included those who had missed at least 1 FU appointment (MAO). All patients were treated by a single, high-volume, fellowship-trained surgeon (S.D.M.) at a large, nonprofit, integrated health care system in New England between April 2014 and June 2023. The exclusion criteria were as follows: age <18 years, Tönnis grade >1, lateral center-edge angle <20º, previous ipsilateral hip arthroscopy, contralateral hip arthroscopy, and no PROMs completed at baseline or 12 months after surgery.
Before surgery, all patients with hip pain received hip and pelvis radiographs along with physical examinations. Patients with positive tests upon physical examination (ie, pain and/or limited range of motion with flexion, adduction, internal rotation, or flexion, abduction, and external rotation) underwent magnetic resonance arthrography, diagnostic and therapeutic intra-articular anesthetic/corticosteroid injection, and a minimum of 3 months of nonoperative formal physical therapy. Patients with persistent hip pain were offered hip arthroscopy. Within 1 year postoperatively, standard FU appointments included office visits at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year.13,33,37,43
Data collected from the electronic medical record included age, sex, race, insurance type, FU appointment dates, and attendance. Additionally, patient residential addresses and Google Maps (Alphabet) were used to calculate the driving distance and time to the clinic for scheduled appointments. The Area Deprivation Index (ADI), a validated score that calculates neighborhood-level socioeconomic disadvantage based on the patient's address, was recorded using the Neighborhood Atlas by the Center for Health Disparities Research at the University of Wisconsin–Madison. The ADI was reported on a scale of 1 to 100, with a score of 1 indicating the least disadvantaged group on the scale. 21 All PROM data were prospectively collected via electronic mail surveys sent during the corresponding postoperative time point to be completed at home. The PROMs used included the modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), HOS–Sports Specific Scale (HOS-SSS), Nonarthritic Hip Score (NAHS), the 33-item international Hip Outcome Tool (iHOT-33), and patient satisfaction at 12 months postoperatively. CMOs, such as the minimal clinically important difference (MCID), patient acceptable symptom state (PASS), and significant clinical benefit (SCB), were used as secondary outcomes. At the 6-week postoperative FU visit, all patients confirmed to be following the rehabilitation protocol as instructed. 37
Abbreviated Surgical Technique and Postoperative Rehabilitation
Once general anesthesia was administered, the patient was positioned supine on a hip distraction table (Advanced Supine Hip Positioning System; Smith & Nephew) with a silicone-padded perineal post. Intra-articular access was facilitated via the puncture capsulotomy technique with anterolateral, anterior, midanterior, and Dienst portals, as previously described to preserve the iliofemoral ligament and zona orbicularis.2,8 To minimize neurovascular complications and maintain ambient intra-articular temperatures for chondrolabral junction preservation, sparing use of intermittent traction and pulsed intra-articular lavage, respectively, were applied.32,38,40,50,52 Acetabular and femoral osteoplasty were performed as indicated without violation of the chondrolabral junction. 52 Repair was performed for small, discrete, linear tears that had adequate healthy tissue amenable to suture anchor fixation. However, labral augmentation via capsular autograft was performed if the labrum was irreparable due to the indication of complex tears, tears involving the chondrolabral junction, or degenerative labral tissue.38,40 After labral repair or augmentation, traction was fully released to ensure restoration of the hip suction seal and formation of an anatomic “in-round” repair. 50
Notably, during the study period, the senior surgeon's (S.D.M.) method of treating full-thickness chondral flaps, focal Outerbridge grade ≥2 lesions, and chondrolabral junction breakdown shifted from microfracture (April 2014 to March 2018) to a standardized method of bone marrow aspirate concentrate augmentation (April 2018 to June 2023).26,30,31,51 There were no other notable variations in surgical technique by the senior surgeon within the study period. To ensure equitable patient access, all costs associated with bone marrow aspirate concentrate were covered by the Conine Family Fund for Joint Preservation (a philanthropic organization without affiliations with industry).
Statistical Analysis
Univariate analysis was performed using a 2-tailed independent t test or a Pearson chi-square test with Yates continuity correction, as appropriate. Based on recent findings in the literature regarding risk factors that affect FU appointment attendance, further analysis was performed using a multivariate linear regression model adjusting for cohort group, age, race, sex, and distance from clinic.3,55 To avoid collinearity in the linear regression models, driving distance from the clinic was adjusted for solely as a measurement of time, as opposed to adjusting using time and miles. This was done to best represent the distance barrier throughout the entire Boston metropolitan area. These regression models were done for all PROM scales (ie, mHHS, HOS-ADL, HOS-SSS, NAHS, and iHOT-33). Statistical analysis was performed using R Version 4.4.2 (The R Foundation for Statistical Computing), and P < .05 was considered statistically significant.
To determine the number of patients required to detect differences in mHHS scores between cohorts at 1 year, an a priori power analysis was performed using G*Power 3.1. Based on previous literature and historical data from our prospective registry, the following assumptions were made: a standard deviation of 13 points, α = .05, an allocation ratio of 1 to 1, and a between-group difference of 6.9 (ie, mHHS MCID value at 1 year). 39 Given these assumptions, 114 patients were required to achieve 80% power.
Results
Patient Characteristics
In total, this study evaluated 323 hips that underwent hip arthroscopy between January 2014 and June 2023. A total of 178 hips met the inclusion criteria and were subsequently included in the data analyses (Figure 1). There were 110 patients in the AA cohort (mean age, 35.9 ± 10.6 years) and 68 patients in the MAO cohort (mean age, 35.1 ± 11.8 years) (Table 1). Within the MAO cohort, 49 patients missed 1 FU visit, 15 missed 2, and 4 did not attend any FU appointments after 6 weeks. Baseline comparisons between cohorts revealed no significant differences in patient characteristics, including age, sex, laterality, body mass index, labral management, National ADI, insurance type, and distance from the clinic. Race was unequally distributed between groups, with more Asians in the MAO group and 1 White patient in the AA group (P < .001) (Table 1). Additionally, radiographic findings, including Tönnis grade, Tönnis angle, lateral center edge angle, and femoroacetabular impingement (FAI) type, were similar at baseline (Table 2).
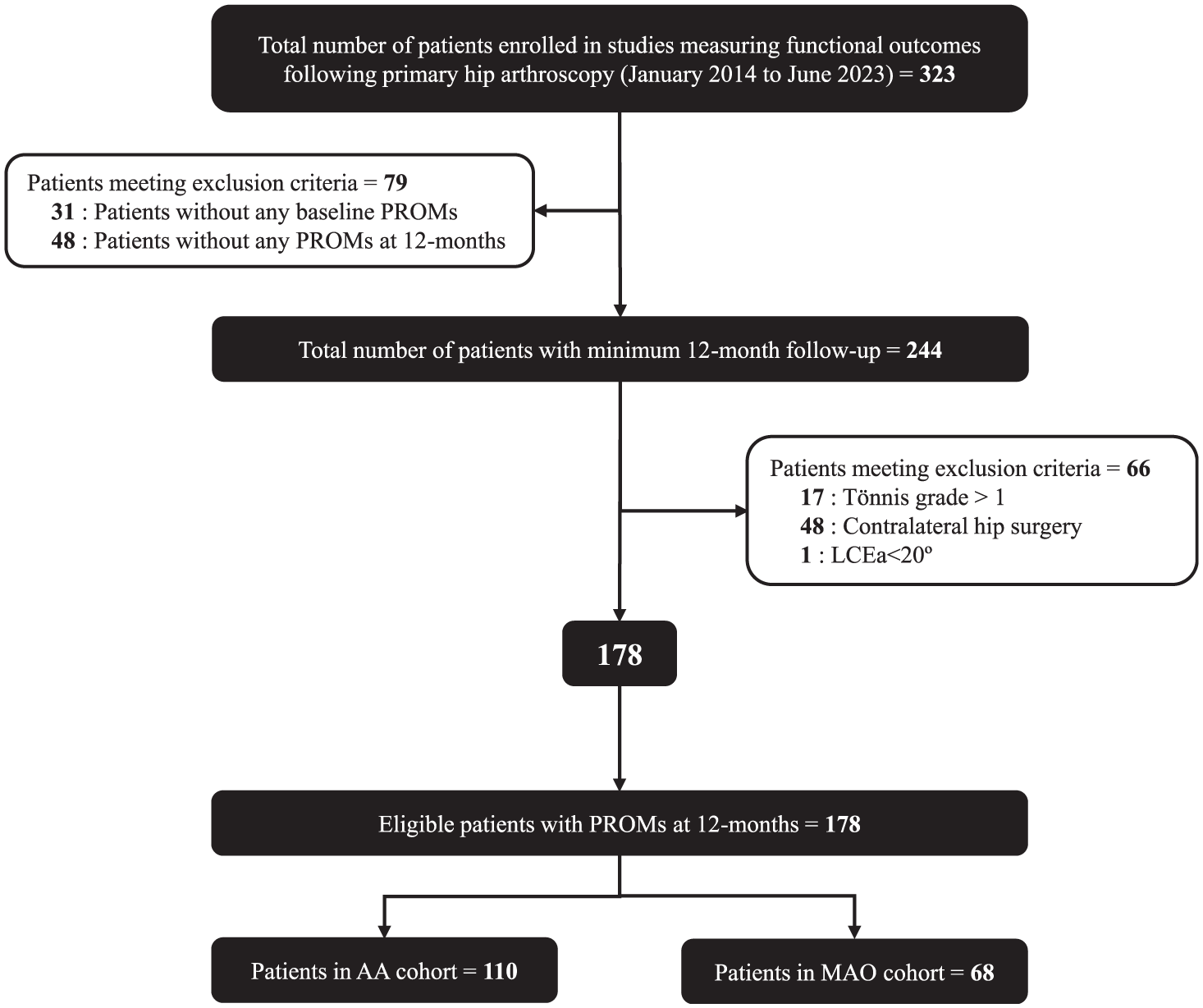
CONSORT diagram. AA, attended all follow-ups; CONSORT, Consolidated Standards of Reporting Trials; FU, follow-up; LCEa, lateral center edge angle; MAO, missed ≥1 follow-up; PROM, patient-reported outcome measure.
Patient Characteristics and Radiographic Findings a

Data are reported as mean (SD) or n (%). The bold P value denotes statistical significance (P < .05). AA, attended all follow-up; ADI, Area Deprivation Index; BMI, body mass index; MAO, missed ≥1 follow-up.
Yates continuity correction was used.
Significant post-hoc differences.
Radiographic Findings a
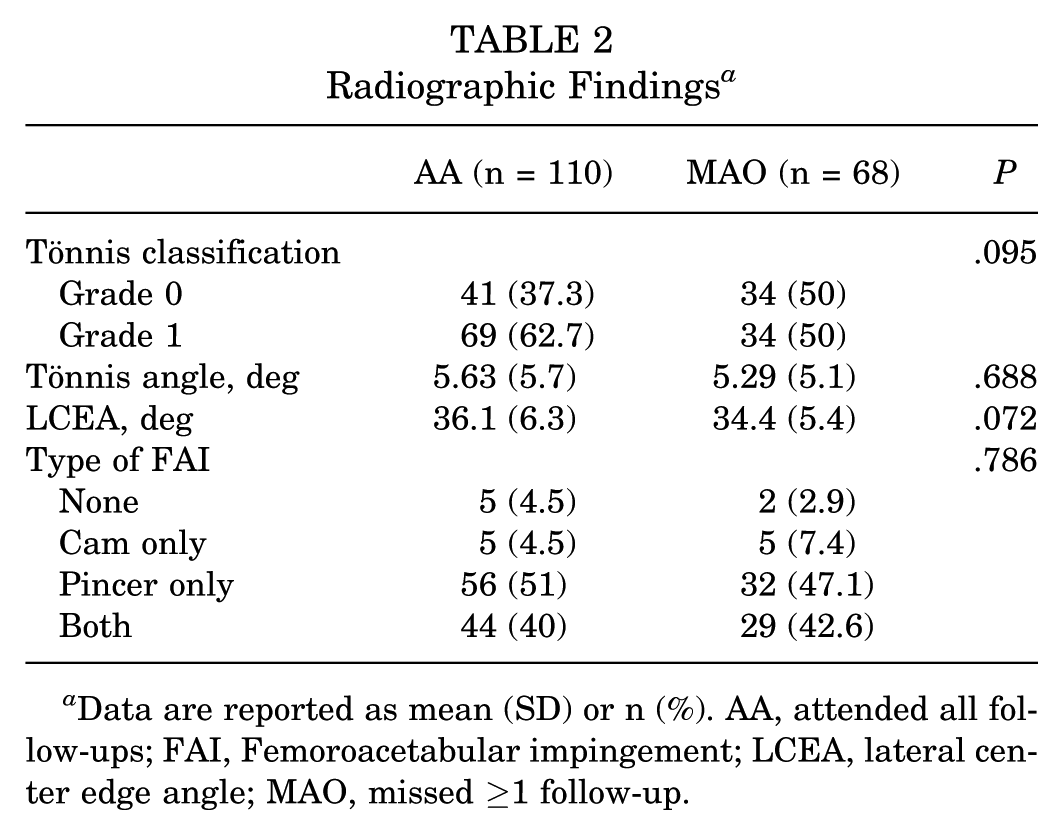
Data are reported as mean (SD) or n (%). AA, attended all follow-ups; FAI, Femoroacetabular impingement; LCEA, lateral center edge angle; MAO, missed ≥1 follow-up.
Patient-Reported Outcome Measures
No significant differences were found when comparing baseline PROMs between cohorts: mHHS (AA, 64.5 ± 13.3 vs MAO, 64.4 ± 12.6; P = .945), NAHS (68.1 ± 16.3 vs 66.8 ± 13.9; P = .601), HOS-ADL (73.6 ± 17.9 vs 72.9 ± 14.5; P = .772), HOS-SSS (46.1 ± 22.4 vs 45.5 ± 21.4; P = .862), and iHOT-33 (43.9 ± 16.9 vs 41.4 ± 16; P = .330). This trend persisted at all timepoints (ie, 3-months, 6-months, and 12-months) (Table 3). Patients in both cohorts reported similar levels of patient satisfaction and rates of answering “yes” when asked if they would undergo the same treatment again (P = .520 and P = .232, respectively). Lastly, no differences were observed in rates of revision hip arthroscopy or conversion to total hip arthroplasty (THA) at the 12-month FU (P > .99 for both) (Table 4).
Unadjusted PROMs a

Data are reported as mean ± SD or n. AA, attended all follow-ups; HOS-ADL, Hip Outcome Score- Activities of Daily Living; HOS-SSS, Hip Outcome Score-Sports Specific Subscale; iHOT-33, 33-item International Hip Outcome Tool; MAO, missed ≥1 follow-up; mHHS, Modified Harris Hip Score; NAHS, Nonarthritic Hip Score.
Patient Satisfaction and Surgical Failure at 1 Year a

Data are reported as n (%). AA, attended all follow-ups; MAO, missed ≥1 follow-up.
Yates continuity correction was used.
A multivariate linear regression analysis was then performed to adjust for demographic factors associated with missed FU appointments.3,55 After adjustment for the factors above, there were no significant differences between cohorts for mHHS, HOS-ADL, HOS-SSS, NAHS, and iHOT-33 scores (P > .05 for all) (Table 5).
Multivariate Linear Regression Models a

HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports Specific Subscale; iHOT-33, 33-item International Hip Outcome Tool; MAO, missed ≥1 follow-up; mHHS, Modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PROM, patient-reported outcome measure.
CMOs and Complications
CMOs, such as MCID, PASS, and SCB, were used as secondary outcomes.39,46 There were no differences between cohorts in the rates of achieving CMOs at 12 months, including MCID, PASS, and SCB for all PROM scales (P > .05) (Table 6).
Clinically Meaningful Outcomes at 1 Year a

Yates continuity correction was used for all tests. AA, attended all follow-ups; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports Specific Subscale; iHOT-33, 33–item International Hip Outcome Tool; MAO, missed ≥1 follow-up; MCID, minimal clinically important difference; mHHS, Modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PASS, patient acceptable symptom score; SCB, significant clinical benefit.
Discussion
The first major finding of the present study was that after hip arthroscopy, AA patients did not have significantly different functional outcome scores compared with MAO patients at a 1-year FU. Second, demographic factors that influenced FU attendance did not affect PROM scores. Ultimately, both cohorts achieved similar rates of CMOs. Together, these findings suggest that functional outcomes are not associated with FU appointment attendance.
This study evaluated functional outcome scores after hip arthroscopy and determined that FU attendance did not have any effect. AA patients had similar functional outcome scores to MAO patients at all postoperative time points. Despite the growing interest in FU attendance, the present study is the first to explore the relationship between FU appointment attendance and PROMs after hip arthroscopy.
After adjusting for demographic variables, variations in cohort, distance from clinic, age, or sex did not display any notable differences in PROMs, as AA patients maintained similar PROMs to MAO patients at all time points up to a 1-year FU.3,17,23,44,54,55 These findings were consistent with recent studies in orthopaedics that found FU attendance did not have a significant relationship with postoperative outcomes.19,20,22,28,41 Joshi et al 19 reported that loss to FU status did not affect survivorship when revision surgery or revision surgery with severe pain were considered in total knee arthroplasty (TKA) surgery. King et al 22 found similar results when exploring outcomes 5 years after TKA. By utilizing response rates to PROM surveys in arm or shoulder registries, 2 studies also found no differences in outcomes for those who initially responded and those who required a reminder to complete the surveys.20,41 Lastly, Levy et al 28 directly compared PROMs with loss to long-term FU status and found no association between the 2 variables after various spine surgeries.
The third key finding is that there were no differences in achieving CMOs between cohorts. Furthermore, the MAO cohort exhibited a consistent trend of similar or even improved CMOs compared with the AA group, however this did not reach statistical significance. This trend is further explained by Sethuraman et al, 47 who found that 45% of patients do not wish to attend routine FU appointments if they are asymptomatic. This was due to a patient's preference to save wages and time by not attending their FU appointment. Additionally, the patients who preferred not to attend FU appointments believed their quality of care would not be affected without an office visit. Similar findings were observed in the present study, by the lack of differences in patient satisfaction and when patients were asked if they would repeat the same procedure. This provides evidence for a need to reevaluate postoperative monitoring, as attending FU visits poses a significant cost to the patient through lost wages and time. 14
Although FU visits play a necessary role in monitoring patient progress after surgery, the present study provides evidence that routine postoperative visits may not be required in all cases. The ever-growing popularity of hip arthroscopy increases the burden on orthopaedic outpatient clinics. 25 Identifying patients who do not need to be closely monitored (ie, low-risk of complication, progressing well, or no preoperative risk factors for worse outcomes) can help alleviate this burden by prioritizing in-person clinic visits for patients who may require closer monitoring such as those with evidence of more radiographic osteoarthritis (ie, higher Tönnis grade), arthroscopic osteoarthritis (ie, higher Outerbridge grade), significant chondral labral junction breakdown, noncompliance with postoperative protocol, and/or more severe labral damage.4,5,7,10,11,16,29,49 An alternative FU method that has been examined is telemedicine visits. Studies have examined the efficacy of telehealth visits and found that they do not affect satisfaction scores; instead, they provide access to care by offering cost and time savings.1,48,53 Offering the option for telehealth visits could help optimize the limited time available during outpatient clinics for those who require more thorough monitoring. Additional investigations in other specialties found that FU through general practitioners, nurses, telephone encounters, or mail-in surveys was a valuable alternative to surgeon-led clinics.9,12,24,42,47 Together, this supports the need to investigate clinic optimization in orthopaedics to allow surgeons the opportunity to prioritize valuable resources for patients who need them.
Limitations
This study is not void of limitations. First, all surgeries were performed by a single experienced senior surgeon who had performed >1000 hip arthroscopy procedures before April 2014. As a result, these outcomes may not be generalizable to other surgeons, especially regarding capsular management, methods of labral reconstruction, and treatment of chondrolabral/chondral injury.6,8,30,38,40 Second, no conclusions can be made for the Black/African-American race and insurance status due to a lack of diversity for these variables. To minimize this limitation, interpretations of the results were maintained within this context. Lastly, the generalizability may be limited as national ADI scores were notably high; however, a recent study found that the ADI does not affect outcomes at a 1-year FU after hip arthroscopy. 27
Conclusion
Patients who missed at least 1 FU appointment achieved similar improvements in functional outcomes compared with those who attended all. Both cohorts achieved MCID, PASS, and SCB at comparably high rates. These findings suggest that functional outcomes are not associated with FU appointment attendance. Additionally, those who do not attend all of their postoperative FU appointments can still achieve CMOs.
Footnotes
Final revision submitted July 10, 2025; accepted August 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was provided by the Conine Family Fund for Joint Preservation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Partners Human Research (2019P002191 and 2013P001442).