
Abstract
Background:
The rise in consumer-centric health insurance plans has increased the importance of the patient in choosing a provider. There is a paucity of studies that examine how patients select an orthopaedic sports medicine physician.
Purpose:
To evaluate factors that patients consider when choosing an orthopaedic sports medicine physician.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 1077 patients who sought treatment by 3 sports medicine physicians were administered an anonymous questionnaire. The questionnaire included 19 questions asking respondents to rate the importance of specific factors regarding the selection of orthopaedic sports medicine physicians on a scale of 1 (not important at all) to 10 (very important). The remaining 6 questions were multiple-choice and regarded the following criteria: preferred physician age, appointment availability, clinic waiting room times, travel distance, and medical student/resident involvement.
Results:
Of the 1077 consecutive patients administered the survey, 382 (35%) responded. Of these, 59% (n = 224) were male, and 41% (n = 158) were female. In ranking the 19 criteria in terms of importance, patients rated board certification (9.12 ± 1.88), being well known for a specific area of expertise (8.27 ± 2.39), and in-network provider status (8.13 ± 2.94) as the 3 most important factors in selecting an orthopaedic sports medicine physician. Radio, television, and Internet advertisements were rated the least important. Regarding physician age, 63% of patients would consider seeking a physician who is ≤65 years old. Approximately 78% of patients would consider seeking a different physician if no appointments were available within 4 weeks.
Conclusion:
The study results suggest that board certification, being well known for a specific area of expertise, and health insurance in-network providers may be the most important factors influencing patient selection of an orthopaedic sports medicine physician. Advertisements were least important to patients. Patient preferences varied regarding ideal physician age, clinic appointment availability, medical student/resident involvement, and travel distance in choosing an orthopaedic sports medicine physician. In the context of health care delivery and as reimbursement becomes increasingly consumer centered, understanding the process of provider selection is important.
Keywords
As the health care landscape continues to evolve, patients’ selection of a physician has become increasingly arduous and complex. The process of making this decision is often performed with minimal information from other health care consumers or providers. With the increasing prevalence of consumer-centric health plans (CCHPs), an understanding of patient decision-making criteria has grown in importance. CCHPs now constitute approximately 20% of the employer-based health insurance market and approximately 80% of the federal health insurance exchange market. 15 Besides enrolling patients in cost-sharing programs such as health savings accounts, CCHPs expand the role of the patient in health care decisions, including physician selection.
Although several studies have investigated criteria influencing patients’ selection of heath providers and plans, 6,7,9,14 few studies exist that examine how patients choose orthopaedic specialists, especially orthopaedic sports medicine physicians. Such factors are particularly relevant when considering the recent advancements that have furthered the use of ambulatory clinical care centers. Many of these centers are often independent of hospital systems and the coinciding referral networks, thereby allowing patients more independence in choosing a physician. Given the increasing prevalence of such stand-alone centers and the constancy of sports-related injuries that may warrant nonoperative or operative management, 17 the factors behind patients’ selection of an orthopaedic sports medicine physician are growing in relevance.
Numerous criteria guide patients’ selection of a medical specialist. Previous investigations have found that patients typically rely on referrals from their primary care physicians or on recommendations from friends or family. 14,25 In 1 study that surveyed 18,000 patients, 58% based their selection of a medical specialist solely on their primary care physician’s recommendation. 14 In a study of 251 patients seeking primary total joint arthroplasty from 1 orthopaedic practice, patients rated quality (ie, outcomes) and physician manner as most important. 6 A survey of 231 orthopaedic spine patients rated board certification as the most important criterion for provider selection. 20 In light of these findings, various metrics, including patient satisfaction ratings and outcomes data, have been introduced to assist patients in comparing and evaluating physicians. 6,12 Nevertheless, the criteria considered by patients when choosing an orthopaedic sports medicine physician are poorly defined.
The purposes of our study were (1) to identify the relative importance of 19 criteria that patients may consider when selecting a sports medicine physician and (2) to assess patient preferences regarding 6 other orthopaedic sports medicine physician characteristics (appointment availability, clinic proximity, waiting room times in clinic, preferred physician age, and resident/medical student involvement).
Methods
Following approval by our institutional review board (ORA No. 16052201), an anonymous questionnaire was administered to 1077 consecutive patients seeking treatment by 3 sports medicine physicians. To minimize bias resulting from treatment or evaluation, all surveyed patients who consented to participation completed the survey prior to their first clinic visit. The first portion of the survey consisted of 3 questions regarding the patient’s demographic information, including age, sex, and type of health insurance. The second part consisted of 25 questions regarding selection of an orthopaedic sports medicine physician. In 19 of these questions, respondents were asked to rate specific selection factors on a scale of 1 (not important at all) to 10 (very important). The other 6 questions featured multiple-choice responses regarding appointment availability, clinic proximity, waiting times in clinic, preferred physician age, and resident/medical student involvement. Content items for the survey were generated according to previous studies of physician selection criteria and our experiences. 6,13 Respondent ratings regarding each selection criterion were calculated via the mean and standard deviation for each item.
Results
Of the 1077 consecutive patients who were administered the questionnaire, 382 (35%) completed the survey. Of those completing the survey, response rates for each survey question ranged between 98% and 100%. Table 1 contains respondent demographic data. There was a slight majority of male participants (59% vs 41% females). Most respondents had private health insurance (85%) and were <50 years of age (58%).
Respondent Demographics as Reported on the Anonymous Survey a

a HMO, health maintenance organization; PPO, preferred provider option.
Table 2 lists the 19 selection criteria in descending order of patient ratings. The 3 factors rated highest by respondents when selecting an orthopaedic sports medicine physician were as follows: board certification (mean ± SD, 9.12 ± 1.88), being well known for a specific area of expertise (8.27 ± 2.39), and status as an in-network provider (8.13 ± 2.94). The 3 factors rated lowest by patients were all related to advertisement: radio (2.29 ± 2.23), Internet (2.28 ± 2.25), and television (2.17 ± 2.09).
Ratings of 19 Selection Criteria According to the Anonymous Patient Survey a
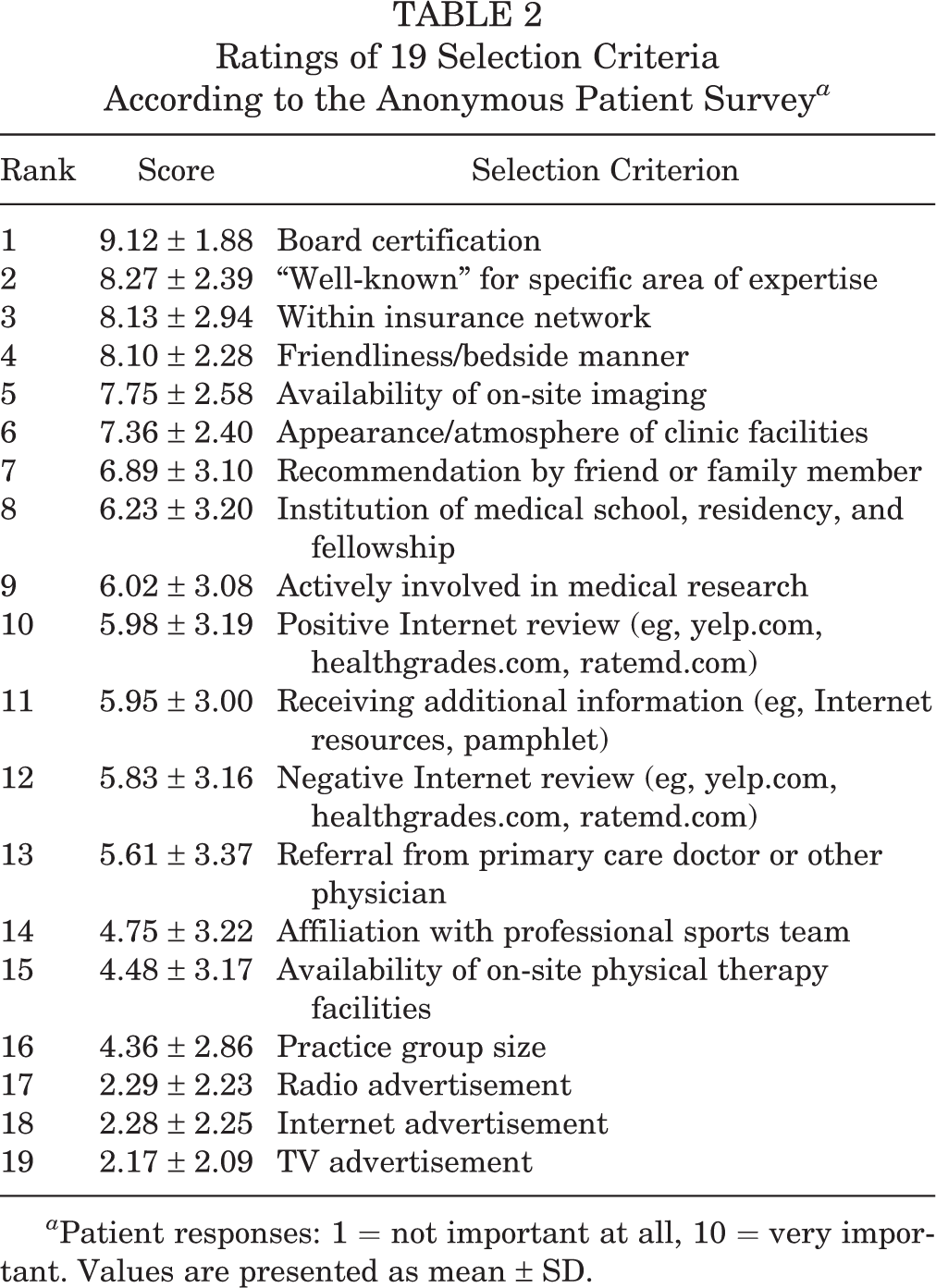
a Patient responses: 1 = not important at all, 10 = very important. Values are presented as mean ± SD.
Table 3 lists responses to the 6 multiple-choice questions. Regarding physician age, 63% of patients would consider seeking an orthopaedic sports medicine physician who is ≤65 years old. Approximately 80% of patients would consider seeking a different sports medicine physician if an appointment were not available within 4 weeks. Most patients (89%) reported that during a clinic appointment, no more than 30 minutes should lapse between check-in and seeing their physician. Most patients expressed no preference regarding involvement in their care by either medical students (68%) or residents (71%).
Responses From the Multiple-Choice Questions on the Anonymous Survey

Discussion
An understanding of the factors considered by patients when selecting an orthopaedic sports medicine physician is increasing in importance. This is especially pertinent as the prevalence of CCHPs continues to increase and health care reimbursement and delivery systems evolve into a more patient-centric paradigm. 15 In addition to changing patients’ financial considerations through health savings accounts, CCHPs will continue to increase the role of the patient in treatment decisions and selection of a provider. 16
Our results suggest board certification, being well known for a specific area of expertise, and health insurance in-network providers as the 3 factors of greatest importance to patients when choosing a sports medicine physician. Several other studies conducted in other medical specialties have demonstrated board certification as an important factor in primary care referrals. 9,10,19 Although initiatives for the reporting of physician quality continue to develop (eg, Physician Quality Reporting System by the US Centers for Medicare & Medicaid Services), board certification has been found to correlate with postoperative outcomes. 23 While any specialist physician in any country must have appropriate licensure to practice, board certification is not always required for medical licensure in the United States. Many licensed specialist physicians who practice in the United States are board eligible, meaning they have completed a residency in their specialty without successfully completing their specialty board examination. Clinical practice guidelines relating to whether a specialist in the US is board eligible or board certified are set by the American Board of Medical Specialties.
Historically, patients have also emphasized the importance of interpersonal skills (ie, bedside manner) when choosing a physician. Our patients rated this factor fourth highest, slightly below in-network insurance status (8.10 ± 2.28 vs 8.13 ± 2.94, respectively) (Table 2). A study by Bozic et al 6 of 251 patients found that interpersonal skills (ie, bedside manner) were the most important factor (even more so than physician quality; eg, outcomes) influencing provider selection for a total joint arthroplasty. Our findings also suggest that orthopaedic sports medicine patients value physician-patient interaction, despite orthopaedic surgeons’ tendency to focus on outcome measures and operative quality. Despite the increasing role of quality metrics in health care delivery and payment systems, developing the patient relationship remains important. 6
Despite spending on health care advertising having has diversified and increased, our patients rated television, radio, and Internet advertisements lowest among factors considered when choosing a sports medicine physician. Although there are minimal data regarding physician-to-patient advertising trends, our patients’ limited consideration of advertisements is noteworthy. This is especially interesting as commercial advertisements for “top-rated physicians” or the “most advanced hospital” can be readily found on various media outlets. 8 While board certification (rated highest by our respondents) could be considered a proxy for quality, a study of nearly 500 US hospitals in 2013 found that only 6% advertised information related to their quality outcomes. 22 Instead of formulating advertisements based on metrics for quality, many hospitals seem to compete primarily on factors relating to the patient experience, such as conveniences and amenities. 22 Interestingly, our patients rated being well known for a specific area of expertise as the second-most important factor in the selection of their sports medicine physician. It is unclear whether patients’ preference for an orthopaedic sports medicine physician who is well known and their disregard for advertisements (as suggested by our results) are mutually exclusive. Nevertheless, the impact of advertisements on physician selection warrants further investigation.
Patients gave middling ratings to online physician review platforms (eg, ratemd.com, yelp.com, healthgrades.com). Despite 80% of Internet users utilizing the Internet for comparison of health care options, 3 our study suggests that other patients’ online physician reviews are of limited importance as compared with other factors. In the context of optimizing patient feedback, online rating systems have potential as forums for information regarding physician quality. Critics of such Internet-based rating systems are concerned that they could become platforms for disgruntled patients to propagate dissatisfaction over minor shortcomings. They also worry that a physician’s reputation could become tarnished by a small number of negative online ratings. 11,18,21 Many websites for physician ratings have no requirements for verification of a user’s identity, which reinforces the concern for manipulation of ratings. Despite these potential flaws, the use of Internet-based systems for rating physicians is likely to increase.
Moderate ratings for recommendations from other physicians, friends, and family members (Table 2) are also a point of contrast with other studies. 14,25 In a survey of 1500 patients, Harris 14 found patients to be “passive consumers” in that they rely primarily on recommendations from other physicians, family, and friends when choosing a specialist. Although our study demonstrated moderate ratings for recommendations by word of mouth, other selection criteria may be the basis for such recommendations (eg, sports medicine physicians who are well known for a specific area of expertise and who are board certified may receive more word-of-mouth recommendations than sports medicine physicians who are not). In addition to our selection criteria, referral patterns by primary care physicians are often influenced by their personal and professional relationships with specialists.
Results from the multiple-choice questions also indicated several noteworthy patient preferences regarding an orthopaedic sports medicine physician. First, most patients preferred a lapse ≤30 minutes between checking into a clinic and seeing the physician. Patients may perceive the overall duration of their visit to a clinic as zero-sum, in which case wait times occur at the expense of appointment time with the physician. Although minimization of wait times is an important component of patient satisfaction and maintaining efficiency, time spent with the doctor remains more predictive of patient satisfaction than waiting room times. 2 Second, 63% of patients preferred an orthopaedic sports medicine physician who is ≤65 years old. In the context of orthopaedic sports medicine physicians who are performing surgery, the topic of when surgeons should retire has long been a point of debate. Anecdotal and objective evidence suggests that increasing surgeon age may contribute to diminished cognitive and physical performance. 5 However, a correlation between operative risk and a specific surgeon age remains unclear, as increasing surgeon age has been noted as a risk factor for some procedures (eg, coronary artery bypass grafting and pancreatectomy) but not others (eg, lung resection and esophagectomy). 26 Finally, patient preferences varied regarding appointment availability, clinic proximity, and resident/medical involvement.
This study had several potential limitations. First, survey respondents were patients of 3 sports medicine physicians at a single private practice in an urban location. Hence, the study findings may not represent all patients in other geographic regions and orthopaedic practices. Second, our survey asked patients to rate, rather than rank, the selection criteria. While ratings comparisons are useful in determining the degree to which patients may prefer one criterion over another, a lack of rankings limits determination of the order in which patients would designate the criteria. A longer survey with additional questions may have helped to further elucidate the impact of each criterion in patients’ decision making (eg, whether advertisements lead patients to look more closely at a hospital or physician before using their other criteria to make a choice). However, this was outside the goals of our study, which was to elucidate the relative importance of the various factors considered by patients when choosing a physician. The length of our survey was also in line with similar studies from other specialties. 6,20 Finally, the patients who completed the survey may not represent the general patient population. A literature review of additional survey studies of specialty patients revealed response rates that were higher (45%), 24 comparable (31%), 20 and lower (21%) 1 than ours (35%) or not reported. 4,6 Regardless, our study results represented a variety of age ranges from both sexes (Table 1).
Future studies could acquire results from multiple private and academic orthopaedic practices in varying geographic locations for greater generalizability. Although the focus of the present study was on the clinical setting, future studies could examine the role of similar criteria in patients’ selection of a surgery center. Further investigations may also examine patient utilization and perceptions of quality metrics when selecting an orthopaedic sports medicine physician.
Conclusion
Our findings suggest that being board certified and well known for a specific area of expertise may be most important to patients in selection of an orthopaedic sports medicine physician. Patient preferences varied regarding ideal physician age, clinic appointment availability, resident/medical student involvement, and clinic proximity when choosing a sports medicine physician. As paradigms of health care delivery and reimbursement become increasingly consumer-centric, understanding the process of physician selection will allow sports medicine physicians to better satisfy the expectations of patients. Our findings may offer guidance to orthopaedic sports medicine physicians as systems of orthopaedic care evolve.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.M.S. receives royalties from Nova Science Publishers and an honorarium from the Postgraduate Institute of Medicine. N.N.V. receives payment for lecturing from the Arthroscopy Association Learning Center Committee; receives payment for writing/reviewing manuscripts from Arthroscopy, SLACK Inc, and Vindico Medical-Orthopaedics Hyperguide; receives research support from Arthrex, Arthroscopy, Arthrosurface, DJ Orthopaedics, Smith & Nephew, Athletico, ConMed Linvatec, Miomed, and Mitek; is a consultant for Smith & Nephew and Minivasive; and holds stock/stock options in Cymedica, Minivasive, and Omeros. B.J.C. receives research support from Aesculap/B.Braun, Arthrex, Cytori, Medipost, Ossur, Smith & Nephew, Tornier, and Zimmer; is a paid consultant for Arthrex, Regentis, and Zimmer; receives royalties from Arthrex, DJ Orthopaedics, Elsevier, Saunders/Mosby Elsevier, and SLACK Inc; and has stock/stock options in Carticept and Regentis.
Ethical approval for this study was obtained from the institutional review board at Rush University Medical Center (ORA No. 16052201-IRB01).