
Abstract
Background:
Proximal hamstring avulsion injuries (PHAIs) are debilitating injuries that can affect long-term quality of life.
Purpose:
To evaluate the long-term functional results of PHAI repair and determine the rate of patient satisfaction and the quality of their return to sport at the latest follow-up.
Study Design:
Prospective cohort study; Level of evidence, 2.
Methods:
This was a prospective cohort study conducted from January 2002 to May 2015. The study targeted all patients undergoing PHAI repair during this time frame, ensuring a minimum follow-up of 8 years. The primary outcome measure used was the Parisian Hamstring Avulsion Score (PHAS). Secondary outcome measures included the University of California at Los Angeles (UCLA) activity scale score and the Tegner activity scale score. A satisfaction survey was administered, the complication rate was assessed, and both the rate and quality of return to sport were analyzed. A subanalysis comparing acute (<4 weeks) versus chronic (>4 weeks) repairs was performed.
Results:
The study involved 139 patients with a mean age of 44.4 years (SD, 11.3 years) and a mean follow-up duration of 123.4 months (SD, 30.8 months). The PHAS at the last follow-up was 87.5 (SD, 14.9). This score was significantly affected by follow-up length (ANOVA-type statistic = 65.40497; df = 4.050724; P < .0002), with post hoc analysis showing lower median scores at 2 years compared with 6 and 8 years (P = .04 and P = .001, respectively) and at 4 years compared with 6 and 8 years (P = .001 and P = .01, respectively). The UCLA activity scale score improved significantly from a preoperative mean of 3.1 (SD, 1.3) to 7.5 (SD, 2.5) at the final follow-up (P < .001). Similarly, the Tegner activity scale score increased from a mean of 1.8 (SD, 1.3) before surgery to 4.5 (SD, 2.1) at the final follow-up (P < .001). Satisfaction was reported by 87.8% of patients. Reruptures were recorded in 11 patients, accounting for 7.9% of the cases. Overall, 80% of the patients returned to the same type of sport postoperatively as before the injury, with 43.5% reaching the same preoperative level. Chronic repairs demonstrated 5.89-fold higher odds of achieving a low PHAS (OR, 5.89; 95% CI, 2.36-17.0; P < .001).
Conclusion:
Surgical repair of PHAI is associated with improved long-term functional outcomes. The PHAS is expected to increase over time until 8 years postoperatively. Chronic repairs carry nearly 6 times higher odds of poor long-term PHAS performance compared with acute repairs.
Keywords
Proximal hamstring avulsion injury (PHAI) is not an uncommon injury and is being increasingly diagnosed in both young and middle-aged patients. 15 The first study reported in the literature dates back to 1988. 21 The rupture is usually caused by a violent eccentric contraction of the hamstring during knee extension and hip flexion.3,4,22 Clinically, a hematoma and ecchymosis extending to the posterior part of the thigh are frequently found. 6 The pain is reproduced by contraction against resistance of the hamstring muscles, often accompanied by a loss of strength on the affected side. 6 Hence, the diagnosis is based on history, clinical examination, and complementary examinations, notably magnetic resonance imaging (MRI), which plays a significant role in the prognostication of this injury by identifying the type, severity, retraction, and involvement of the sciatic nerve.12,24,29
The surgical repair of PHAI has been extensively debated in the literature, with favorable clinical outcomes and improvements in activities of daily living reported.10,23,25 Many studies support that surgical treatment of acute or chronic PHAI has considerably improved the functional prognosis in these patients and the quality of sport resumption in athletic patients, regardless of their levels.8,12,14,19 The optimal timing for surgery is controversial. Some studies have reported similar clinical outcomes in patients with acute or chronic lesions, 9 while others have suggested better outcomes with early surgery.7,8,15,18,19,25 A recent large-scale study determined that patients are best treated in the first months postinjury to reduce the rerupture rate. 19
The various studies in the literature have evaluated mainly the functional results and the quality of return to sport in operated patients in the short and medium term.12,14,28,29 However, few studies, within the limits of our bibliographic research, have studied long-term outcomes.2,28 In a 2022 meta-analysis by Hillier-Smith and Paton, 12 the mean follow-up was 3.2 years among 35 analyzed studies. Similarly, Jokela etal 14 found a follow-up range between 12 and 78 months among 24 analyzed studies. These studies are limited by sample size and follow-up duration, thus failing to address the durability of the outcomes. Large-scale, long-term studies are necessary to assess the durability of functional outcomes along with potential sequelae and evaluate patient satisfaction.
The primary objective of our study was to evaluate the long-term (at least 8 years) functional outcomes of surgical repair of PHAI as measured by the Parisian Hamstring Avulsion Score (PHAS). 20
The secondary objectives were to analyze the complication rate, patient satisfaction, and return to sport at the final follow-up.
Methods
Type of Study and Inclusion and Exclusion Criteria
This was a prospective cohort study from the Proximal Hamstring Avulsion Surgery Cohort Study targeting all patients operated on between January 2002 and May 2015 at a sports surgery referral center in Paris. All patients were >18 years of age. Exclusion criteria included patients who refused to participate, patients with bony avulsion, revision surgery, and surgery necessitating allograft.
Ethical Considerations
The study was approved by the local institutional review board. All patients were informed and gave their consent.
Surgical Indication and Procedure
Surgical interventions were offered for patients with complete PHAI involving both the conjoint and semimembranosus tendons, as well as for patients with partial PHAI involving either tendon when retraction exceeded 2 cm or when 6 months of nonsurgical treatment failed. The diagnosis was based on MRI. The study utilized 2 sources of MRI data. For patients referred to the center with a confirmed diagnosis of PHAI from another medical center, the original MRI data were used and recorded as DICOM files. For patients referred to the center with suspected PHAI, an MRI study was ordered and performed at the center using a GE Healthcare 3-T Signa Architect MRI machine. The analyzed sequences in these MRI studies were mainly axial and coronal T2-weighted sequences. The MRI assessment was performed by an independent musculoskeletal radiologist.
All surgical procedures were performed by senior surgeons (A.H., A.M., Y.B.) who specialized in sports surgery, with the majority of cases treated by one surgeon (N.L.). All surgeries were identical for all patients and followed the technique detailed by Lefevre etal. 16 A short vertical or horizontal incision was made beneath the gluteal crease, directly above the ischial tuberosity. On exposing the superficial aponeurosis, the ruptured tendon stump was revealed, followed by the deeper sciatic nerve. The nerve was protected with or without neurolysis in cases of adhesions, especially in chronic conditions. Then, the tendons were reinserted using 4 anchors and nonabsorbable sutures through the transosseous technique.
Postoperative Management and Rehabilitation
All patients had a similar postoperative protocol. Postoperative immobilization was carried out with the knee in a flexed position (30° in general). Full weightbearing was performed at 4 weeks with continuous use of crutches for up to 6 weeks. The brace was removed between 6 and 8 weeks postoperatively. Functional rehabilitation was started at 6 weeks postoperatively with isometric work of the hamstrings, followed by active work. Active hip flexion was started at 4 weeks. Sport-specific training was initiated at 12 weeks postoperatively with a return to full sports participation between 5 and 8 months.
Outcome Measures
The primary outcome measure was the PHAS, 20 which is a recently validated score to assess functional recovery. The score is a 9-item score with 36 questions, and scores ranging from 0 to 100, with higher scores indicating better outcome.
Secondary outcome measures included the complication rate, particularly the rerupture rate. Different evaluation scores were analyzed, such as the University of California at Los Angeles (UCLA) activity scale score1,30 and Tegner activity scale score, 26 assessed preinjury, the day before surgery, and at the final follow-up.This also included the rate and quality of return to sport. Additionally, the patient’s satisfaction was analyzed. Patient satisfaction was assessed using a binary question: “Do you consider the current condition of your operated leg to be satisfactory?” (Yes/No).
The study also conducted a thorough longitudinal analysis of the main scores collected, specifically the PHAS, Tegner activity scale score, and UCLA activity scale score, at multiple intervals over a 12-year period (2, 4, 6, 8, 10, and 12 years).
Data Collection
Data were collected prospectively through patient responses to questionnaires sent through Websurvey software. This software was accessed also by the surgeon to prospectively fill out the history and physical examination findings, imaging findings, and surgical details.
The data collected included pre- and postoperative descriptive information relating to the characteristics of the treated patients, their comorbidities, associated pathologies, usual sporting and nonsporting activities and profession practiced before the accident, type of typical sports practiced before the accident, history of pain before the injury, history of accident (circumstance, cause, and mechanism), immediate clinical situation and that before intervention, posttraumatic care, preoperative imaging assessment, intervention and surgical technique, complications including iterative ruptures, postoperative examinations, return of sport, and type of sport practiced postoperatively.
Participants and Flowchart
During the study time frame, 151 patients underwent surgery. Of these, 12 were lost to follow-up, leaving 139 patients eligible for subsequent analysis. This group was assessed for complications and rerupture rates. For the functional outcome analysis, 8 patients who experienced rerupture within the study period were excluded. Consequently, the cohort for in-depth analysis of functional outcomes consisted of 131 patients (Figure 1).

Study flowchart.
Statistical Analysis
Frequencies and percentages are used to describe qualitative variables, while mean and standard deviation are used for quantitative variables unless otherwise specified. The comparison between different preoperative UCLA and Tegner activity scale scores (before injury and the day before intervention) and postoperative scores was conducted using the Wilcoxon signed-rank test for paired data.
For evaluating the mean values of the Tegner activity scale score, UCLA activity scale score, and PHAS over time in longitudinal analyses of repeated measures, nonparametric mixed models were used. This approach was chosen due to the nonnormal distribution of scores and the presence of missing data. To assess the effect of time on the scores, we used the ANOVA-type statistic (ATS) from a nonparametric longitudinal data analysis.
A low PHAS was defined as a score below the first quartile of the population distribution. Univariate logistic regressions were performed to identify potential risk factors associated with a low PHAS. Odds ratios and their 95% confidence intervals were estimated to assess the strength of associations between explanatory variables and the likelihood of having a low PHAS.
Kaplan-Meier survival analysis was performed to evaluate the survival probability of rerupture using time in years as the timescale.
When significant effects were found using the nonparametric mixed model, post hoc pairwise comparisons were performed with P values adjusted using the Bonferroni method to account for multiple comparisons.
A P value <.05 was considered statistically significant. All statistical analyses were carried out using R software (Version 4.2; R Foundation for Statistical Computing).
Results
Patient Characteristics
The mean age of patients was 44.9 years (SD, 10.7 years). The tear was acute (<4 weeks) in 46% of cases and chronic (>4 weeks) in 54% of cases. The mean follow-up time was 123.4 months (SD, 30.8 months), with a minimum follow-up of 8 years and a maximum of 20 years. The characteristics of the population in this series are detailed in Table 1.
Patient Characteristics a
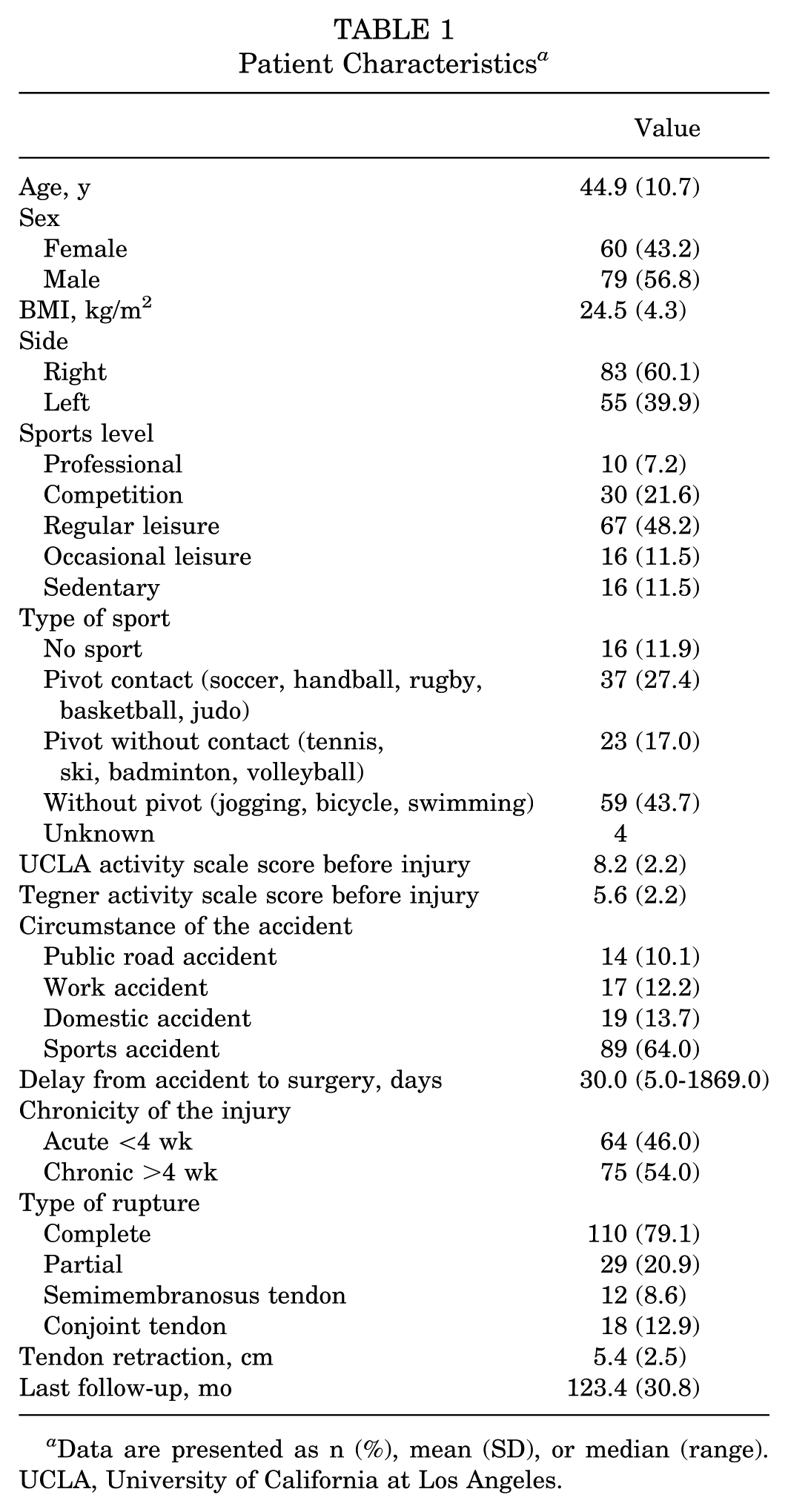
Data are presented as n (%), mean (SD), or median (range). UCLA, University of California at Los Angeles.
Functional Outcomes and Progression of Scores
The functional outcomes and progression of scores are shown in Table 2 and Figure 2.
Comparison of Pre- and Postoperative Activity Scale Scores a
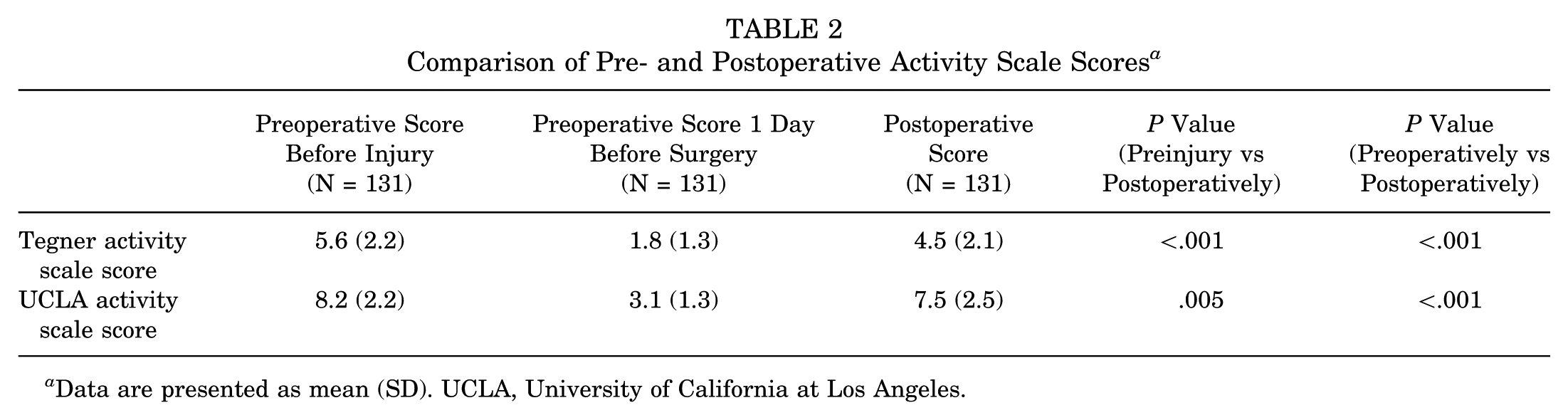
Data are presented as mean (SD). UCLA, University of California at Los Angeles.

Effect of time (in years) on the Parisian Hamstring Avulsion Score (PHAS).
At the final follow-up of 123.4 months (SD, 30.8 months), the mean PHAS was 87.5 (SD, 14.9). This score was impacted by a highly significant effect of time (ATS = 65.40497; df = 4.050724; P < .0002), suggesting that the mean scores varied significantly across different time points. Post hoc analysis indicated that the median score at 2 years was lower compared with scores at 6 and 8 years (P = .04 and P = .001, respectively). Additionally, the median score at 4 years was significantly lower than that at 6 and 8 years (P = .001 and P = .01, respectively) (see Figure 2).
Of note, not all patients completed patient-reported outcome measures at every scheduled follow-up visit. However, all included patients provided data at least at 2 different time points, which satisfies the assumptions required for the longitudinal mixed-model analysis. The numbers of patients contributing outcome data at each follow-up interval were as follows: 45 (34.4%) patients at 1 year, 62 (47.3%) at 2 years, 107 (81.7%) at 4 years, 67 (51.1%) at 6 years, 93 (71.0%) at 8 years, 80 (61.1%) at 10 years, and 47 (35.9%) patients at 12 years.
The mean Tegner activity scale score increased from 1.8 (SD, 1.3) preoperatively to 4.5 (SD, 2.1) at the last follow-up (P < .001). Similarly, the mean UCLA activity scale score increased from 3.1 (SD, 1.3) to 7.5 (SD, 2.5) at the last follow-up (P < .001). However, the last follow-up figures for the Tegner activity scale score were 4.5 (SD, 2.1), lower than the preinjury score of 5.6 (SD, 2.2) (P < .001). There was no effect of time on this outcome (P > .05) (Figure 3).

Effect of time (in years) on the Tegner activity scale score.
Similarly, the UCLA activity scale score at the last follow-up was 7.5 (SD, 2.5), lower than the preinjury score of 8.2 (SD, 2.2) (P < .001). There was no effect of time on this outcome (P > .05) (Figure 4).

Effect of time (in years) on the University of California at Los Angeles (UCLA) activity scale score.
Return to Sport
Return-to-sport data are provided in Tables 3 and 4.
Return to Sport and Satisfaction at the Last Follow-up a

Data are presented as n (%).
Return to Sport by Type and Level of Sport a
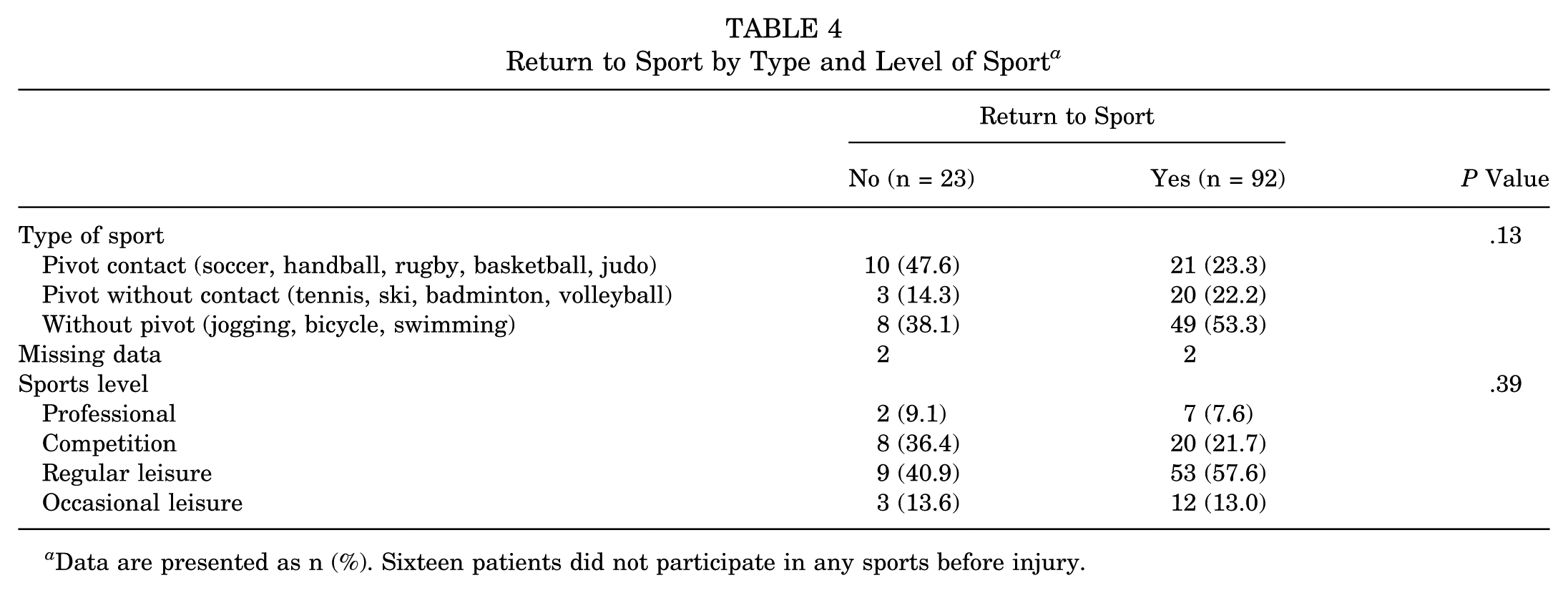
Data are presented as n (%). Sixteen patients did not participate in any sports before injury.
After at least 8 years of follow-up, 92 (80%) participants resumed the same sport as before their injury. Among these, 40 (43.5%) returned at the same level, 49 (53.3%) at a superior level, and 3 (3.3%) at a lower level. Conversely, 23 (20%) participants did not resume the same sport, with 11 (47.8%) ceasing to engage in sports altogether and 12 (52.2%) switching to different sports. The main reasons for stopping or changing sports included personal reasons (13 individuals, 56.6%) and issues related to the hamstring injury (10 individuals, 43.5%).
Satisfaction with the condition of the operated leg was high, with 115 (87.8%) participants reporting it as satisfactory.
Rerupture Rate and Complications
The rerupture rate in these patients was 7.9% (11/139 patients). Eight of them were reoperated, while the remaining 3 were treated nonoperatively.
The mean time to repair failure was 73 days (range, 1 day–11.84 years) (Figure 5). The early rerupture observed on the first postoperative day occurred after an accidental traumatic event (a fall at home) unrelated to the surgical procedure itself.
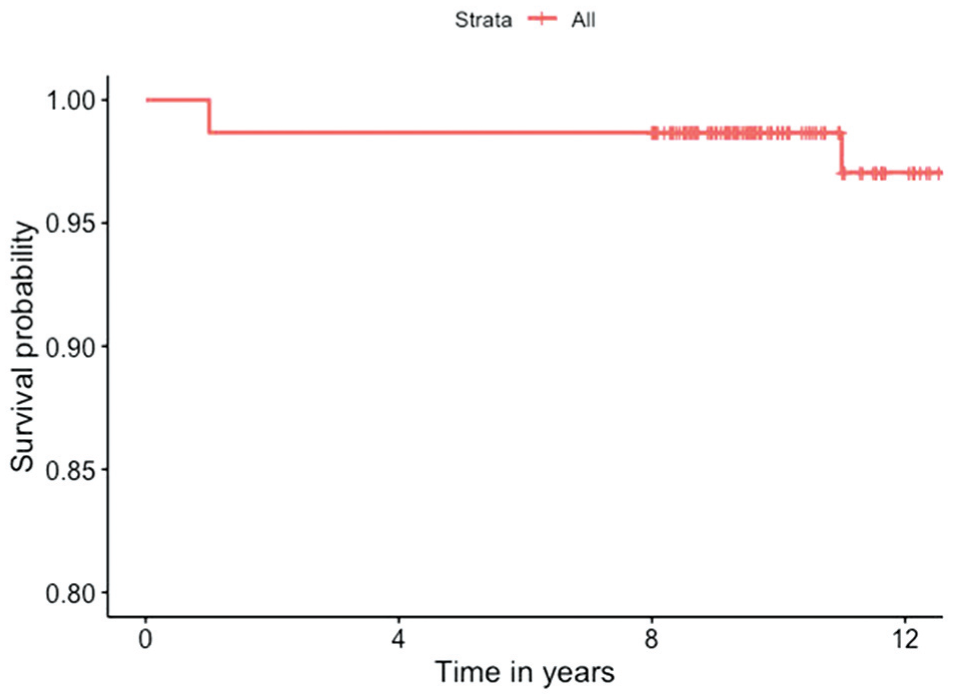
Kaplan-Meier curve.
Concerning the rate of other complications observed in these patients, 4.3% had a postoperative hematoma, 4.3% paresthesia at the sciatic nerve territories, 2.2% posterior cutaneous paresthesia of the thigh, and 0.7% postoperative pudendal nerve paresthesia (Table 5). All cases of sensory deficit were transient and resolved spontaneously within 3 to 6 months postoperatively. None required surgical revision or neurolysis. Pain during prolonged sitting at the final follow-up was reported as follows: 81 (61.8%) patients had no pain, 30 (22.9%) had mild pain, 12 (9.2%) had moderate pain, 7 (5.3%) had severe pain, and 1 (0.8%) patient reported extreme pain, making the activity impossible.
Complication Rate of the Surgical Intervention Within the Study Period a
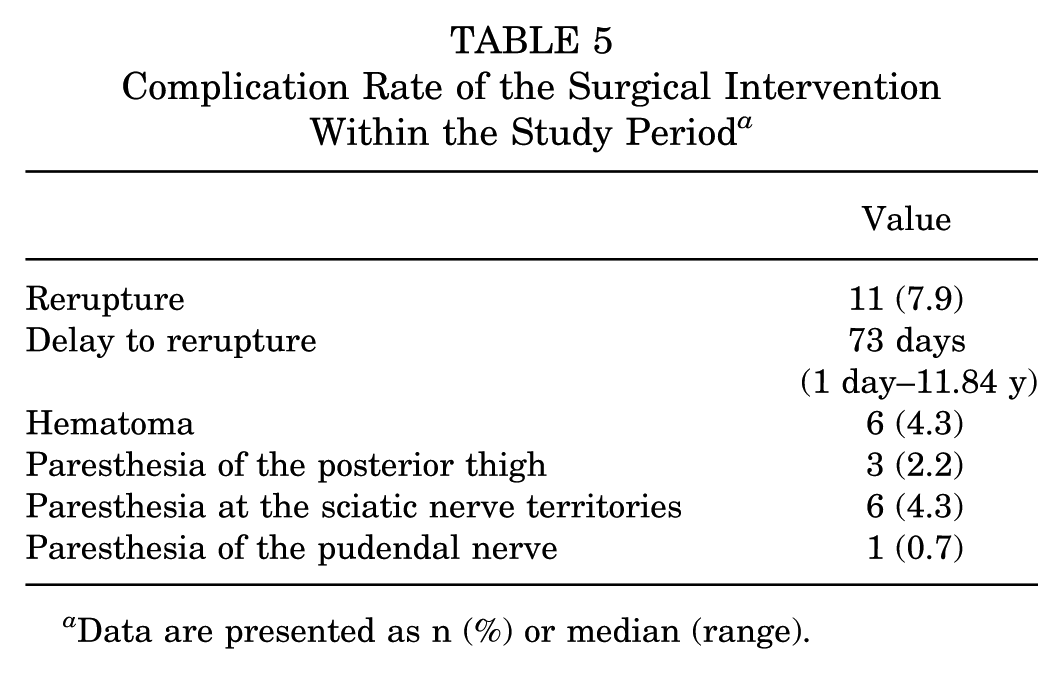
Data are presented as n (%) or median (range).
Risk Factor Analysis
The risk factor analysis results are shown in Table 6.
Univariate Logistic Regressions to Identify Potential Risk Factors for a Lower PHAS (<81.3) a

Bold values indicate statistical significance. BMI, body mass index; PHAS, Parisian Hamstring Avulsion Score; ref, reference; UCLA, University of California at Los Angeles.
The first quartile (Q1) for the PHAS in the cohort was 81.3/100, and any score below this threshold was classified as a “lower PHAS.” The univariate logistic regression analysis demonstrates that chronic injuries (>4 weeks) were significantly associated with a higher risk of a lower PHAS (OR, 5.89; 95% CI, 2.36-17.0; P < .001). Patients with higher preinjury UCLA activity scale scores werefound to have a lower likelihood of obtaining a low PHAS (OR, 0.80; 95% CI, 0.67-0.96; P = .017). Similarly, sport-related injuries, as opposed to public road accidents, were associated with a reduced risk of a poor PHAS outcome (OR, 0.24; 95% CI, 0.07-0.83; P = .022)
Discussion
The main finding of this study was that surgical treatment of PHAI is associated with time-lasting functional outcomes at the last follow-up, as demonstrated by a high PHAS. This score is expected to increase over time until 8 years postoperatively.
When compared with a recent matched comparative study from the same PHAS cohort, Lefèvre etal 21 reported mean PHAS values of 86.3 (SD, 13.7) in the surgical group and 69.8 (SD, 15.1) in the nonsurgical group, at a mean follow-up of 50.7 months (approximately, 4.2 years). That study demonstrated a statistically significant benefit of surgical treatment over nonsurgical approaches across multiple outcomes, including the PHAS, UCLA activity scale score, and Tegner activity scale score, as well as return to sport and patient satisfaction. 21 Our study reported a similar mean PHAS of 87.5 (SD, 14.9) at a longer mean follow-up of 123.4 months (approximately 10.3 years). This reinforces the long-term functional durability of surgical repair and supports the sustained value of operative management in PHAI, beyond the midterm horizon.
According to a systematic review by Jokela etal, 14 there are only 3 studies in the literature with >50 months of follow-up.2,5,28 For instance, Arner etal 2 explored the midterm outcomes of PHAI (mean follow-up, 6.5 years; range, 2-12.5 years). They studied 64 patients with partial PHAI treated surgically. The results showed a mean postoperative Lower Extremity Functional Score of 96%, and the mean total proximal hamstring score was 94%. Furthermore, the authors reported high patient satisfaction, with 97% of patients satisfied with the surgery, 92% able to participate in strenuous activity, and 97% estimating their strength to be >75% that of their contralateral side. 2 Our study demonstrated slightly lower satisfaction rates at 87.8% at the last follow-up.While the figures are relatively close, the decline in satisfaction rates might be attributed to factors such as time, the technique of collecting outcomes, and the mode of survey administration. In our study, this outcome was collected via web survey software, which may have led to responses not being influenced by the presence of surgeons. This provides another perspective on satisfaction at long-term follow-up after PHAI surgery; the functional scores remained consistently high, while a slight decrease in satisfaction may occur over time. This is noteworthy compared with another midterm study by Barnett etal, 5 who reported a similar rate of satisfaction. In their study, 84.4% of patients rated their results as good or excellent at a mean follow-up of 53.8 months (SD, 19.5 months). The authors did not report postoperative scores but instead measured objective hamstring strength and endurance, finding mean values of 83% and 108%, respectively, as measured by isotonic muscle quantification.
Return to Sport and Activity Level
The rate of return to sport in our study (80%) is relatively high, considering the level of sports participation among the participants, with >50% involved only in occasional and regular leisure activities, and a smaller percentage being competitive or professional sportsmen. Various studies on the return to sport after surgical repair of PHAI have shown variable rates (between 76% and 100%), but the number of patients reaching the same level as before the injury was lower (between 50% and 78.1%).11-13,16,17,22,29
The minor decline in long-term activity scores likely reflects the natural effects of aging and time rather than a direct consequence of the surgical procedure.
Rerupture
In our study, the most common postoperative complication identified was rerupture, occurring in 7.9% of cases. This rate is slightly higher than that reported in the literature. Van der Made etal, 27 in a systematic review of 13 studies including 387 patients, reported a rerupture rate of 3%. Lefèvre etal 19 reported a rate of 4.59%. 19 The rerupture rate was 3.8% in the Folsom 10 series, 1.4% in the Wood 28 series, and 1.3% in the systematic review by Hillier-Smith and Paton. 12 Sarimo etal, 25 in their series of 41 acute and chronic ruptures, found 5 (12.2%) cases of iterative ruptures. While most reruptures occur during the first year postoperatively, as demonstrated by Lefèvre etal, 19 the longer follow-up duration in our study may in part explain this higher number.
Originality and Limitations
The originality and strengths of this study lie in the large number of patients involved and a mean follow-up time of 123.4 months (SD, 30.8 months), which stands out as the longest duration to the best of our knowledge. Furthermore, this is one of the few studies that investigated the progression of functional outcomes over time.
However, there are several weaknesses in this study. The absence of a control group and the inclusion of a heterogeneous population with a mix of acute and chronic repairs are significant limitations. Additionally, the data collection was based on subjective questionnaires without objective strength analysis. A notable limitation of this study is the presence of missing data for some repeated measures. Not all patients completed every questionnaire at each follow-up interval. However, the use of mixed models helps account for these missing data points.
Conclusion
This study demonstrates satisfactory long-term results of surgical repair of PHAI, in terms of both functional prognosis and return to sport, at the same previous level, in a large cohort of patients with a minimum follow-up of 8 years. The PHAS is expected to increase over time, until 8 years postoperatively. Chronic repairs carry nearly 6 times higher odds of poor long-term PHAS performance compared with acute repairs.
Footnotes
Final revision submitted November 30, 2025; accepted December 6, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. has received consulting fees from Websurvey Society. A.H. has received consulting fees from Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of University Hospital Pitié Salpétrière (CPP IDF VI).