
Abstract
Background:
Despite the prevalence of proximal hamstring avulsion injuries (PHAIs), the understanding of rerupture risk factors and the influence of injury chronicity on these rates remain limited.
Purpose:
To investigate the rerupture rate after PHAI repair and identify its associated risk factors and the optimal time to primary surgery.
Study Design:
Case-control study; Level of evidence, 3.
Method:
This is a retrospective analysis of prospectively collected data from the French Proximal Hamstring Avulsion Surgery Cohort Study targeting patients surgically treated for PHAI between 2002 and 2022. The primary outcome measure of this study was the rerupture rate of PHAI repair. The secondary outcome measures included the assessment of the potential risk factors for rerupture as well as the investigation of the incidence rate of rerupture for 100 person-years depending on various injury-surgery delay definitions.
Results:
This study analyzed 740 patients with a mean age of 45.9 years (SD, 13.6 years) and followed up for a mean of 4.9 years (SD, 3.9 years). The rerupture rate was 4.59% (34/740). Most reruptures (75%) occurred within the first 6 months after surgery (median, 88.5 days; interquartile range, 39.5-182 days), and 74% were atraumatic. Univariate analysis identified potential risk factors: longer initial surgery delay (hazard ratio [HR], 1.03; 95% CI, 1.01-1.04; P = .04) and initial complete ruptures (HR, 4.47; 95% CI, 1.07-18.7; P = .04). Receiver operating characteristic curve analysis found the optimal injury-surgery delay cutoff predicting rerupture to be 32 days (area under the curve, 0.62; 95% CI, 0.53-0.71). The relative Youden index was calculated at 0.24, corresponding to a sensitivity of 65% and a specificity of 59%. Surpassing this cutoff showed the highest HR (2.56), narrowest 95% CI (1.27-5.17), and highest incidence of rerupture (1.42 per 100 person-years) (P = .01). In the multivariate analysis, an injury-surgery delay of >32 days (HR, 2.5; 95% CI, 1.24-5.06; P = .01) and initial complete ruptures (HR, 4.33; 95% CI, 1.04-18.08; P = .04) emerged as significant risk factors for rerupture.
Conclusion:
This study found a 4.59% rerupture risk after PHAI repair. Most reruptures (75%) occurred within the first 6 months after surgery. Risk factors for rerupture included chronicity and initial complete injury. The optimal threshold for chronicity of PHAI lesions, based on rerupture rate, was marked by an injury-surgery delay of >32 days.
The proximal hamstring avulsion injury (PHAI) is a debilitating injury that is increasingly identified in athletes and nonathletes alike.8,12,14 This injury typically results from a forceful flexion of the hip associated with a full extension of the knee and is more pronounced in sports that need acceleration, such as football and rugby.9,11,14 Notably, Ekstrand et al 11 showed an annual increase of 4% of hamstring injuries in professional football within 13 years. Despite often presenting with explicit clinical signs, these lesions can be underdiagnosed or have their diagnosis delayed. 3 Magnetic resonance imaging (MRI) is the standard imaging for the diagnosis of PHAI.8,10,21,27
The treatment of PHAI depends on the degree of retraction, type of tear (partial or total), chronicity of the lesions, and associated symptoms. 6 Studies have emphasized the benefits of early surgical treatment, leading to satisfactory results and improved functional outcomes.2,8,13,16,25 However, the literature does not support a clear definition of chronicity. Some authors have defined chronicity as a delay of >4 weeks and divided patients in the analyzed study into acute (<4 weeks) and chronic (>4 weeks) groups.15,16,25,26 van der Made et al 21 described it as acute (<8 weeks) and delayed (>8 weeks). Belk et al 2 described it as early surgery (<1 month), delayed surgery (1-6 months), and late surgery (>6 months). They demonstrated that the early-surgery group showed the earliest and highest rate of postoperative return to sport. Sarimo and colleagues 19 established categories for injury-surgery delay based on patient outcomes. They defined 3 categories: early surgery (<3 months), delayed surgery (3-6 months), and late surgery (>6 months). The authors found that the risk of a moderate or poor result was much higher in patients who underwent late surgery. 19
Complications of surgical treatment include hematoma, surgical-site infection, compressive hematoma, sciatic nerve damage, and rerupture.3,13,25 One of the largest meta-analyses conducted on the subject, by Hillier-Smith and Paton, 13 included 35 studies and 1530 patients and showed a significantly lower overall rate of complication if treatment was acute (with “acute” being defined arbitrarily as treatment within 4 weeks of injury because of the absence of a medical consensus). 8 The rerupture rate was 1.2% overall, with a lower rate for acute (0.2%) than for chronic injuries (1.0%). There was no significant difference between partial and complete injuries. However, postoperative sciatic nerve symptoms were more prevalent in chronic repairs (5.1%) and complete injuries (3.6%). 8 To the best of our knowledge, no study to date has primarily investigated the rerupture rate and risk factors after PHAI as the main outcome measure.
The primary aim of the study was to investigate the rerupture rate after PHAI repair. The secondary aim was to evaluate rerupture variables (such as timing and mechanism of injury), investigate potential risk factors for rerupture, and assess the incidence rate of rerupture for 100 person-years depending on various injury-surgery delay definitions, with the specific aim of identifying the critical time delay after injury that defines the chronicity of PHAI.
Methods
Study Design and Inclusion Criteria
This single-center cohort study conducted a retrospective analysis of prospectively collected data from the French Proximal Hamstring Avulsion Surgery Cohort Study (ClinicalTrials.gov identifier: NCT02906865) between January 2002 and July 2022.
The study included all patients who underwent primary surgical repair of PHAI with a minimum follow-up of 12 months. Patients who had a bony avulsion of the ischial tuberosity, required a reconstruction using an autograft or allograft, or underwent previous surgeries on the hamstring were excluded.
This study was approved by the local institutional ethics committee. After the decision for surgical intervention, each patient provided informed consent to participate in the study.
Surgical Technique and Postoperative Rehabilitation Protocol
Indications for the initial surgery included all patients with complete avulsions or those with partial avulsions who had >2-cm retraction or were persistently highly symptomatic for pain and weakness compared with the contralateral side. If patients who initially underwent nonoperative management developed these indications—particularly increased retraction in partial avulsions or escalating symptoms—they were subsequently evaluated for surgical intervention.
All patients were operated on under spinal anesthesia by senior surgeons following the surgical technique described by Lefèvre et al. 16 The majority of the surgeries were performed by the senior author (N.L.). A smaller portion of the procedures were carried out by 2 other senior surgeons from the same staff team (A.H. and Y.B.).
Postoperatively, patients used an articulated knee brace set to a 40° extension block for 3 weeks.
The rehabilitation strategy was aligned with the protocol delineated by Lefèvre et al. 16 Initially, isometric strengthening exercises for the quadriceps and hamstrings were executed while maintaining knee flexion at 30° to 45°. Each week, an extra 10° of extension was permitted. Full weightbearing was initiated at 6 weeks. Passive rehabilitation began early, with active rehabilitation starting after 6 weeks. By the conclusion of the 6th week, the regimen was progressed to include dynamic quadriceps exercises in a closed-chain formation and active-assisted exercises for the hamstring muscles. Between the 12th and 16th weeks, patients were permitted to engage in brisk walking and potentially light jogging, with a focus maintained on enhancing hamstring strength through isokinetic exercises, before transitioning to eccentric exercises. From the 16th to the 32nd week, a return to typical sporting activities was generally achievable for the athletes.
In the management of delayed complete avulsions, the protocol entailed careful adhesiolysis to free the tendon, followed by assessing its mobility. If the tendon exhibited excessive tension, an Achilles tendon allograft was used to restore its length.
Outcome Measures
The primary outcome measure was the rerupture rate after PHAI repair. The secondary outcome measures included the assessment of other rerupture variables (timing and mechanism of injury), investigation of the potential risk factors for rerupture, and evaluation of the incidence rate of rerupture for 100 person-years depending on various injury-surgery delay definitions, with the specific aim of identifying the critical time delay after injury that defines the chronicity of PHAI. The decision on the optimal cutoff was based on 3 key variables: the highest hazard ratio (HR), the highest incidence of rerupture, and the narrowest confidence interval, each of which had to be statistically significant.
We categorized delays based on existing literature definitions: acute (injury-surgery delay <28 days) and chronic (>28 days),15,16,25,26 acute (injury-surgery delay <45 days) and chronic (>45 days),6,14 acute (injury-surgery delay <8 weeks) and delayed (>8 weeks), 21 early surgery (<3 month) and delayed surgery (>3 months), 19 and early or delayed surgery (≤6 months) and late surgery (>6 months).2,19 Other definitions include the following:
Three-category definition by Belk et al 2 : time to surgery ≤4 weeks, 4 weeks < time to surgery ≤ 6 months, and time to surgery >6 months
Three-category definition by Sarimo et al 19 : time to surgery ≤4 weeks, 4 weeks < time to surgery ≤ 12 weeks, and time to surgery >12 weeks
Cutoff according to tertiles: time to surgery ≤18 days, 18 days < time to surgery ≤ 44 days, and time to surgery >44 days
Hypothetical cutoff at 2 weeks: time to surgery ≤14 days versus time to surgery >14 days
Definition of Rerupture
Rerupture was defined as the recurrence of an injury at the same location and site as the initial injury. The diagnosis of rerupture was based on MRI 23 in symptomatic patients. Clinical characteristics of a rerupture included a deterioration in symptoms after a symptom-free interval, as well as a deterioration in functional and clinical tests, a modification of rehabilitation or training for >48 hours, and time lost from training or match play. This definition is based on the methodology suggested by the systematic review conducted by van Heumen et al. 22
Unless they became symptomatic earlier, all patients systematically underwent hip MRI at 6 months postoperatively to evaluate for repair integrity.
When rerupture occurred, nonoperative treatment was offered before surgery. The criterion for not responding to nonoperative treatment was based on insufficient symptom or function improvement after nonsurgical methods (rehabilitation, nonsteroidal anti-inflammatory drugs, painkillers, activity modification, and rest), with symptoms still affecting daily activities. This evaluation integrated clinician assessment and patient feedback.
Partial avulsion was defined as the involvement of either the conjoint tendon or the semimembranosus tendon, while complete avulsion referred to the involvement of both the conjoint tendon and the semimembranosus tendon. 13
Data Collection
Data were collected prospectively using the internet-based software WebSurvey, which was accessed and completed by both surgeons or fellows (for physical examination, imaging, and surgical findings) and patients (for descriptive characteristics and scores). The collected data included the characteristics of the study population, such as age, sex, body mass index (BMI), level of sport, accident circumstances, time to surgery, type of rupture, number of tendons involved, and tendon retraction on MRI scans. Data related to the surgical technique were also collected.
Participants and Sample Size
During the study time frame, 912 patients were operated on; of them, 100 were excluded (24 with bony avulsion, 32 with revision surgery, and 44 with allograft/autograft). Of the 812 remaining patients, 72 (8.9%) were lost to follow-up. The final study sample size was therefore 740 patients (Figure 1).
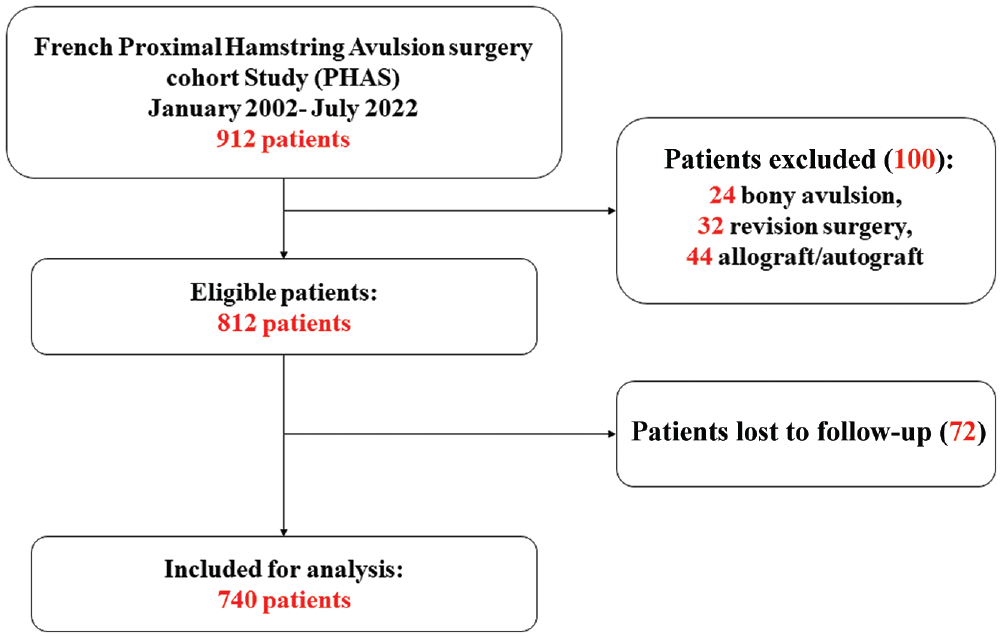
Flowchart of the study.
Statistical Analysis
Descriptive statistics were computed, including frequencies and percentages for categorical variables. For continuous variables, the mean and standard deviation were reported if they followed a normal distribution, as confirmed using the Shapiro-Wilk test. In cases in which the continuous variables did not exhibit normality, they were described using the median and interquartile range (IQR). Comparisons between the 2 groups were made using either the Student t test or the Wilcoxon rank-sum test for continuous variables and chi-square test or Fisher exact test for categorical variable, depending on the sample size.
To determine the optimal threshold of the delay between the accident and the surgery in relation to the primary outcome of interest, rerupture, we used a receiver operating characteristic (ROC) curve and the Youden index.
Kaplan-Meier survival curves were performed to evaluate the survival probability of rerupture between the 2 groups and were compared using the log-rank test, using time in years as the time scale.
The incidence rate per 100 person-years was calculated by dividing the number of new cases of rerupture observed during the study period by the total person-years at risk and multiplying the result by 100 to express the rate per 100 person-years.
Analysis of risk factors was conducted using a multivariate Cox proportional hazards model to estimate the HRs and 95% CIs of the risk factors associated with the outcome of interest. Before fitting the multivariate model, we identified potential confounding variables using univariate Cox regression analyses. Variables with a significant association with the outcome at a P value <.10 were included in the multivariate Cox regression model. A backward stepwise method was used to eliminate nonsignificant variables from the model, with a threshold of P < .05 for retention in the model.
The final multivariate model included only the variables that were significantly associated with the outcome, and the proportional hazards assumption was tested using the Schoenfeld residuals, which were found to be valid. Multicollinearity was checked using variance inflation factors, and no evidence of collinearity among the covariates was found. Statistical analyses were performed using R software, Version 4.2 (R Foundation for Statistical Computing) with a 2-tailed significance level of P < .05.
Results
Patient Characteristics
The study population of 740 participants had a mean age of 45.9 years (SD, 13.6 years) and consisted of 56.2% men and 43.8% women. In terms of rupture type, 21.5% were partial while 78.5% were complete. The mean tendon retraction on MRI scans was 4.8 cm (SD, 2.7 cm). The median time to surgery was 26 days (IQR, 15-62 days). The mean follow-up period was 4.9 years (SD, 3.9 years) (Table 1).
Characteristics of the Study Population a
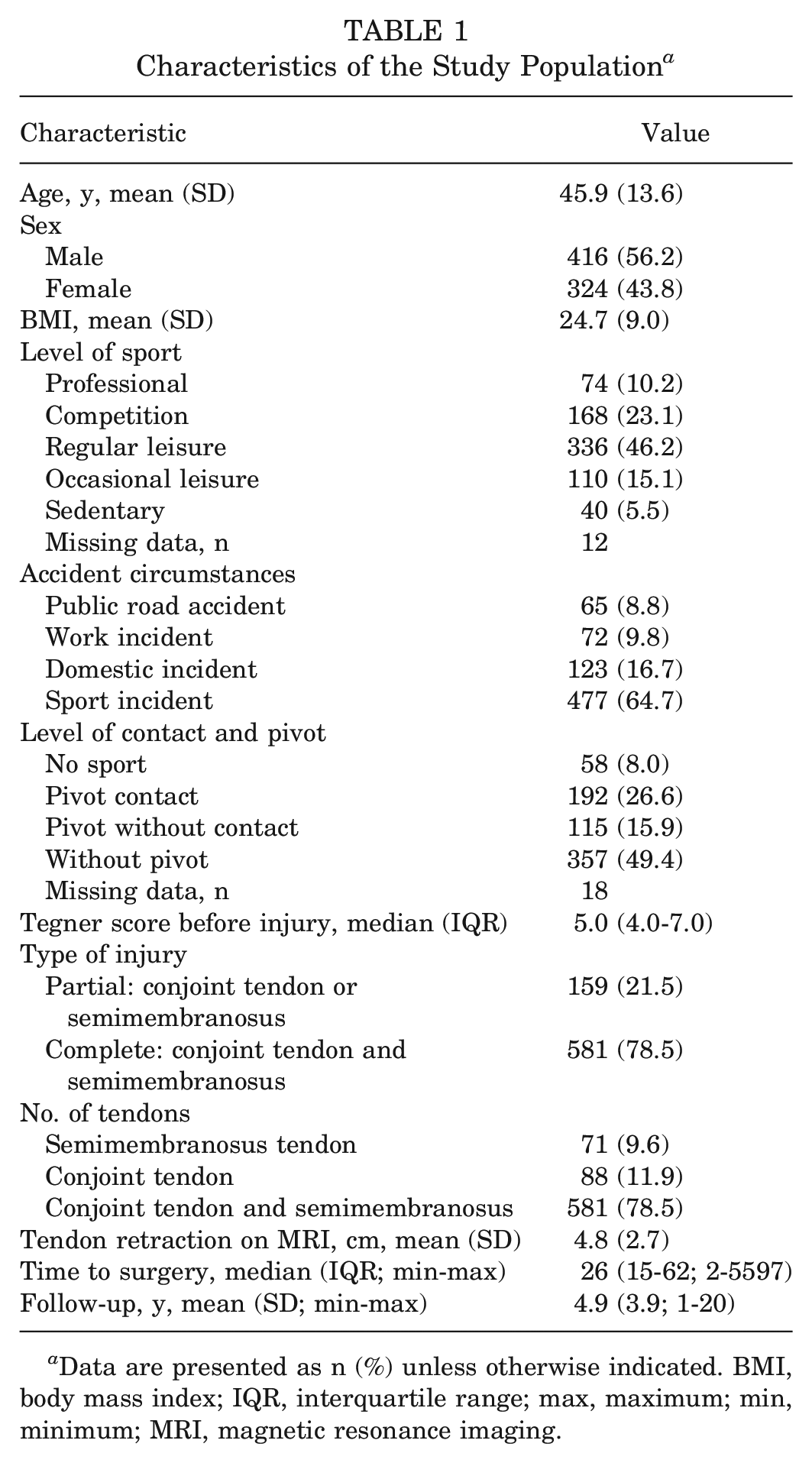
Data are presented as n (%) unless otherwise indicated. BMI, body mass index; IQR, interquartile range; max, maximum; min, minimum; MRI, magnetic resonance imaging.
Rate, Timing, and Cause of Rerupture
The rate of rerupture, confirmed clinically and via MRI scans, was 4.59% (34/740). Overall, 74% (25/34) of reruptures manifested within the first 6 months after surgery, and only 3 (8.8%) reruptures occurred beyond the first year. The median surgery-rerupture delay was 88.5 days (IQR, 39.5-182 days; range, 1-1517 days). Among the reruptures, 25 (74%) were atraumatic and 9 (26%) were cases of new trauma. Of the 34 reruptures, the majority were initially complete ruptures. Specifically, 1 case involved the conjoint tendon, and another involved the semimembranosus tendon. Not all reruptures necessitated surgery, with 32.4% (11 patients) responding to nonoperative treatment.
Other Complications
Other complications occurred in 28 patients (3.7% of total cases), including local wound inflammatory reactions and local noncompressive hematomas (3 patients each), compressive hematoma (4 patients), and sensory signs in territories of the sciatic nerve (1 patient) and pudendal nerve (7 patients). Motor sciatic nerve palsy was noted in 1 patient. Additionally, partial fixation detachment or cyst formation at the reinsertion site was observed in 3 patients; deep venous thrombosis, in 4 patients; and infection, in 2 patients.
Univariate Analysis of Potential Risk Factors
There were no significant differences in age, sex, BMI, level of sport participation, or accident circumstances between the 2 groups (Table 2).
Univariate Analysis of Potential Risk Factors of Rerupture a
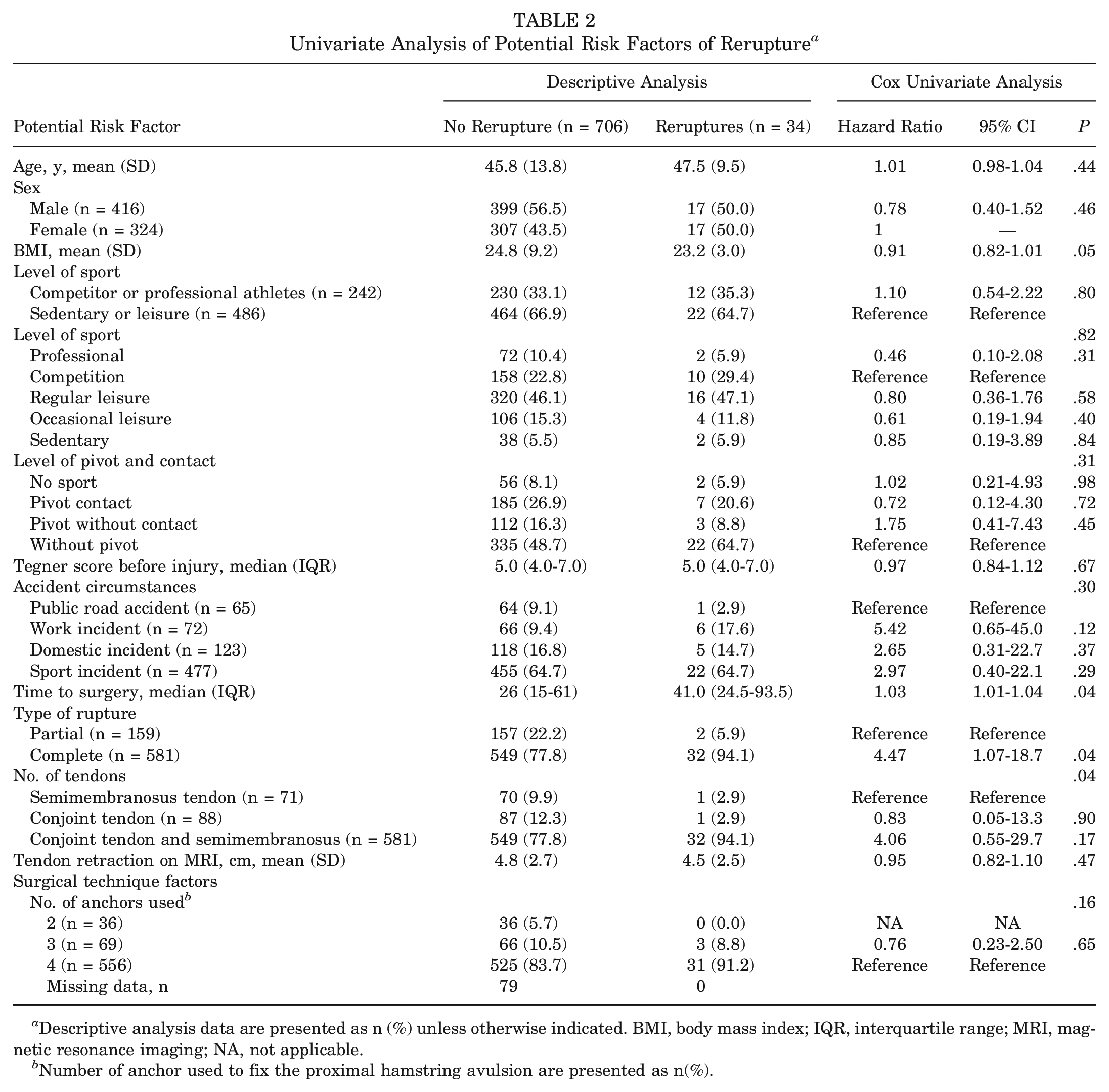
Descriptive analysis data are presented as n (%) unless otherwise indicated. BMI, body mass index; IQR, interquartile range; MRI, magnetic resonance imaging; NA, not applicable.
Number of anchor used to fix the proximal hamstring avulsion are presented as n(%).
However, patients who had a significantly longer injury-surgery delay (41.0 days [IQR, 24.5-93.5 days] vs 26 days [IQR, 15-61 days]; P = .04) were more likely to experience rerupture. This factor was associated with an HR of 1.03 (95% CI, 1.01-1.04; P = .04).
Furthermore, complete ruptures were more common in the rerupture group (HR, 4.47; 95% CI, 1.07-18.7; P = .04).
Assessment of Various Injury-Surgery Delay Definitions and Their Effect on Rupture
ROC Curve
The optimal cutoff point, predicting rerupture, derived from the ROC curve analysis was 32 days (area under the curve [AUC], 0.62; 95% CI, 0.53-0.71). The Youden index was calculated at 0.24, which, although relatively low, was still indicative of discriminatory capability because the AUC interval did not include the value of 0.5. This index corresponded to a sensitivity of 65% and a specificity of 59% (Figure 2).
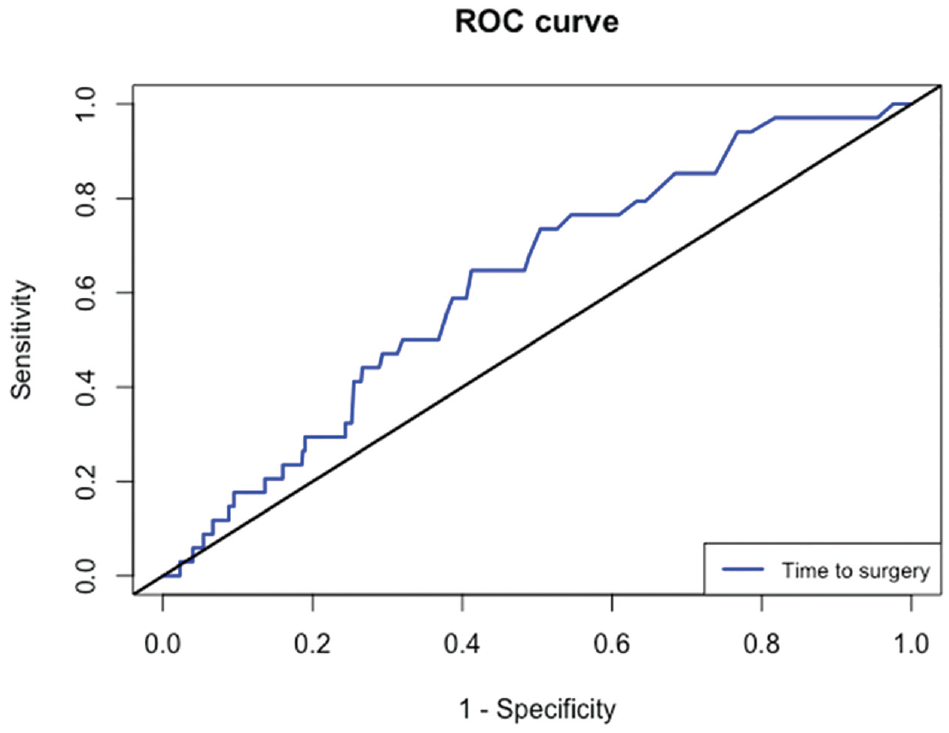
Receiver operating characteristic (ROC) analysis for rerupture prediction using time to surgery as the predictor.
Cox Regression Analysis
Among the tested cutoff points, those who underwent surgery beyond 14, 28, and 32 days experienced significantly higher risk of rerupture, with HRs of 4.79 (95% CI, 1.15-20.0), 2.09 (95% CI, 1.03-4.22), and 2.56 (95% CI, 1.27-5.17), respectively (P≤ .01). This increased risk trend continued for those who had surgery after 45 days, although the results were not statistically significant (all P > .05). Last, according to the tertile cutoff, those who had their surgery after 44 days had a significantly higher risk of rerupture, with an HR of 2.63 (P = .03) (Table 3).
Comparison of Rerupture Rates and Hazard Ratios Based on Different Time to Surgery Cutoffs a
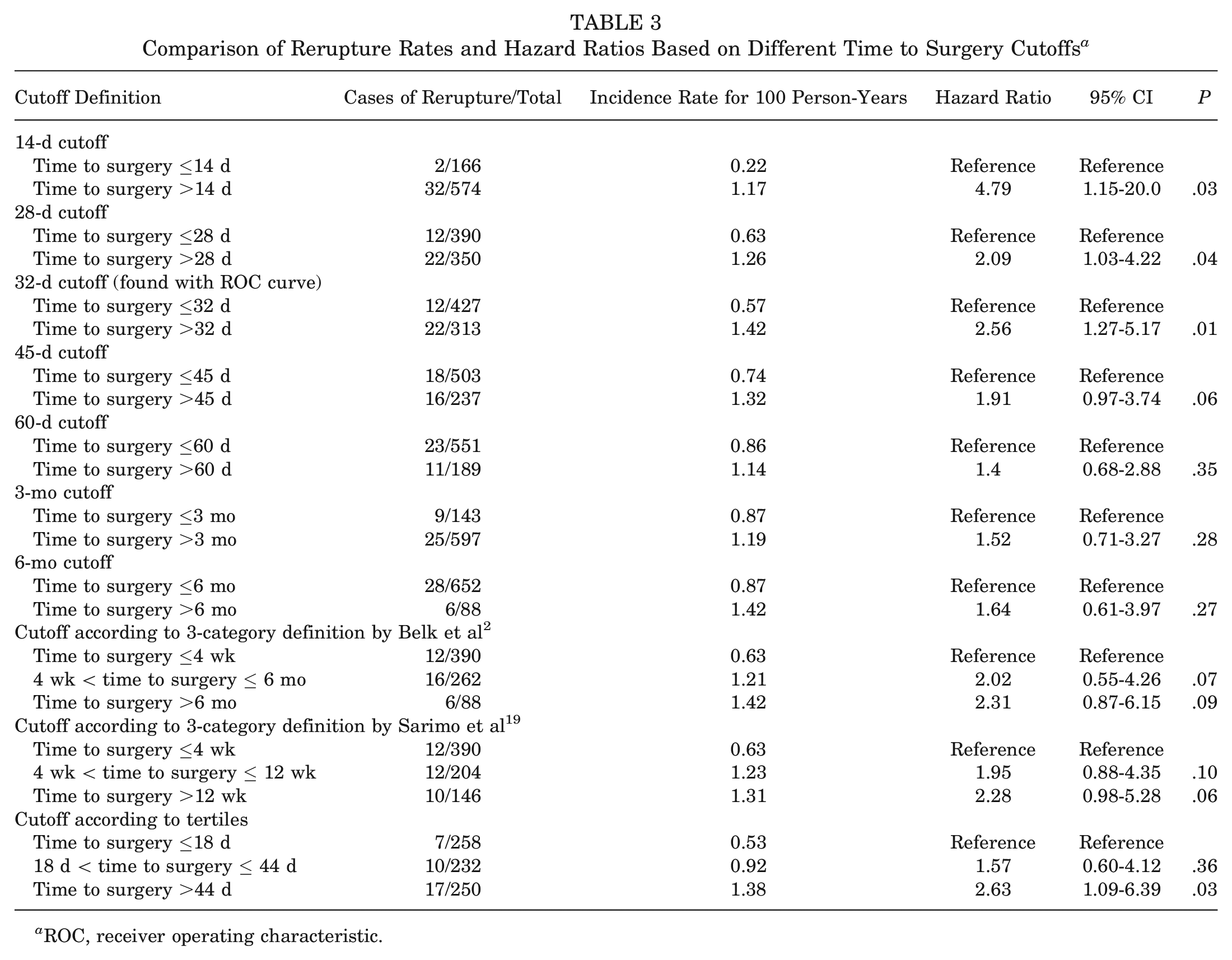
ROC, receiver operating characteristic.
Based on the results from the Cox regression analysis, the optimal cutoff point, characterized by the highest HR (2.56), the highest incidence of rerupture (1.42 per 100 person-years), and the narrowest 95% CI (1.27-5.17), was identified as a delay of 32 days before surgery (P = .01; Youden index, 0.24; sensitivity, 65%; specificity, 59%).
Kaplan-Meier Curve
The Kaplan-Meier survival curves with a 32-day threshold showed a statistically significant divergence in rerupture rates between the 2 groups (log rank test; P = .007) in favor of the early-surgery group. Specifically, the rerupture-free survival rate at 5 years was 93% for the late-surgery group (>32 days) compared with the early-surgery group, which achieved 97.2%. Similar results were shown for the 14- and 28-day cutoffs, with less robust P values (.02 both) (Figure 3).
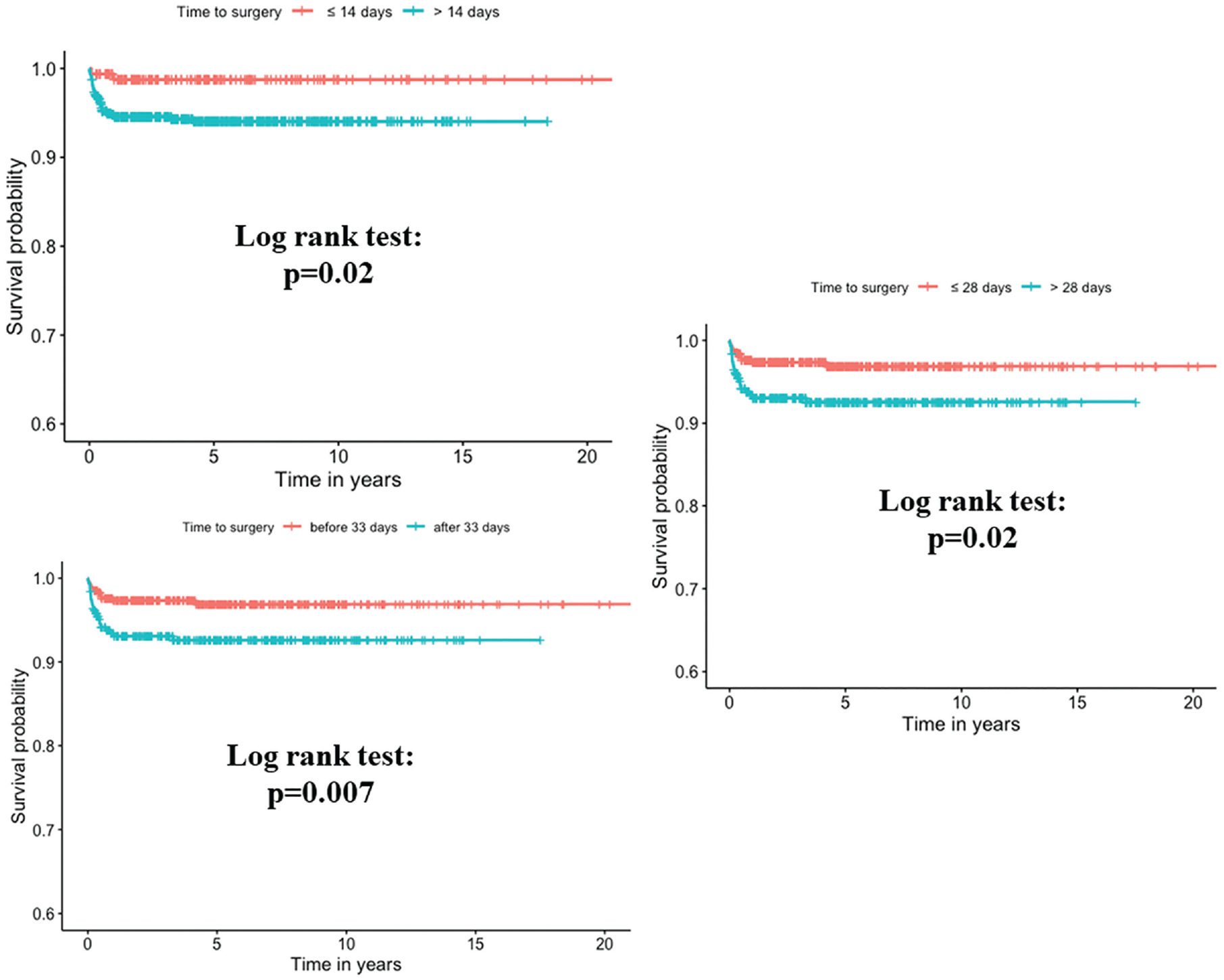
Kaplan-Meier survival curves comparing rerupture-free survival rates based on the 14-, 28-, and 32-day surgery delay threshold.
Final Multivariate Cox Regression Analysis
In the univariate model (Table 2), BMI, time to surgery, type of rupture, and the number of tendons were identified as the potential confounders associated with the outcome (P < 0.10). However, because of a strong correlation observed between type of rupture and number of tendons, only type of rupture was included in the multivariate model to circumvent multicollinearity issues in the Cox analysis. In the multivariate model analysis, 2 key risk factors for rerupture after surgery were identified: an injury-surgery delay >32 days increased rerupture risk by a factor of 2.5 (95% CI, 1.24-5.06; P = .01), and an initial complete rupture presented a 4.33 (95% CI, 1.04-18.08) times higher risk of rerupture compared with a partial one (P = .04) (Table 4).
Multivariate Cox Analysis of Risk Factors for Rerupture After Surgery
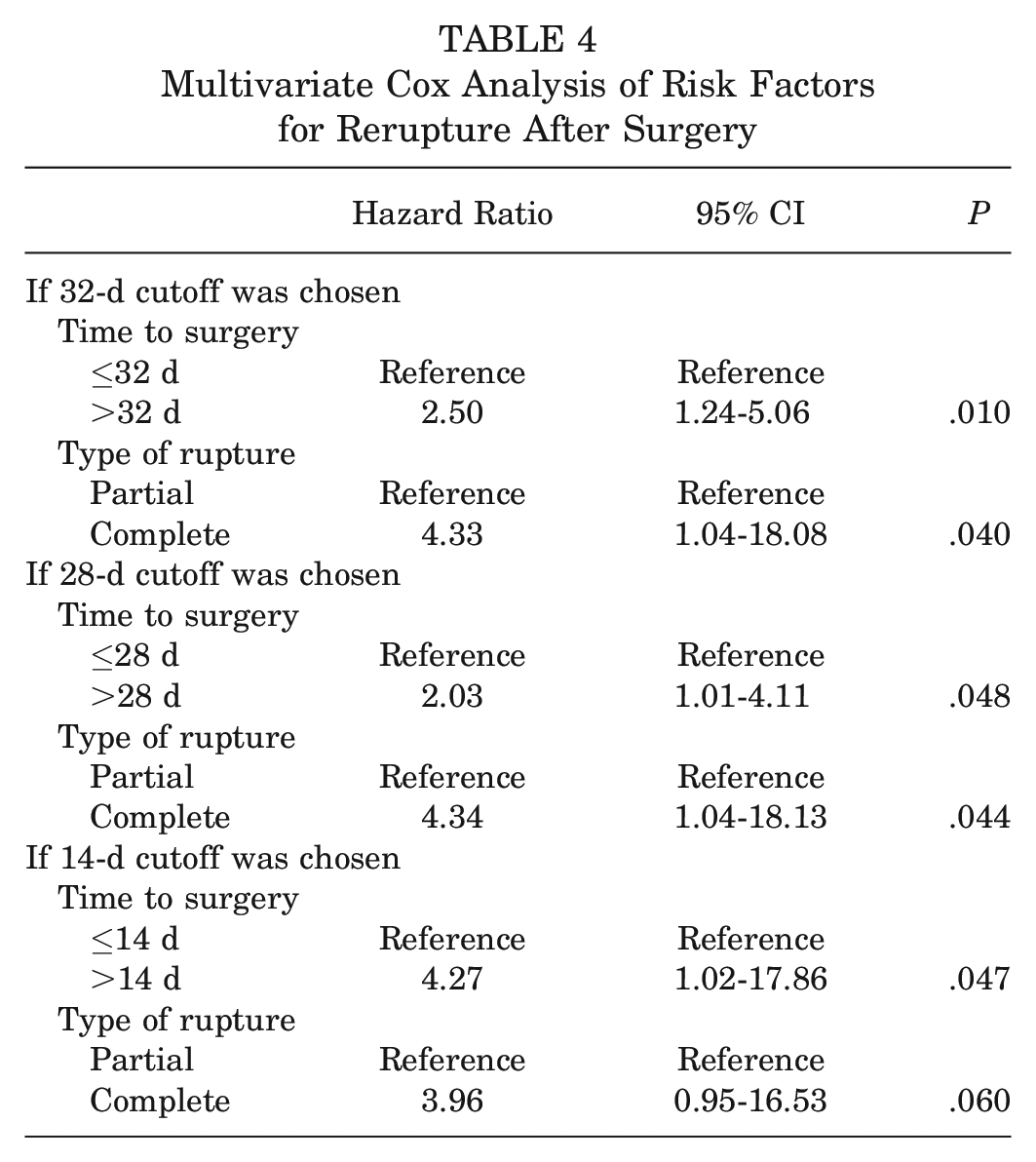
A similar trend was seen when using the 28-day threshold for the analysis, with less robust statistical significance (P = .048 compared with P = .01).
Discussion
This study found a 4.59% rerupture rate after a PHAI repair. The main finding was that a delay >32 days from injury to surgical repair of PHAI significantly increased the risk of rerupture by a factor of 2.5. Furthermore, initial complete ruptures faced a 4.33 times higher rerupture risk versus partial ones.
Rerupture Rate, Timing, and Mechanism
This study showed a recurrence rate of 4.59% after repair of PHAI, with most recurrences occurring in the first 6 months after surgery. These results are consistent with the findings of Lempainen et al., 17 who reported 2 (4.2%) reruptures among the 48 patients with partial PHAIs treated operatively. However, Barnett et al 1 reported a slightly lower rate with 2 confirmed reruptures (1.5%), both of which were associated with chronic injuries. In addition, no reruptures were reported by Blakeney et al 4 or Willinger et al 24 in their respective cohorts of 96 and 94 patients treated operatively. Subbu et al 20 found an 8.3% (2/24 patients) rerupture rate in the delayed repair group (>6 weeks) compared with no rerupture in the early group (78 patients). Nevertheless, these studies are potentially limited because of their relatively small sample sizes and shorter follow-up periods.
When it comes to larger-scale studies, the systematic review by van der Made et al 21 demonstrated a rerupture rate of 3%. Hillier-Smith and Paton 13 reported a rerupture rate of 1.2% at a mean follow-up of 3.2 years for 35 studies and 1530 patients collected up to 2021. Similarly, Jokela et al 14 identified reruptures in 11 (0.69%) of 1602 patients, after collating data from 24 studies in their systematic review. The observed variability of rates could be attributed to heterogeneous follow-up durations and different surgical techniques used in the analyzed studies. Furthermore, the percentage of operatively treated PHAIs that were chronic or complete within each study varied widely. This is especially important as those 2 factors were identified in our multivariate regression analysis as the most important risk factors for rerupture. Another factor influencing the reported rate was the different rerupture definition used in each study. In the systematic review by van Heumen et al, 22 the definition of rerupture varied between studies. This diagnosis was based on MRI scans only, clinical examination, telephone calls, or a combination of these modalities. In our article, we employed a standardized approach to define “rerupture” based on the combination of these modalities, as proposed by van Heumen et al.
Optimal Injury-Surgery Delay
This study established the definition of “chronicity” as an injury-surgery delay exceeding 32 days before undergoing primary intervention. Although the HR for exceeding the 14-day cutoff was 4.79, suggesting a higher rerupture risk, the incidence rate for this group was notably lower than for those surpassing the 32-day cutoff (1.17 vs 1.42 per 100 person-years). Moreover, the 32-day cutoff displayed a narrower confidence interval, providing a more precise estimate of the rerupture risk. Thus, this study defined chronicity as a delay >32 days before primary intervention. The subsequently performed methodological measurements (ROC curve, Cox regression analysis, and Kaplan-Meier curve) reinforced this result. The selection between the 14-day, 28-day, and 32-day cutoffs for predicting rerupture can be debated. The 14-day cutoff, while presenting a higher HR (4.79) compared with the 32-day cutoff (2.56), was accompanied by a significantly larger confidence interval. This limitation was compounded by its comparison involving a considerably smaller number of cases, thus rendering its HR estimation less robust. Furthermore, the extensive confidence interval associated with the 14-day cutoff underscored its instability and imprecision as a predictive threshold. The 28-day cutoff, despite having a narrower confidence interval, demonstrated a lower HR and incidence rate compared with the 32-day cutoff. Similarly, Kaplan-Meier curves and Cox regression analysis incorporating the 28-day cutoff were performed. However, these analyses yielded less robust statistical significance and P values when compared with those derived using the 32-day cutoff.
This threshold fills a substantial gap in the literature concerning the best definition of chronicity, with the vast majority of studies defining it based on assumption. For instance, several studies have adopted a dichotomous categorization based on varied time cutoffs, such as acute (<28 days) versus chronic (>28 days),15,16,25,26 acute (<45 days) versus chronic (>45 days),6,14 and acute (<8 weeks) versus delayed (>8 weeks). 21 Others have proposed a trichotomous classification incorporating an intermediary “delayed” stage, as proposed by Belk et al 2 (thresholds of 4 weeks and 6 months) and Sarimo et al 19 (thresholds of 4 and 12 weeks). The nearest cutoff to our derived 32-day threshold was 30 days, and it was adopted by Harris et al, 12 Best et al, 3 and Bodendorfer et al. 5 Literature reviews have shown that 6 weeks is the most used definition of chronicity.1,18,20,25
Several studies have demonstrated the superiority of acute surgical treatment in terms of functional outcomes, return to sports, and complication rates over the chronic intervention.3,5,7,18,20,25 The systematic review by Hillier-Smith and Paton 13 reported a reduced rate of rerupture when repair is done acutely. Furthermore, a recent study by Wood et al 25 highlighted the fact that acute repairs (<6 weeks) were less technically complex and were associated with a shorter mean operating time (64.67 vs 74.71 minutes; P < .001). In light of these findings, our study used an evidence-based methodology to provide a more objective definition of PHAI chronicity.
Other Risk Factors of Rerupture
Based on our data, complete PHAIs presented a 4.33 times higher risk of failure than did partial ones. Barnett et al 1 reported 2 reruptures, both of which were due to complete tendon avulsion. In their systematic review, Bodendorfer et al 5 did not find a significant difference when comparing complete versus partial tears. However, 12 of the 13 reruptures analyzed were initial complete PHAIs.
Descriptive characteristics, such as age, sex, and BMI, as well as severity of retraction and the number of anchors used, did not significantly contribute to rerupture risk. To the best of our knowledge, the literature currently lacks in-depth examinations of these parameters as potential risk factors for rerupture.
Limitations
Despite its contributions, this study has some limitations. One limitation of our study is the potential bias from consecutive enrollment over 20 years, with evolving rehabilitation protocols and surgeon experience possibly affecting outcomes. However, we believe this effect is minimal because of the few changes and consistency in rehabilitation protocols and surgical techniques. The retrospective nature of the analysis may introduce potential bias; however, all data were collected prospectively, which mitigates the influence of these limitations. Loss to follow-up could affect results, but this was within acceptable limits (8.9%). The sample size may limit generalizability; however, to our knowledge, this series represents the largest in the literature on this topic. Another potential limitation to consider might be the absence of a control group, although this is a common challenge in studies attempting risk factor analysis. Furthermore, it is important to acknowledge that the modest Youden index of 0.24 (sensitivity, 65%; specificity, 59%) and the moderate AUC of 0.62 indicate only a limited predictive accuracy of the 32-day cutoff for rerupture. However, this is completely logical, as the surgical delay is not the only factor implicated. Additionally, the absence of patient-reported outcome measure data is also an area of limitation in the present study; however, our focus remained primarily on rerupture confirmed via clinical and MRI evaluations.
Originality
This study significantly contributes to the existing literature, as it uniquely establishes an evidence-based definition for the chronicity of PHAI. Additionally, it is pioneering in identifying the risk factors associated with rerupture. A key strength of this study is its foundation on the largest patient cohort studied to date, with a long follow-up period. Furthermore, the fact that all patients underwent a standardized surgical technique and adhered to the same postoperative protocol substantially minimizes potential bias.
Conclusion
This study found a 4.59% rerupture rate after a PHAI repair. The risk was found to significantly increase 4.33 times with complete avulsions and 2.5 times with chronic PHAI. The optimal statistical threshold for chronicity of PHAI lesions, based on rerupture rate, is marked by a delay in surgery of >32 days. However, the high HR at 14 days presents a clinically important consideration, indicating the potential advantage of earlier surgical intervention.
Footnotes
Submitted August 11, 2023; accepted December 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. is a consultant for WebSurvey Society, Paris, France. A.H. is a consultant for Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Data Accessibility Statement
Data are available upon reasonable request.