
Abstract
Background:
The Hip–Return to Sport after Injury (Hip-RSI) score emphasizes the importance of psychological factors in return to sport (RTS) after arthroscopic treatment of femoroacetabular impingement.
Purpose/Hypothesis:
The goal of this study was to evaluate the reproducibility and validity of the Hip-RSI score for the assessment of the psychological readiness to RTS after surgical repair of a proximal hamstring avulsion in active patients, and the ability of the score to predict the return to preinjury sport at 9 months postoperatively. It was hypothesized that the Hip-RSI score is a reliable and valid tool for effectively assessing psychological readiness and predicting return to preinjury sport at 9 months after surgery.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Patients who underwent primary surgical repair of a proximal hamstring avulsion between June 2022 and November 2023 were included in this prospective cohort study. All patients completed the Hip-RSI score at 4 and 9 months postoperatively. The Hip-RSI score was compared with the Parisian Hamstring Avulsion Score (PHAS) for validation using the Pearson correlation coefficient. The discriminant and predictive abilities of the Hip-RSI score were also estimated. A test-retest method was used to assess the reliability of the scores, and internal consistency was evaluated using the Cronbach alpha coefficient.
Results:
A total of 84 patients (38 women and 46 men), with a mean age of 48.7 ± 12.7 years (range, 21-85 years), were included in the study. The Hip-RSI score was strongly correlated with the PHAS score (r = 0.55 [95% CI, 0.37-0.68]). The intraclass correlation coefficient was 0.89 (95% CI, 0.75-0.96), indicating good reliability of the score over time. The discriminant ability of the Hip-RSI score was good, as it was significantly higher in the RTS group than in patients who did not return to their preinjury sport. Furthermore, the predictive ability to identify patients who would return to their preinjury sport at 9 months postoperatively was acceptable (area under the curve = 0.76). At an optimal cutoff value of 51.7, the Hip-RSI score at 4 months had a sensitivity of 69% and a specificity of 77%, with a moderate Youden index of 0.46. The internal consistency suggested redundancy among the score items (alpha coefficient = .97).
Conclusion:
The Hip-RSI score is a valid, reproducible tool to assess the psychological readiness to RTS in active patients who undergo surgical repair of a proximal hamstring avulsion. This score, with a cutoff of 51.7 at 4 months postoperatively, demonstrated a moderate ability to predict which patients would return to sport, with a sensitivity of 69% and a specificity of 77%.
Hamstring injuries usually occur during sports, with most affecting the muscle itself or the myotendinous junction. They range from tendinopathies to complete proximal avulsion of the tendons from their insertion at the ischial tuberosity. Proximal avulsions are less frequent but more severe. 3 Two major mechanisms have been reported: acute eccentric overload, occurring during excessive lengthening under tension, such as during hip flexion combined with knee extension, and sprinting, when a sudden muscle contraction leads to injury.2,16,18 Given their effect on athletic performance, these often-neglected injuries must be correctly diagnosed and treated.10,13
Treatment success of proximal hamstring avulsions can be assessed using several scores, including the Parisian Hamstring Avulsion Score (PHAS), the Perth Hamstring Assessment Tools (PHAT), and the level of play. 15 Some of these scores, such as the PHAS, have been correlated with return to sport (RTS). 12 Although much attention has been focused on the postoperative RTS, these scores do not take into account a patient's psychological readiness to RTS. In 2008, Webster et al 21 developed the Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) score, composed of 12 items, to assess psychological readiness to RTS after anterior cruciate ligament reconstruction. Faleide et al 6 subsequently found, in 2021, that functional tests, including the International Knee Documentation Committee 2000 score and leg symmetry indices from hop and strength tests, did not predict RTS outcomes as effectively as the psychological readiness measures from the ACL-RSI. 6 This suggests that psychological readiness might be a more important factor in returning to sport than was traditionally thought.
The ACL-RSI score has been adapted for use in other sports-related injuries, such as hip pathologies (Hip-RSI).7,17 The Hip–Return to Sport after Injury (Hip-RSI) score has been validated for assessing psychological readiness to RTS after hip arthroscopy. 22
There are no existing tools to analyze psychological readiness to RTS after surgical repair of a proximal hamstring avulsion. The purpose of this study was to validate the Hip-RSI score as a tool to assess the psychological readiness to RTS after surgical repair of a proximal hamstring injury in an active population.
The hypothesis was that the Hip-RSI score could help discriminate and predict RTS after proximal hamstring reinsertion in athletes.
Methods
Study Design
This prospective cohort study included patients who underwent primary surgical repair of a proximal hamstring avulsion between June 2022 and November 2023. All included participants practiced at least 1 sport before the injury at various levels of play.
Sedentary patients, defined as not practicing any physical activity at all, those who underwent revision surgery, and/or who refused to participate in this study, were excluded from the study.
This study was approved by the institutional ethics review board of the Pitié Salpêtrière University Hospital (ID CPP-IDF6-19012012). Patient consent was obtained at the initial consultation.
Surgical Technique and Rehabilitation Protocol
Open repair was performed in all patients4,19 after the technique described by Lefevre et al. 9 The surgery involved a horizontal incision, in case of tendon retraction <4 cm, over the ischial tuberosity to expose the proximal hamstring tendon avulsion. Tendon reinsertion was achieved using 2 suture anchors in case of partial avulsion or 4 suture anchors in case of complete avulsion. Postoperatively, all patients were immobilized with the knee flexed at 30° to 45°, thereby limiting extension for the first 3 to 5 days after surgery. An articulated knee brace was used to allow free flexion and complete extension for 45 days. Full weightbearing with crutches was allowed immediately after surgery as tolerated, although limited by the knee being immobilized at 30° to 45° of flexion. A functional rehabilitation protocol, also described by Lefevre et al, 9 was initiated early on with isometric exercises for the quadriceps and hamstrings, with the knee bent at an angle of between 30° and 45°. Active rehabilitation was allowed after 6 weeks, including dynamic closed-chain quadriceps exercises and assisted active hamstring exercises. The patient could begin brisk walking or light jogging at between 12 and 16 weeks, and hamstring strengthening was continued with isokinetic and then eccentric exercises. Sports could be resumed after between 16 and 32 weeks.
Outcome Measures and Analysis
The goal of the Hip-RSI score, derived from the ACL-RSI, is to measure the psychological readiness to RTS in patients who have undergone surgery for hip pathologies. This score is based on 3 psychological factors related to the RTS: emotions, fear, and self-esteem. The score is obtained from a 12-item questionnaire, with each item using an 11-point scale (range, 0-10 points). The total score is calculated by adding the values of the 12 responses, then dividing by 1.2 to obtain a percentage. 22
This score was compared with the PHAS, another patient-reported outcome score. This 12-item scale has been validated for assessing functional outcomes after proximal hamstring avulsion surgery. Results range from 0 to 100; the higher the score, the better the outcome. 12
The primary outcome measure was the 4-month Hip-RSI score and its ability to predict RTS at 9 months. 11
The 9-month postoperative RTS was a secondary outcome measure, with patients indicating whether they had resumed their preinjury sport.
Data Collection and Follow-up
All patients were followed prospectively. A follow-up evaluation was performed 4 and 9 months after surgery. Patients completed, via an online questionnaire through the WebSurvey platform, the 12-item Hip-RSI score and the PHAS score at postoperative 4 and 9 months and reported whether they had returned to their preinjury sport at 9 months; if yes, at what level of play, according to the following categories: Occasional leisure (physically active individuals who practice sport sporadically, without a regular schedule), Regular leisure (regular noncompetitive sport participation, typically once per week or more), Competition (participation in organized competitive sports), and Professional.
Study Population
We included nonsedentary and first intention operated patients between June 2022 and November 2023 with a completed 9-month postsurgery Hip-RSI score. This population was used to analyze the discriminant and predictive ability of the Hip-RSI score for returning to the same preinjury sport at 9 months.
All patients’ characteristics included were obtained via an online questionnaire on the WebSurvey platform, completed by the surgeon for information on the lesion and by the patient for information regarding the sports practice.
Statistical Analysis
Variables were classified as either continuous or categorical. Continuous variables were first assessed for normality using the Shapiro-Wilk test. Depending on the distribution, parametric tests (eg, Student's t test) were used for normally distributed data, and nonparametric tests (eg, Mann-Whitney U test) were used for non-normally distributed data. Categorical variables were analyzed using the chi-square test or the Fisher test, as appropriate. For descriptive statistics, percentages were used for categorical variables, while the mean and standard deviation or the median and interquartile range (IQR) were used for continuous variables, depending on their distribution.
Validity
The validity of the Hip-RSI score was assessed by estimating the Spearman correlation coefficient between the score and the PHAS score. The degree of correlation (r) was defined according to the following guidelines: "strong" (r > 0.5), "moderate" (0.5 < r < 0.3), or "weak" (0.3 < r < 0.1). 14
Reliability
The intraclass correlation coefficient (ICC) was used to assess the test-retest reliability of the Hip-RSI score. The test-retest was performed on 20 randomly selected patients at 48-hour intervals. The ICC values were interpreted as follows 8 : “poor” for values <0.5, “moderate” between 0.5 and 0.75, “good” between 0.75 and 0.9, and “excellent” >0.9.
Internal Consistency
The correlation between the 12 items of the Hip-RSI score was measured using the Cronbach alpha coefficient, which evaluated internal consistency. An alpha coefficient >.90 suggests redundancy as a maximum value of 0.9 is recommended. 20
Floor and Ceiling Effect
Floor and ceiling effects were assessed by calculating the proportion of participants with minimum (0) or maximum (100) scores at 4 and 9 months. A floor or ceiling effect was considered to be present if >20% of the participants achieved these scores.
Score Progression
Scores were compared at 4 and 9 months using the paired Mann-Whitney-Wilcoxon tests because the variables of interest were not normally distributed according to the Shapiro-Wilk tests.
Discriminant validity
Mann-Whitney-Wilcoxon tests were also used to assess the discriminant ability of the Hip-RSI score at postoperative 4 or 9 months between patients who returned to their preinjury sport at 9 months (regardless of the level) and those who did not.
Predictive Capacity
The capacity of the 4-month Hip-RSI score to predict return to the same preinjury sport at 9 months (regardless of the level) was assessed using receiver operating characteristic curve statistics. The largest Youden index value (sensitivity + specificity – 1) was used to determine the ideal cutoff score for a safe RTS. Two predictive analyses were performed.
P < .05 was considered statistically significant.
All analyses were performed using R software Version 4.2 (R Foundation for Statistical Computing).
Results
During the study, 84 patients (38 women and 46 men; mean age at surgery, 48.7 ± 12.7 years) met the inclusion and exclusion criteria. Among these patients, 22.6% practiced sports at a competitive level before the injury, 63.1% exercised regularly, 9.5% exercised recreationally, and 4.8% were professional athletes. Additionally, 41.2% of patients underwent surgery for an acute injury (<4 weeks), and 84.5% for a complete rupture. Patient's characteristics are presented in Table 1.
Patient Characteristics a

IQR, interquartile range.
Occasional: the individual is physically active and practices sport sporadically, without a regular schedule. Regular leisure: regular noncompetitive sport participation, typically once per week or more. Competition: participation in organized competitive sports.
Of the 84 patients, 47 (56%) had returned to their preinjury sport at 9 months postoperatively, regardless of the level.
The Hip-RSI was found to be valid, as a significant and strong correlation was observed between the Hip-RSI and the PHAS scores at 9 months (r = 0.55 [95% CI, 0.37-0.68]; P < .001).
The ICC was 0.89 (95% CI, 0.75-0.96), indicating good reliability of the Hip-RSI score over time. The median Hip-RSI score was 58.75 (IQR, 47.29-74.17) for the first test and 58.75 (IQR, 46.67-73.13) for the retest.
To assess internal consistency, the Cronbach alpha was calculated and found to be 0.97, suggesting that the 12 items of the Hip-RSI score could be redundant.
No floor or ceiling effects were observed. At 4 months, 5% of participants scored the minimum value, and 0% scored the maximum value. At 9 months, 1% of participants scored the minimum value, and 1% scored the maximum value.
Regarding score progression, both the Hip-RSI and PHAS scores showed significant improvements between 4 and 9 months postoperatively (P < .001) (Table 2).
Scores of Interests at 4 Months Versus at 9 Months After Surgery (N = 84) a
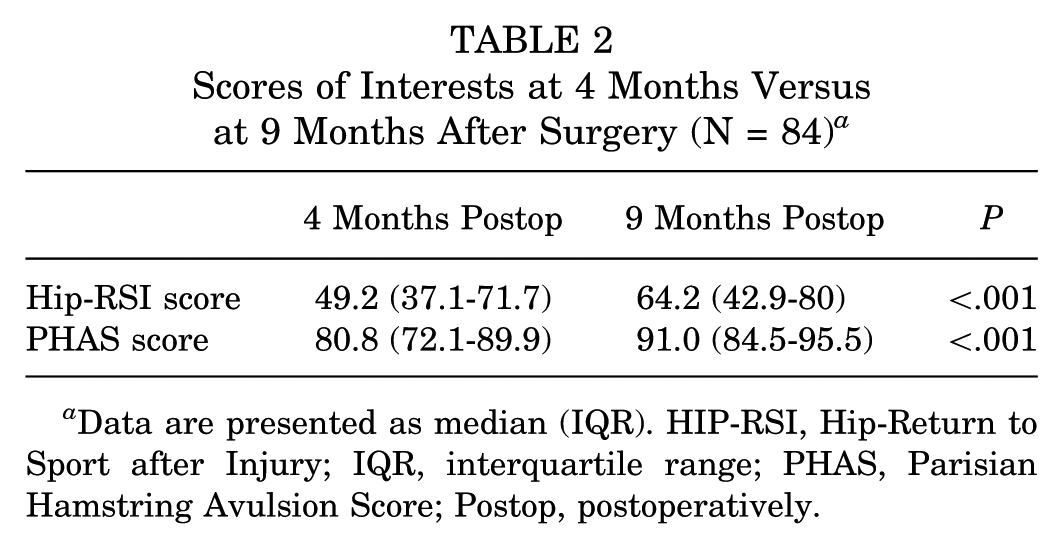
Data are presented as median (IQR). HIP-RSI, Hip-Return to Sport after Injury; IQR, interquartile range; PHAS, Parisian Hamstring Avulsion Score; Postop, postoperatively.
The Hip-RSI score was found to effectively discriminate between patients who returned to their preinjury sport and those who did not at both postoperative 4 and 9 months. At 4 months, the median Hip-RSI score was significantly higher in patients who underwent RTS (median, 57.5 [IQR, 45-79.2]) than in those who did not (median, 41.3 [IQR, 20.6-50.4]) (P = .001). Similarly, at 9 months, the median Hip-RSI score was 72.5 (IQR, 59.2-89.6) in patients who underwent RTS, compared with 42.5 (IQR, 25-60) in those who did not (P < .001) (Table 3). Notably, there was no improvement in Hip-RSI scores between 4 and 9 months among patients who did not RTS. In contrast, PHAS scores showed a significant increase over time even in those who had not resumed sport by 9 months (P < .001) (Table 3).
Discriminant Ability of Postoperative 4- and 9-Month Scores, for Return to the Same Preinjury Sport at 9 Months Regardless of the Level of Play (N = 84) a

Data are presented as median (IQR). Hip-RSI, HIP-Return to Sport after Injury; IQR, interquartile range; PHAS, Parisian Hamstring Avulsion Score.
The results showed that the predictive value of the 4-month Hip-RSI score was acceptable for returning to the preinjury sport at 9 months postoperatively, with an area under the curve of 0.76. The optimal threshold for the Hip-RSI score was 51.7%, with a sensitivity of 69% and a specificity of 77%, resulting in a Youden index of 0.46 (Figure 1).
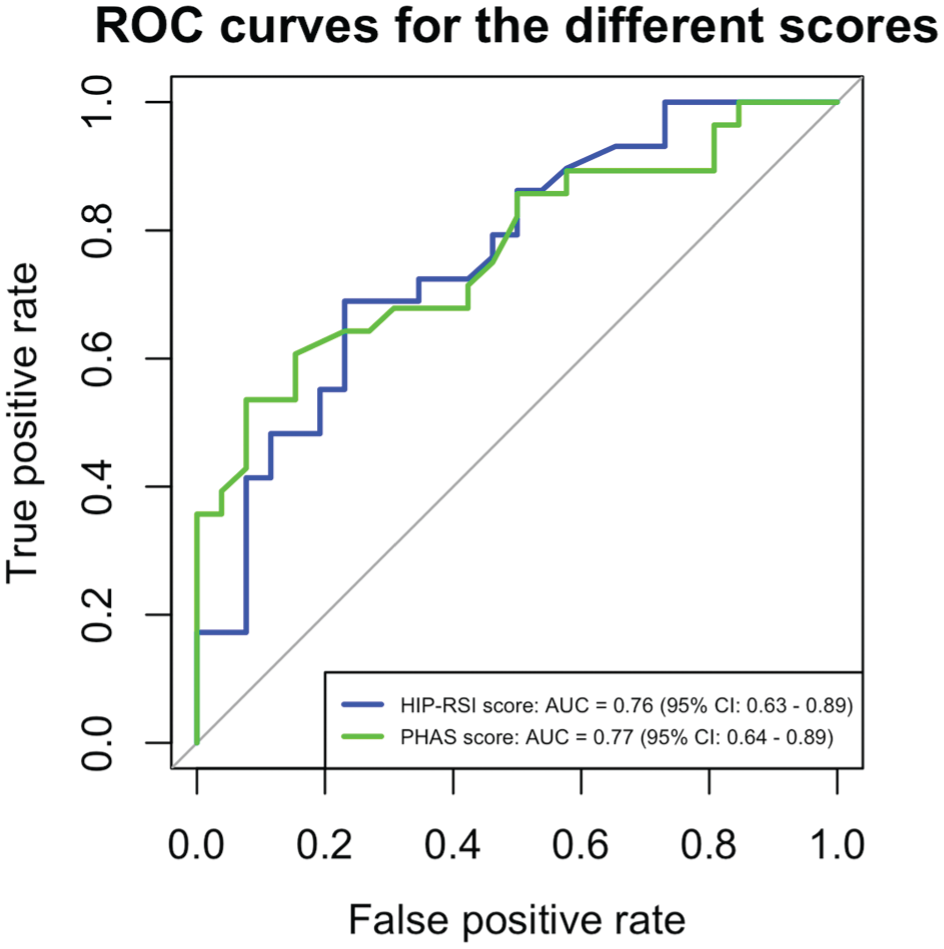
ROC curves showing the predictive ability of the Hip-RSI score compared with the PHAS score (N = 84). Hip-RSI, HIP-Return to Sport after Injury; PHAS, Parisian Hamstring Avulsion Score; ROC, receiver operating characteristic.
The PHAS score demonstrated a comparable predictive ability, with an optimal threshold of 87.3%, a sensitivity of 54%, and a specificity of 92%, also resulting in a Youden index of 0.46 (Table 4, Figure 1). This Youden index suggests that the Hip-RSI score has only a moderate predictive ability for RTS.
Optimal Thresholds for the 4-Month Hip-RSI and PHAS Scores to Predict Return to the Same Preinjury Sport at 9 Months Postoperatively Regardless of the Level of Play (N = 84) a

Hip-RSI, Hip-Return to Sport after Injury; IQR, interquartile range; PHAS, Parisian Hamstring Avulsion Score.
Discussion
The main finding of this study was that the Hip-RSI score is a valid and reliable score to identify psychological readiness to RTS in patients who undergo surgical repair for proximal hamstring avulsion. The Hip-RSI score demonstrated moderate discriminant and predictive validity, with a postoperative 4-month score threshold of 51.7% for a sensitivity of 69% and a specificity of 77% in predicting a return to the preinjury sport at 9 months postoperatively.
To the best of our knowledge, this is the first study to demonstrate the association between psychological readiness, according to the validated Hip-RSI score, and RTS after a proximal hamstring avulsion injury. Although the PHAS score has been validated for RTS in patients who have undergone surgical proximal hamstring avulsion repairs, it mainly focuses on physical recovery rather than the psychological aspects. For instance, in their systematic review, Reza et al 15 identified several types of patient-reported outcomes to evaluate the outcome of proximal hamstring avulsion treatment; however, PHAT was the only validated outcome measurement specifically designed for proximal hamstring injury at that time, and none targeted psychological factors. Numerous studies have shown that psychological factors, such as self-confidence and fear, significantly influence RTS after injury.1,14 Various scores exist and take into account these factors in other sports-related injuries, such as the Ankle Ligament Reconstruction–Return to Sport after Injury for ankle instability, the Shoulder Instability–Return to Sport after Injury for shoulder instability, and the ACL-RSI for knee instability.7, 17,21
In our study population, 56% (n = 47) of the patients returned to their preinjury sport 9 months after surgery. A review of the literature reported RTS rates ranging from 60% at 1 year after surgery to ≥75% in a mean time of 5.8 months (range, 1-36 months) after proximal hamstring tendon avulsion surgery.5,8 The higher rates observed in some studies may be explained by a longer follow-up period, larger sample sizes—as seen in meta-analyses—or by differences in surgical techniques and rehabilitation protocols. Further studies with longer follow-up and larger sample sizes could be performed to reassess the discriminant ability of the score.
Our results showed that a threshold of 51.7 (sensitivity, 69%; specificity, 77%) for the 4-month Hip-RSI score is a moderately accurate decision-making tool for predicting RTS at 9 months, regardless of the level of play, taking into account psychological factors, such as fear and self-esteem. Studies with 1- or 2-year follow-up could be performed to reassess this threshold and might result in even better sensitivities and specificities. Moreover, it could be interesting to take into consideration the type and level of sport, because RTS is significantly influenced by the type of sport, as shown by Lefevre et al. 13
The good reliability (ICC, 0.89 [95% CI, 0.75-0.96]) of our study shows that the Hip-RSI is a valid, reliable tool for assessing psychological readiness to RTS after proximal hamstring injury.
Nonetheless, this study has certain limitations, including the small sample size. Further studies with larger cohorts are necessary to investigate the changes in the Hip-RSI score after surgical treatment of proximal hamstring avulsions. A larger cohort could also allow us to study the predictive ability of the score according to the preinjury type of sport, which could lead to a more targeted estimation of RTS for each patient. Additionally, we lacked data on preinjury scores, as the score is relatively recent. Further studies could investigate whether a return to preinjury sport at 9 months is associated with the preoperative Hip-RSI score, as we believe psychological readiness to RTS after surgery may be linked to preinjury psychological factors, such as self-confidence. Also, we focused on predicting RTS regardless of the level of play at 9 months postoperatively. However, further studies exploring RTS according to the level of sport could be of interest. Because of our small sample size, we did not have sufficient patients in each stratum to perform this analysis. Another limitation is the high internal consistency (Cronbach’s alpha = .97), which suggests redundancy among the score items. Nevertheless, Wörner et al, 22 in their study validating the Hip-RSI score as a tool for assessing psychological readiness to RTS after hip arthroscopy, reported a similar Cronbach’s alpha of .96. They also found a Cronbach’s alpha of .90 for the Hip-RSI score when reduced to 6 items. Thus, further studies could explore a shorter, optimized version of the score.
Conclusion
The Hip-RSI score was found to have an acceptable discriminant ability and predictive value for assessing psychological readiness to return to the same preinjury sport in patients who underwent surgery for a proximal hamstring avulsion. These results support previous findings that show the effect of psychological factors on RTS after this type of injury. Therefore, the Hip-RSI is a valid and reliable tool for assessing psychological readiness to RTS. A threshold of 51.7 at 4 months postoperatively can be used as a moderately accurate decision-making tool for RTS at 9 months, with a sensitivity of 69% and a sensibility of 77%.
Footnotes
Final revision submitted July 1, 2025; accepted July 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.H. is a consultant for Arthrex and Depuy. N.L. is a consultant for Websurvey. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Pitié Salpêtrière University Hospital (ID CPP-IDF6-19012012).