
Abstract
Background:
Risk factors for injury to the thrower's shoulder remain a controversial topic.
Purpose:
To prospectively investigate the relationship between risk factors and the outcomes of pain, injury, and dysfunction in the dominant shoulder of volleyball athletes.
Study Design:
Cohort study; Level of evidence 2.
Methods:
Professional and masters-level athletes were followed for 8 months. All participants underwent physical examination, goniometry, dynamometry, and ultrasound. Injured athletes underwent magnetic resonance imaging. We analyzed the association of 15 risk factors with shoulder pain, injury, and dysfunction. Pain was defined as any score >0 on a 10-point visual analog scale. Injury was defined as any event causing an absence of ≥1 day from volleyball activities. An American Shoulder and Elbow Surgeons (ASES) score below 100 was considered dysfunction.
Results:
A total of 95 athletes were analyzed. The incidence rates of shoulder pain, injury, and dysfunction were 52.6%, 38.9%, and 47.3%, respectively. The most common injuries were subacromial bursitis (94%), superior labrum from anterior to posterior lesions (73%), and acromioclavicular joint arthritis (62%). Age, sex, glenohumeral internal rotation deficit, total range of motion, insufficient external rotation, category, player position, years of volleyball experience, and training and game overload were not significantly associated with the outcomes. Athletes with scapular dyskinesis had 4.2-fold increased odds of pain (95% CI, 1.7-10.4; P = .001), 3.5-fold increased odds of injury (95% CI, 1.3-9.2; P = .001), and lower ASES scores (P = .003). Those with a history of shoulder injury had 25.3-fold increased odds of pain (95% CI, 8.15-78.7; P < .001), 606-fold increased odds of reinjury (95% CI, 33.1-11085; P < .001), and lower ASES scores (P < .001). Athletes with strength imbalance at 90°/90° had 2.6-fold increased odds of injury (95% CI, 1.1-6.0; P = .03). Starters had 2.7-fold increased odds of injury (95% CI, 1.0-7.0; P=0.032) and lower ASES scores (P = .01). Decreased humeral retroversion was a protective factor against injury (OR, 0.2; 95% CI, 0.1-1.0; P = .03).
Conclusion:
Scapular dyskinesis and a history of shoulder injury are risk factors for shoulder pain, injury, and dysfunction. Being a starter is a risk factor for injury and dysfunction. Strength imbalance is a risk factor for injury. Decreased humeral retroversion is a protective factor against injury.
Volleyball is classified as an overhead sport because of characteristic movements such as serves and spikes, where athletes use their arm over the head to propel the ball toward an opponent or teammate.1,33 Professional athletes may execute up to 40,000 spikes annually, 8 subjecting the shoulder to forces that often exceed physiological limits and propelling the ball at speeds reaching 120 km/h.9,24,34
Frequent volleyball practice generates stresses on the shoulder that result in adaptive changes of several structures, such as the rotator cuff, capsulolabral complex, biceps tendon, humeral head, and other soft tissues and osseous structures of the glenohumeral joint.15,41 The relationship between these musculoskeletal adaptations and the risk of injury to the thrower's shoulder has been studied over the past 2 decades.2,22 However, few longitudinal and prospective studies have exclusively focused on the shoulder of the volleyball athlete. 12 Addressing this gap was the primary motivation for conducting this study.
The purpose of this study was to prospectively investigate the relationship between 15 variables, identified as risk factors in the orthopaedic literature, and the outcomes of pain, injury, and dysfunction in the dominant shoulder of volleyball athletes. We hypothesized that select clinical, biomechanical, and sport-specific factors would demonstrate significant associations with these outcomes over the season.
Methods
We conducted a prospective cohort study using a convenience sample of male and female volleyball players from both masters-level and professional categories. Participants were followed across 3 seasons (2021/2022, 2022/2023, and 2023/2024), with each season spanning 8 months from August to April of the following year. Masters athletes were defined as nonprofessional athletes who take part in competitions specifically designed for individuals aged 35 years or older. 7
Due to the inherent challenges in prospectively enrolling high-level athletes for this type of study, a formal sample size calculation was not feasible. Therefore, the final sample size was determined by the number of athletes who met the inclusion criteria during the study period and consented to participate.
Systematic assessments occurred at 2 time points: preseason (risk factors) and postseason (outcomes). These assessments included clinical evaluation, physical examination, goniometry, ultrasound, and isometric dynamometry of both shoulders. Only data from the dominant shoulder were analyzed for this study.
Two orthopaedists (D.C.T. and R.A.M.) with 7 and 9 years of experience in shoulder and elbow conditions, assisted by a physical therapist (P.H.C.D.) with 5 years of experience in orthopaedic trauma, conducted all assessments. Only athletes with shoulder injuries underwent magnetic resonance imaging (MRI), within days of diagnosis. MRI scans were evaluated by a radiologist (N.L.M.) with 5 years of experience in the musculoskeletal field (N.L.M.). Injured athletes were referred to the medical department for treatment and rehabilitation.
Data interpretation was performed at the conclusion of the study.
The study was approved by the ethics committee of Faculdade de Medicina da Universidade de São Paulo. All athletes gave informed consent before inclusion.
Participants
In the week before the start of the season, athletes were assessed for eligibility for the study. Eligible participants were all athletes who had been called up for the seasons under investigation and did not have any restrictions on sports practice. Athletes were excluded from the study if they had medical restrictions, were recovering from injury, refused to participate, or withdrew consent.
Risk Variables
A total of 15 risk factors were analyzed and divided into 4 categories:
Musculoskeletal adaptations: glenohumeral internal rotation deficit (GIRD),8,29-31,40,43 total range of motion (TROM),8,29-31,38,40 insufficient external rotation (IER),8,29-31,40,43,44 decreased humeral retroversion,19,32 scapular dyskinesis,18,29,30,34,40 and imbalanced isometric shoulder strength between internal rotation/external rotation (IR/ER) of the rotator cuff muscles measured at 2 shoulder positions12,14,29,30,33,34,40
Sport-related variables: category (professional or masters),29,30,34,40 team composition (starter or substitute),29,30,34,40 player position (middle hitter, setter, libero, opposite hitter, or outside hitter),12,29,30,34,40 training and game overload,29,30,34,40 and years of volleyball experience29,30,34,40
Health history: history of dominant shoulder injury14,29,30,34,40
A training and game load exceeding 16 hours per week was considered overload and a risk factor. 33 Shoulder injury history was defined as any dominant shoulder injury occurring in previous seasons.14,29,30,34,40
Outcomes of Interest
Three outcomes were analyzed: shoulder pain, injury, and dysfunction. Pain was assessed using a 10-point visual analog scale (VAS) 13 and was defined as any score >0. Injury was defined as any event occurring during scheduled games or training that resulted in the athlete's being sidelined for ≥1 days. 1 Dysfunction was assessed using the American Shoulder and Elbow Surgeons (ASES) scale, and a score <100 was considered dysfunction. 23
Assessment of Range of Motion (ROM)
Shoulder ROM was assessed as illustrated in Figure 1. 47 GIRD, TROM, and IER were measured with a goniometer by 2 examiners (D.C.T. and P.H.C.D.). The first examiner (D.C.T.) manually stabilized the shoulder by positioning the thumb on the coracoid process and the fingers around the shoulder and scapula (C-shaped hand) and then performed passive IR and ER. The second examiner (P.H.C.D.), with the axis of rotation of the goniometer at the olecranon, performed the measurements using the ulnar shaft and styloid process as references.20,44,47 GIRD was defined as IR loss >18° in the dominant shoulder compared with the nondominant shoulder.20,45,47 TROM was defined as a total rotation deficit >5° in the dominant shoulder compared with the nondominant shoulder.20,45,47 IER was defined as a difference of <5° in ER between the dominant and nondominant shoulders. 44

Clinical assessment of shoulder range of motion. (A) Measurement of external rotation; and (B) measurement of internal rotation, both performed with the shoulder in 90° of abduction and the elbow flexed at 90°.
Assessment of Scapular Dyskinesis
Scapular examinations involved both static and dynamic observation of the prominence of the inferomedial, medial, and superior scapular borders during 3 to 5 elevations. 42 The presence of an abnormal pattern of scapular motion and position was considered dyskinesis. 42
Assessment of Isometric Strength
Isometric shoulder strength was assessed using a portable digital dynamometer (Micro FET 2; Hoggan Health Industries Inc), as illustrated in Figure 2.10,33 With the athlete in the seated position, the dynamometer was positioned 2 cm proximally to the wrist, and isometric strength was measured at 2 shoulder positions: 90° of abduction and neutral rotation (90°/0°) (Figure 2A); and 90° of abduction and 90° of ER (90°/90°) (Figure 2B). At each position, the athlete performed IR and ER against the resistance of the dynamometer, being instructed to gradually increase force to maximum effort over 2 seconds and maintain it for 5 seconds.10,33 The test was repeated 3 times, and the average strength, in Newtons (N), was recorded. Strength imbalance was defined as an ER/IR ratio less than 0.9 or greater than 1.0, with the shoulder at 90°/0°; and an ER/IR ratio less than 0.6 or greater than 0.85, with the shoulder at 90°/90°. 33

Isometric shoulder strength testing using a hand-held dynamometer. (A) Seated position; dynamometer secured 2 cm proximally to the wrist; shoulder at 90° abduction with neutral rotation (90°/0°). (B) Seated position; shoulder at 90° abduction with 90° external rotation (90°/90°).
Assessment of Humeral Retroversion
Humeral retroversion was assessed via ultrasound by a research radiologist (N.L.M.). The transducer was positioned on the athlete's anterior shoulder, parallel to the plane of the table and aligned perpendicular to the long axis of the humerus in the frontal plane. The humerus was then rotated so that the bicipital groove appeared in the center of the ultrasound image, with a line parallel to the horizontal plane connecting the apexes of the greater and lesser tubercles. A goniometer, pressed firmly against the ulna, recorded the forearm inclination angle relative to the horizontal plane. This angle represents an indirect approximation of humeral retroversion. 26
Decreased humeral retroversion, considered a risk factor, was defined as a difference of <9.6° in humeral retroversion between the dominant and nondominant shoulders. 32
MRI Assessment
MRI was performed using a 1.5-T scanner (Magnetom Essenza; Siemens Healthcare).
The following findings were considered significant changes on MRI: glenohumeral osteoarthritis (Samilson-Prieto grades 1 to 3) 17 ; partial-thickness rotator cuff tear; full-thickness rotator cuff tear; acromioclavicular joint arthritis grades II to IV according to the classification of Shubin Stein et al 35 ; superior labrum from anterior to posterior (SLAP) lesions grades 1 to 4 according to the classification of Snyder et al 36 ; fatty degeneration grades 1 to 4 according to the classification of Goutallier et al 16 and adapted for use with MRI by Somerson et al 37 ; long head of the biceps tendinopathy; subacromial bursitis; Bankart lesion; and Hill-Sachs lesion.
Statistical Analysis
Data were recorded in Microsoft Excel spreadsheets and analyzed using Jamovi software. The Shapiro-Wilk test was used to assess the normality of data distribution. Continuous variables are presented as mean with standard deviation if normally distributed or median (range) if not normally distributed. Categorical variables are presented as counts and percentages.
The association between risk factors and outcomes was analyzed using the chi-square test for categorical variables, Student t test for parametric continuous variables, and the Mann-Whitney U test for nonparametric continuous variables.
For risk analysis, the odds ratio (OR) and 95% CI were calculated to estimate the probability of an outcome in individuals exposed versus not exposed to risk factors.
Two multivariable binary logistic regression models and one multivariable linear regression model were constructed to identify the main variables capable of explaining the outcomes of interest. Initially, all risk variables were entered into the model. Then, statistical variable selection techniques were used based on the inclusion (forward stepwise selection: conditional likelihood ratio and Wald tests) and exclusion of variables (backward stepwise selection: conditional likelihood ratio and Wald tests). The Wald test was used to determine the significance of the regression parameters.
The level of significance was set at 5% for all analyses.
Results
Of the 111 athletes initially assessed for eligibility, 16 were excluded: 14 refused to participate in the preseason assessment, and 2 withdrew consent. This resulted in a final sample of 95 athletes for analysis (Figure 3).
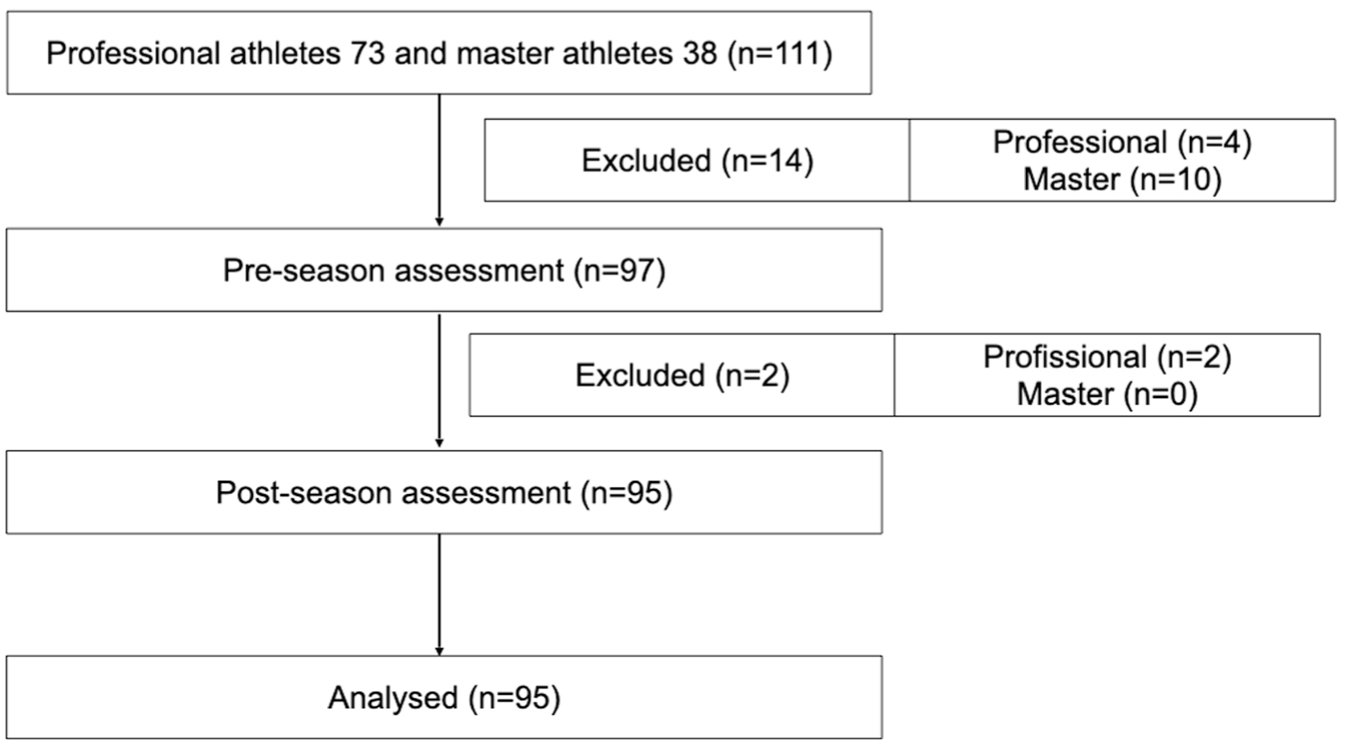
Flowchart detailing the study protocol.
Descriptive Analysis
The athletes’ mean age was 30.3 ± 9.0 years, ranging from 18 to 55 years. A total of 87 athletes (91.6%) were right-handed. The participants had a mean of 14.3 ± 7.1 years of volleyball experience, ranging from 3 to 40 years. Regarding training and game load, 43.2% of the athletes played volleyball for >16 hours per week, which was considered overload. The frequency of risk variables is shown in Table 1.
Frequency of Risk Variables (N = 95) a

Data are presented as n (%) unless otherwise indicated. GIRD, glenohumeral internal rotation deficit; TROM, total range of motion.
Regarding the outcomes at the end of the season, 50 athletes (52.6%) reported pain, 37 (38.9%) experienced injuries, and 45 (47.3%) exhibited dysfunction in the dominant shoulder.
Overall, the mean VAS score for pain was 2.3 ± 2.5, with no athlete rating his or her pain as 9 or 10. The mean ASES score was 84.5 ± 16.9, ranging from 50 to 100 points.
A total of 37 athletes (38.9%) developed dominant shoulder injuries and underwent MRI. Of these, 33 (89.2%) had injuries to the right shoulder and 4 (10.8%) had injuries to the left shoulder. The frequency of injuries is shown in Figure 4.

Magnetic resonance imaging diagnosis of dominant shoulder injuries in volleyball athletes. ACJ, acromioclavicular joint; GHOA, glenohumeral osteoarthritis; LHB, long head of the biceps tendon; RC FD, rotator cuff fatty degeneration; RCT, rotator cuff tear; SA, subacromial; SLAP, superior labrum anterior to posterior.
Association Analysis
The risk factors scapular dyskinesis (P = .001) and history of being sidelined due to shoulder injury (P < .001) were significantly associated with the outcome shoulder pain (Table 2). Age (P = .41), years of volleyball experience (P = .97), and the other risk factors showed no significant association (P > .05).
Association of Risk Factors With Dominant Shoulder Pain and Injury (N = 95) a
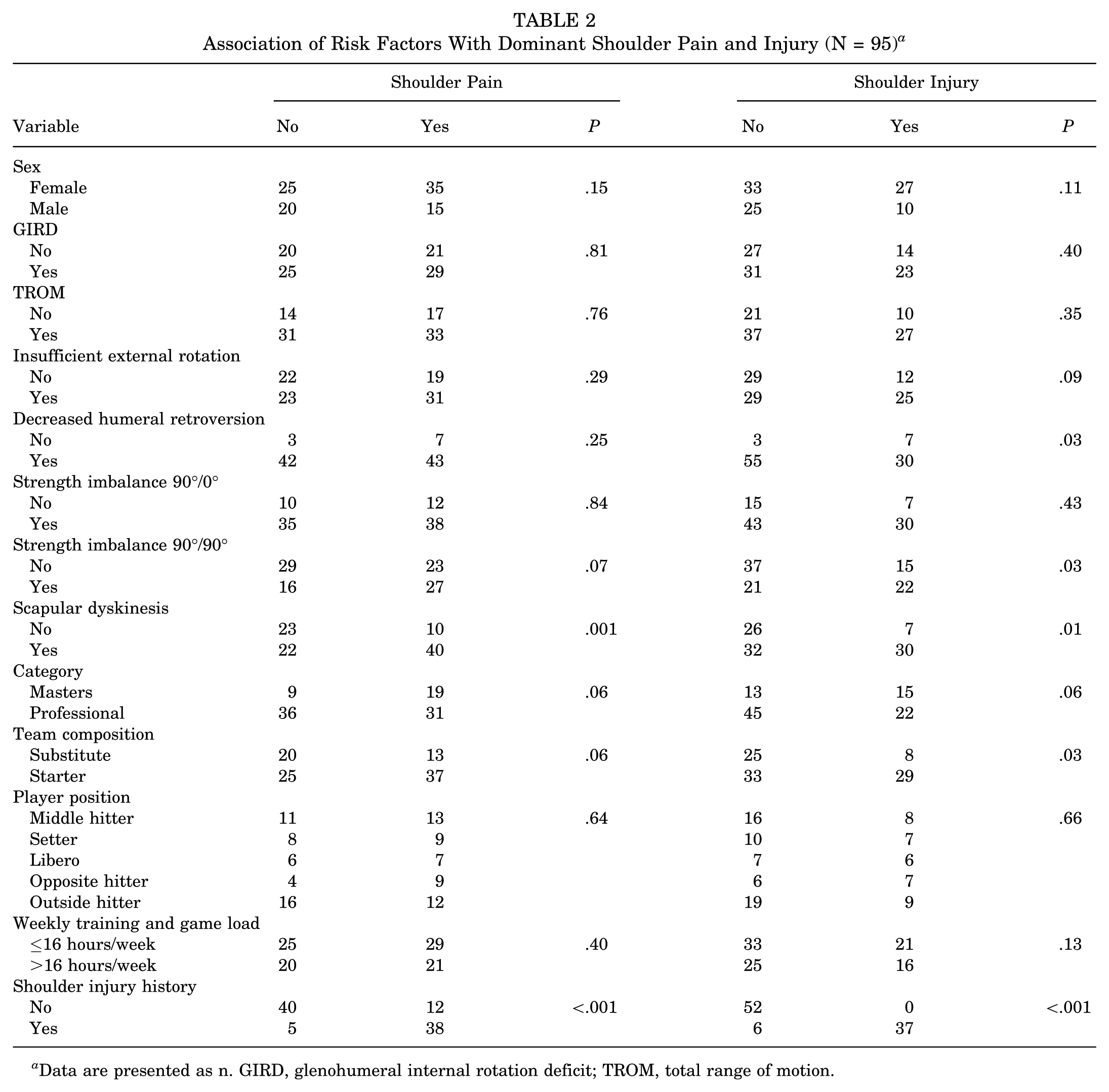
Data are presented as n. GIRD, glenohumeral internal rotation deficit; TROM, total range of motion.
Scapular dyskinesis (P = .01), strength imbalance at 90°/90° (P = .03), decreased humeral retroversion (P = .03), team composition (starter or substitute) (P = .03), and history of being sidelined due to shoulder injury (P < .001) were significantly associated with shoulder injury (Table 2). Age (P = .21), years of volleyball experience (P = .51), and the other risk factors showed no significant association (P > .05).
Athletes with scapular dyskinesis (P = .003), starters (P = .01), and those sidelined due to shoulder injury (P < .001) had significantly lower ASES scores. The other variables did not show significant differences in ASES scores (P > .05).
Risk Analysis
Athletes with scapular dyskinesis had 4.2 times greater odds of experiencing shoulder pain than those without this risk factor (95% CI, 1.7-10.4) (Table 3). Athletes with a history of shoulder injury had 25.3 times greater odds of experiencing pain than those without shoulder injury history (95% CI, 8.15-78.7) (Table 3).
Odds Ratio of Variables Significantly Associated With Shoulder Pain

Athletes with scapular dyskinesis had 3.5-fold increased odds of shoulder injury compared with those without this risk factor (95% CI, 1.3-9.2). A history of shoulder injury increased the odds of reinjury by 606 times (95% CI, 33.1-11085). Athletes with strength imbalance at 90°/90° had 2.6-fold increased odds of injury compared with those without strength imbalance (95% CI, 1.1-6.0). Starters had 2.7 times greater odds of sustaining shoulder injuries than substitutes (95% CI, 1.0-7.0). The presence of decreased humeral retroversion reduced the odds of injury by 80% (95% CI, 0.1-1.0) (Table 4).
Odds Ratio of Variables Significantly Associated With Shoulder Injury

Multivariate analysis: logistic and linear regression
Scapular dyskinesis (P = .04) and a history of shoulder injury (P < .001) were predictive of shoulder pain. The presence of scapular dyskinesis increased the odds of pain by 3.9 times (OR, 3.9; 95% CI, 1.08-14.14), while a history of shoulder injury increased these odds by 32.1 times (OR, 32.16; 95% CI, 8.31-124.46).
Strength imbalance at 90°/90° was also predictive of shoulder injury (P = .04), increasing the odds of injury by 34.3 times (OR, 34.33; 95% CI, 1.19-992.27).
Scapular dyskinesis (P = .04) and a history of shoulder injury (P = .001) were predictive of lower ASES scores. Scapular dyskinesis was associated with a reduction of 5.5 points on the ASES score (95% CI, -10.74 to -0.37), while a history of being sidelined due to shoulder injury was associated with a reduction of 23 points (95% CI, -28.11 to -18.01). A summary of the main results of this study is provided in Table 5.
Summary of Main Results a

ASES, American Shoulder and Elbow Surgeons.
Discussion
This study identified key clinical and biomechanical variables associated with shoulder pain, injury, and dysfunction in volleyball athletes. Scapular dyskinesis and a history of shoulder injury were the most consistent predictors, demonstrating significant associations with all 3 outcomes. Strength imbalance at 90°/90° was significantly associated with an increased risk of shoulder injury. Additionally, being a starter was linked to higher odds of both injury and dysfunction.
The results of this study align with existing orthopaedic literature, revealing a high incidence of pain, injury, and dysfunction in the dominant shoulder of volleyball athletes at the end of the season. The prevalence of shoulder pain in volleyball studies ranges from 23% to 50%,14,24 while the prevalence of shoulder injury ranges from 15% to 23%. 41 This is likely because of the high physical demands exerted on the arm by the repetitive and intense overhead movements inherent in volleyball, which can overload and damage muscles, tendons, and joints. 9
The most common injuries observed on MRI scans were subacromial bursitis, SLAP lesions, acromioclavicular joint arthritis, and partial-thickness rotator cuff tears. Notably, none of the athletes had glenohumeral osteoarthritis. This contrasts with the findings of Lee et al, 25 who reported a 50% prevalence of this condition in volleyball athletes evaluated by MRI. This discrepancy may be attributed to differences in sample characteristics or diagnostic criteria used. However, the frequency of rotator cuff, acromioclavicular joint, glenoid labrum, and long head of the biceps tendon disorders was consistent with existing literature, 25 supporting the validity of our findings. It is important to acknowledge that, because MRI scans were performed only after injury, some findings may reflect chronic, preexisting conditions aggravated by overuse during the season. These results highlight the importance of preseason screening and baseline assessment for early identification of shoulder lesions.
In the present study, age, sex, category, player position, training and game load, and years of volleyball experience were not identified as significant risk factors. However, starters had greater odds of experiencing shoulder injuries and had lower ASES scores than substitutes. This finding suggests a new area for further investigation. While previous research has suggested several potential risk factors for shoulder conditions in throwers, there remains a lack of consensus on this relationship.33,40 Previous studies have indicated that younger, 12 female,12,29,34 attacking,29,34 professional athletes,29,34,40 those with more years of volleyball experience,34,40 and those with greater training and game loads33,34,40 may be at greater risk of developing shoulder disorders. These conflicting results may be due to methodological heterogeneity between studies and the limited number of longitudinal studies available.
While our study found a high prevalence of GIRD, TROM, and IER, we did not identify a significant association with the analyzed outcomes. Shoulder ROM is considered crucial for normal movement mechanics, and significant ROM changes can alter glenohumeral kinematics and increase risks.2-5,20,22 Schmalzl et al 31 reported a 1.5-fold higher risk of impingement syndrome in volleyball players with GIRD than in those without GIRD, a relationship that we were unable to confirm in our study. The role of musculoskeletal adaptations in the occurrence of shoulder disorders remains controversial, and current evidence is insufficient to clearly distinguish physiological from pathological alterations.33,39,47
We demonstrated that imbalanced shoulder strength significantly increased the odds of injury, supporting existing literature. The importance of balanced ER and IR strength for normal shoulder function is widely recognized.6,11,12,29 Reeser et al 29 explained that imbalance between shoulder ER and IR strength should be considered a risk factor in volleyball. Fayão et al 12 reached a similar conclusion. Byram et al 6 highlighted that ER weakness increased the risk of injury requiring surgery in the dominant shoulder of athletes. Edouard et al 11 quantified the risk of dominant shoulder injury as 2.5 times higher for athletes with ER/IR imbalances. Our results are in line with this evidence and emphasize the value of routine shoulder assessments by isometric dynamometry for volleyball athletes.
Our results indicate that scapular dyskinesis is a significant risk factor for the analyzed outcomes. Altered scapular kinematics is often associated with subacromial and internal impingement syndromes, labral tears, and rotator cuff tears.2,20-22 Kibler et al 21 highlighted that scapular abnormalities are associated with shoulder pain and injury. Hickey et al 18 reported a 43% increased risk of a shoulder pain event in asymptomatic athletes with scapular dyskinesis. This relationship has also been confirmed by several studies on volleyball.29,30,34 Our findings further support this relationship and emphasize the importance of identifying scapular dyskinesis during athlete evaluation as part of a strategy to reduce the incidence of injuries throughout the season.
A history of being sidelined due to shoulder injury was identified as a significant risk factor for shoulder pain, injury, and dysfunction. In volleyball athletes, a history of previous shoulder disorders plays an important role in the recurrence of these problems.12,14,29,30,34,40 Forthomme et al 14 revealed that athletes with a history of shoulder pain had a 9 times higher risk of experiencing further pain. Fayão et al 12 highlighted that previous injuries should be considered a critical factor for new episodes of pain and injury. This is often because of structural and functional changes resulting from previous injuries, which can compromise normal biomechanics of the glenohumeral joint. These changes include joint stiffness, residual muscle weakness, and imbalances between dynamic and static stabilizers; and not only do they decrease the shoulder's ability to withstand the demands imposed by sport, but they also increase its susceptibility to further trauma. Therefore, rehabilitation strategies should focus not only on treating the initial injury but also on preventing future injuries by addressing muscle imbalances, recovering functional ROM, and optimizing movement mechanics.
This study revealed an unexpected finding: decreased humeral retroversion was associated with a lower risk of injury. It is known that throwing athletes develop greater humeral retroversion in their dominant shoulder as an adaptation to repetitive stress. 46 Theoretically, decreased humeral retroversion would result in less energy dissipation during throwing, increasing the stress on the shoulder and, consequently, the risk of injury.26,27,32,46 This hypothesis is supported by the literature. Pieper 28 suggested that athletes who do not have increased humeral retroversion may be at a higher risk for shoulder pain. Noonan et al 27 demonstrated that increased humeral retroversion is a protective factor against shoulder injuries in throwers. Schwab and Blanch 32 concluded that the dominant shoulder of volleyball players has, on average, a 9.6° increase in humeral retroversion compared with the nondominant shoulder. Our results contrast with this evidence. One possible explanation may lie in our assessment method. While ultrasound is a validated tool, it provides an indirect measurement of humeral retroversion. Future studies using computed tomography may clarify this discrepancy.
While caution is warranted when using clinical variables to predict risk, our results reinforce previously described associations between clinical variables and shoulder disorders in a sport-specific context, supporting their application in both preseason and postseason clinical assessments. Future research should confirm the predictive value of these variables and contribute to the development of more robust and individualized preventive strategies.
Limitations and Strengths
This study has limitations. The lack of randomization in the study group may have introduced selection bias. Also, no formal sample size calculation or power analysis was performed, as this study was based on a convenience sample of volleyball athletes who were available across 3 competitive seasons. Given the logistical challenges of prospectively enrolling high-level athletes, we included all eligible participants who met the inclusion criteria and consented to participate. Additionally, the heterogeneity of the participants may limit the generalizability of the results to the general population. The 8-month follow-up period may not have been sufficient to capture the true frequency of outcomes. The inclusion of both masters-level and professional athletes who, despite being potentially exposed to the same risk factors, have different training demands and loads, may have generated confounding bias due to variations in age, training hours, training days, and years of competitive practice. It is also important to acknowledge that the interaction between risk factors and the variability of exposure over time represents an inherent limitation of prospective cohort studies, with the potential to affect the robustness of our conclusions.
The strengths of this study include its longitudinal and prospective design, which allowed for a comprehensive assessment of participants, including medical history, physical examination, isometric dynamometry, goniometry, ultrasound, and MRI. The consistent assessment of all athletes by the same team and the analysis of established variables in the literature reinforce the reliability of the results. The use of standardized scales to measure the outcomes facilitates comparison and the use of these results in future research. Additionally, the analysis of all imaging studies by a single radiologist contributed to the consistency of the findings. These methodological practices demonstrate the rigor and care with which the study was conducted, seeking to ensure the reliability of its conclusions.
Conclusion
Our study revealed a high incidence of pain, injury, and dysfunction in the dominant shoulder of both masters-level and professional volleyball athletes. The most common injuries identified on MRI scans were subacromial bursitis (94%), SLAP lesions (73%), and acromioclavicular joint arthritis (62%). Notably, no athlete had glenohumeral osteoarthritis. Significant risk factors for shoulder pain, injury, and dysfunction included scapular dyskinesis and a history of shoulder injury. Additionally, starters had greater odds of experiencing shoulder injury and dysfunction. Imbalanced shoulder strength was also associated with an increased risk of injury. Conversely, decreased humeral retroversion was associated with a reduced risk of shoulder injury; however, this particular finding should be interpreted with caution because of potential confounding factors that may have affected this association.
Footnotes
Acknowledgements
The authors are grateful to the club president for granting permission to conduct this research. We also thank physical therapists, physical educators, coaches, and players for their availability and valuable contribution.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of Faculdade de Medicina da Universidade de São Paulo (No. CAAE: 50354521.1.0000.0068).